-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Prevention and Treatment
p-ISSN: 2167-728X e-ISSN: 2167-7298
2022; 10(1): 1-3
doi:10.5923/j.ijpt.20221001.01
Received: Sep. 18, 2022; Accepted: Sep. 28, 2022; Published: Oct. 21, 2022

The Stage at Diagnosis of Patients with Esophageal Cancer at Moi Teaching and Referral Hospital, Eldoret Kenya
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLTabitha Chepkemoi
Kabarak University, Kabarak, Kenya
Correspondence to: Tabitha Chepkemoi, Kabarak University, Kabarak, Kenya.
| Email: |  |
Copyright © 2022 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

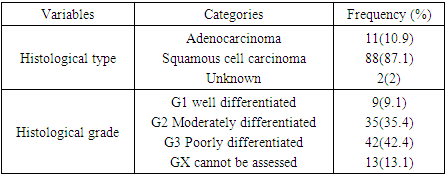
Esophageal cancer staging is an important determinant of prognosis. Staging helps the physicians in determining the best treatment approach for their patients. The aim of the study was to document the stage at diagnosis of esophageal cancer at Moi Teaching and Referral Hospital MTRH, Kenya. A cross-sectional study was done where the medical records of patients with esophageal cancer were reviewed and the stage of the cancer, histological type and grades retrieved. Semi- structured questionnaire was also used to interview patients on their socio-demographic characteristics. A total of 104 patients were interviewed and their files reviewed. Descriptive statistics was done using R-4.1.0-win, where percentages of cancer stages, histological type, and grades were calculated, for continuous variables, mean was used. A majority of participants 87.1% were diagnosed with squamous cell carcinoma. On histological grading, 42.4% were at G3, poorly differentiated. The study revealed that esophageal cancer is common among the older population, and males are more affected than females. Squamous cell carcinoma (SCC) accounted for higher esophageal cancer cases in the population than adenocarcinoma (ADC). A large proportion of patients are diagnosed at an advanced stage of esophageal cancer.
Keywords: Esophageal cancer, Cancer staging, Squamous cell carcinoma, Adenocarcinoma, Cancer grading, Esophageal cancer diagnosis, and esophageal cancer treatment
Cite this paper: Tabitha Chepkemoi, The Stage at Diagnosis of Patients with Esophageal Cancer at Moi Teaching and Referral Hospital, Eldoret Kenya, International Journal of Prevention and Treatment, Vol. 10 No. 1, 2022, pp. 1-3. doi: 10.5923/j.ijpt.20221001.01.
Article Outline
1. Introduction
- Of all the esophageal cancer incidence and deaths globally, 80% occur in low and middle -income countries meaning that they bear the greatest burden of the disease as compared to high- income countries [1]. Esophageal cancer causes the highest number of cancer-related deaths in Kenya killing over 4,000 people annually [2].The stage at diagnosis of esophageal cancer is a key predictor of the overall outcome of the disease; it helps clinicians to select the modalities of therapies and to evaluate the success of the therapy to the patients. Late presentation and diagnosis lead to poor outcomes and high cost of treatment. The Late presentation for diagnosis constitutes stages 3 and 4 which in most cases are advanced and difficult to manage [3]. Early diagnosis of esophageal cancer is a crucial goal because it gives opportunity for early initiation of treatment which may improve prognosis and allow cure to be achieved. It is presumed that most esophageal cancer patients present late for diagnosis but there is limited documentation in Kenya on the same. Therefore, the aim of the study was to document the stage at diagnosis which could be very useful for policymakers and those managing esophageal cancer.
2. Materials and Methods
- Study design: The study was a cross-sectional which involved interviewing of the patients using a semi- structured questionnaire to get socio-demographic characteristics and reviewing of their medical records to retrieve information on cancer stage and other clinical characteristics.Sample size determination and Sampling techniques: A sample size of 104 patients was arrived at using the formula for the finite population (Daniel 1999). Patients were recruited using consecutive sampling until the targeted sample size was achieved. Data collection techniques: At the oncology and cardiothoracic clinics, the researcher started from the clinician desk to check on the registers for the patients who were identified as having esophageal cancer. Their names were written down and then they were approached physically on the waiting bay to give consent for the researcher to peruse through their files and to be interviewed. For those who met eligibility criteria, the researcher retrieved the information on clinical data from their files then proceeded to interview them on socio- demographic characteristics.Stage determination: Esophageal cancer staging is usually done by the clinician before the initiation of treatment to the patients and in most cases the stage is documented in the patients’ file. The researcher therefore, obtained the stage at diagnosis from the patients’ file. At MTRH, the system used for staging esophageal cancer is TNM (Tumor- Node- Metastasis) where the assessment of the tumor is done in the following three ways, Tumor- depth of tumor invasion, Node-involvement of regional lymph nodes, and Metastasis- the presence or absence of metastatic disease, after knowing the TNM of the patient, the stage is then assigned as either 0, I, II, III, or IV.The initial test that is commonly used to identify and diagnose esophageal cancer is upper GI endoscopy with biopsy. The test shows the location and length of the tumor and the biopsy taken is used for pathological examinations.A CT scan of the chest and abdomen can also be done to identify the spread of the disease to the lungs and the liver or endoscopic ultrasound to establish the depth of tumor invasion and the extent of lymph nodes involvement.Data management and analysis: All the data captured was counter checked and entered into MS Excel. Data was then exported to R-4.1.0-win software for analysis. Descriptive statistics were summarized in frequency, means with standard deviations, and percentages. Ethics: The study sought ethical approval from the Institutional Research and Ethics Committee (IREC) of Moi University, IREC/2019/288. Informed written consent was obtained from all the eligible participants and those who consented were interviewed.
