Ireye Faith1, Ejiyere Harrison1, Aigbiremolen Alphonsus O.1, 2, Famiyesin Olubowale Ekundare1, Rowland-Udoh Eloho A.2, Ogeyemhe Charles O.2, Okudo Ifeanyi1, Onimisi Anthony B.1
1World Health Organization, Nigeria
2Cedar Centre for Health and Development, Ekpoma, Nigeria
Correspondence to: Ireye Faith, World Health Organization, Nigeria.
| Email: |  |
Copyright © 2019 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Good adherence to standard precautions and infection prevention and control (IPC) practices in healthcare settings has been identified as an important factor in the control of potential outbreaks of Lassa fever within the hospital setting. Poor health care workers’ (HCWs) knowledge of the disease and infection control techniques is a major contributing factor to hospital-acquired Lassa infection. A cross sectional study to assess the knowledge, attitude and IPC practices was conducted among 294 HCWs in Edo State, Nigeria. Data was collected using an interviewer-administered questionnaire and the assessment was done using defined scoring systems. Data was analyzed using SPSS version 21. Associations between variables were assessed using Chi-square test with a significance level set at p<0.05. The proportions of respondents with good knowledge, good attitude and good IPC practices among HCWs were 4.4%, 63.3% and 41.2% respectively. Type of facility and cadre of HCW were significantly associated with knowledge of IPC. IPC practices were found to be poor among over 50% across all cadres of study participants. Type of facility, cadre and duration of work were all significantly associated with practice of IPC. Majority of health workers had fair knowledge of and good attitude towards Lassa fever prevention and control. Conclusively, this study found that IPC practices were generally poor among HCWs in the study area. Information, education and communication on Lassa fever prevention and control should be enhanced and sustained in all public and private health facilities across Edo State.
Keywords:
Lassa fever, Infection prevention and control, Health care worker, Edo State
Cite this paper: Ireye Faith, Ejiyere Harrison, Aigbiremolen Alphonsus O., Famiyesin Olubowale Ekundare, Rowland-Udoh Eloho A., Ogeyemhe Charles O., Okudo Ifeanyi, Onimisi Anthony B., Knowledge, Attitude and Infection Prevention and Control Practices Regarding Lassa Fever among Healthcare Workers in Edo State, Nigeria, International Journal of Prevention and Treatment, Vol. 8 No. 1, 2019, pp. 21-27. doi: 10.5923/j.ijpt.20190801.03.
1. Introduction
Lassa fever has accounted for the deaths of a number of HCWs since its discovery in a northern Nigerian town in 1969. [1, 2] It has resulted in the loss of quality healthcare manpower across many cadres in the health workforce. [3, 4]. Unfortunately, within health care setting, the transmission of the disease is promoted by non-adherence to standard precautions and poor infection prevention and control (IPC) practices. Adherence or non-adherence to IPC measures in healthcare settings has been identified as an important factor to be considered in the control potential outbreaks of Lassa fever. [5] Contributing factors to hospital-acquired Lassa infection include poor knowledge of the disease and poor knowledge of infection control techniques on the part of the health facility personnel among others. In support of this, studies have shown that transmission of Lassa virus is minimal in hospitals with improved IPC practices. [6]In Nigeria, the 2012 Lassa fever outbreak recorded 623 cases including 70 deaths reported from 19 out of the 36 states in the country. Three doctors and four nurses were reported to be among the fatalities. [7] Furthermore, between August 2015 and May 2016, the World Health Organization (WHO) was notified of 273 cases of Lassa fever reported from 23 states in Nigeria. These included 149 deaths and of these, ten cases were health care workers (HCWs) and four were hospital acquired infections. [2, 7] As at 3rd June, 2018, 181 out of the 432 (42%) confirmed Lassa fever cases were from Edo State and 13 of these were HCWs. [8]Lassa virus is fast gaining prominence as an emerging nosocomially transmitted pathogen with significant public health impact in the West African sub region. The most important mechanism of spread of this pathogen is via the contaminated hands of the healthcare givers or relatives/friends of the patients. [9, 10] Contaminated environmental surfaces, drugs, intravenous solutions or foodstuffs are all potential sources of infection [9, 10] In view of the above, the transmission of Lassa fever in healthcare facilities represents a significant burden on the healthcare system [2, 11] and a potential for sporadic outbreaks in different parts of the country. This study set out to assess the knowledge and practice of infection prevention and control (IPC) among health care workers in Edo State, a state known to be endemic for Lassa fever in Nigeria. A study of this nature is therefore imperative and timely given the fact that implementation of its recommendations will promote good IPC, healthcare service delivery and health workers safety with regards to the management of Lassa fever and other potential hospital-acquired infections.