3. Results
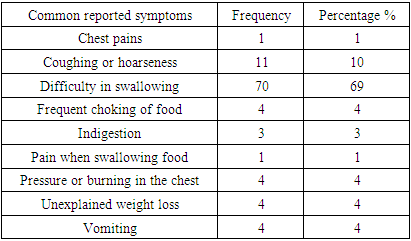
- Majority of participants had stage IV (45.5%) and III (33.7%), (advanced stage) at the cancer diagnosis while Stages, 0, I, II accounted for 20.8%, (early stages), Figure 1. On the esophageal cancer histological type and histological grade, a majority of participants 87.1% were diagnosed with squamous cell carcinoma, on histological grading, 42.4% were at G3, poorly differentiated. Table 2. 69% of the participants reported difficulty in swallowing as the most common symptom for esophageal cancer. Figure 2. Participants were asked what they thought about their symptoms and out of 102, 53% thought that the symptoms were not serious to necessitate urgent attention. Of importance to note are 30% who were afraid and worried of the symptoms.
|
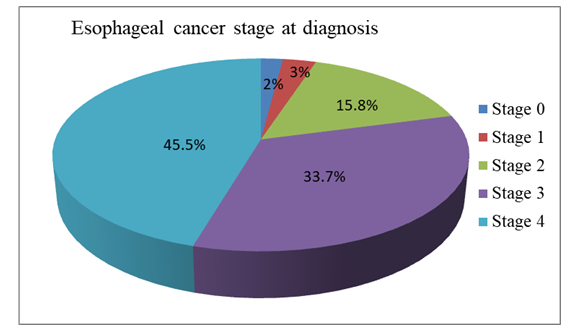 | Figure 1. Pie chart showing the percentages of stage at diagnosis |
|
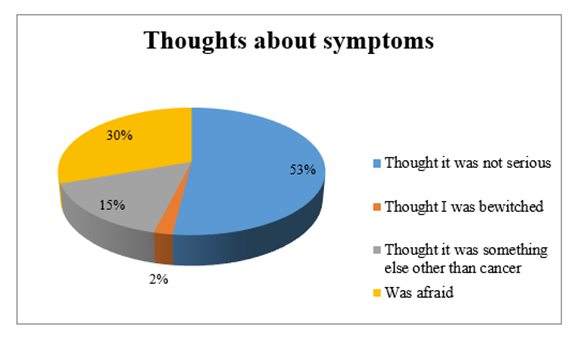 | Figure 2. Thoughts about the experienced esophageal symptoms |
4. Discussion
- The Stage at Diagnosis: The study revealed that a majority of the participants (79.2%) were diagnosed at an advanced stage (stage III and IV). The results were however, slightly lower than those found by a study done in Thailand that revealed that nearly all the patients with esophageal cancer (94.5%) presented with late-stage disease. Another study done at KNH showed that 89% of their participants were diagnosed at stage III and IV [4,5]. The delays may have risen in different steps from the time the patients presented for the first time to the health facility through to the process of diagnosis which allowed the cancer to advance.Clinical characteristics: Squamous cell carcinoma (SCC) accounted for higher esophageal cancer cases in the population than adenocarcinoma (ADC). These results were consistent with other published reports, where SCC is widely dominant over ADC [6,7]. In terms of grading, a majority of the participants fell under Grade II (moderately differentiated) and Grade III (poorly differentiated) which meant cancer cells were somewhat to very abnormal. Symptoms: The study revealed that dysphagia, unexplained weight loss, pain, pressure or burning in the chest and vomiting were the most common presenting symptoms for esophageal cancer as observed by other previous studies. Dysphagia is the most disturbing symptoms resulting from esophageal obstruction as it leads to poor nutrition, pain and compromised quality of life [8,9,10].Thoughts about the experienced symptoms: The perception of one’s symptoms would influence the time for presentation to the health facility. From our findings, 52% of the participants thought their symptoms were not serious enough to warrant an urgent medical attention and this could explain the late presentation among the 59.8% of the participants. Fear has been found to be a contributing factor to late presentation because it acts as a barrier to an individual seeking medical attention and the thought of being diagnosed with a cancer has been found to cause anxiety and stigma.
5. Conclusions
- A large proportion of patients are diagnosed at an advanced stage of esophageal cancer at Moi Teaching and Referral Hospital. Squamous cell carcinoma is the most occurring type of esophageal cancer. Dysphagia is the most presenting symptom for patients with esophageal cancer. The public should be educated on the importance of early presentation and diagnosis since it could provide a window for esophageal cancer treatment.
ACKNOWLEDGEMENTS
- We express our sincere gratitude to God for the strength, Moi Teaching and Referral Hospital administration for the permission to access patients’ medical records and the School of Public Health Moi University for academic guidance.
DISCLOSURE
- Competing interestsThe authors declare no competing interest.