2. Methodology
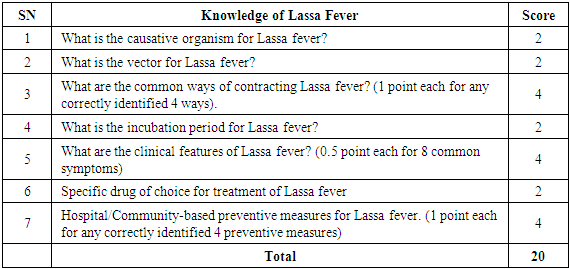
Study design: We conducted a descriptive cross sectional study among health care workers (HCWs) in selected LGAs of Edo State in 2018.Sample size determination: The sample size of 290 was calculated using the Cochran formula for cross sectional studies where the minimum sample size, n= Z2pq/d2. [12, 13] The prevalence, p, used in the calculation was the prevalence of good knowledge of Lassa fever from a similar study done previously in Edo State. [4]Study area: Edo State is divided into 3 senatorial districts made up of various Local Government Areas (LGAs). One LGA was selected from each of the three senatorial districts of Edo State. Two LGAs (Esan West and Etsako West) were selected purposively because they recorded the highest frequencies of cases of Lassa fever in Edo Central and Edo North Senatorial District during the 2018 Lassa fever outbreak in Edo state. A third LGA, Egor, was further selected by simple random sampling technique from among LGAs in Edo South senatorial district.Study population: The study was conducted among HCWs who have been working in selected public and privately-owned health facilities in the selected LGAs prior to the commencement of this study. Sampling: This involved a sampling of healthcare facilities (both government and privately-owned) selected by simple random sampling technique and questionnaires administered to their HCWs in the selected LGAs until the required sample size was attained.Data collection: Data for this study was collected in August/September, 2018. The instrument of data collection was a semi-structured questionnaire administered to HCWs to assess their knowledge and attitude on Lassa and their practice of IPC.Data management: Data was entered and analysed using Statistical Package for Social Sciences (SPSS) version 21. The questionnaires captured information on socio-demographic variables and information on Lassa fever. Knowledge of Lassa fever was assessed using a 20-point scoring system on basic knowledge of the aetiology, disease vector, mode of transmission, clinical features, drug treatment and preventive measures against Lassa fever (Box 1). A score of less than 10 was assessed as poor knowledge; 10-14 was assessed as fair knowledge while a score of ≥15 was assessed as good knowledge. Box 1. Knowledge assessment for Lassa fever
 |
| |
|
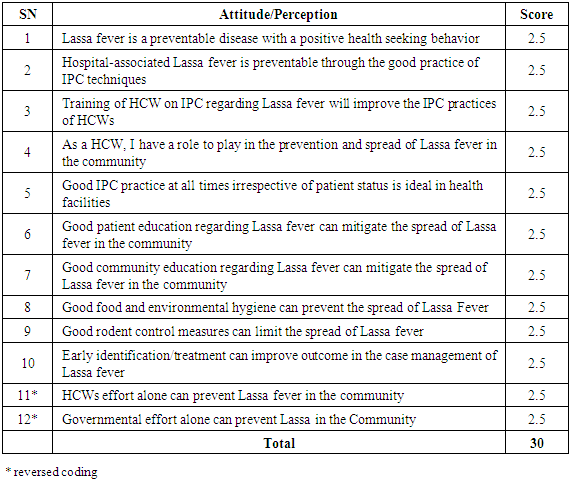
The attitude and perception on preventive practices were assessed using a 30-point scoring system made up graded responses to specific preventive measures on a 5-point Likert scale (Box 2). The responses were graded as follows: 2.5 = strongly agree, 2.0 = Agree, 1.5 = Not sure, 1.0 = Disagree and 0.5 = strongly disagree in ten out of twelve attitude/perception parameters while the coding was reversed for the last two of the parameters (that is, 0.5 = strongly agree, 1.0 = Agree, 1.5 = Not sure, 2.0 = Disagree and 2.5 = strongly disagree). A cumulative score of less than 15 was assessed as poor attitude/perception; 15 – 22.49 was assessed as fair attitude/perception while a score of ≥22.5 was assessed as good attitude.Box 2. Attitude/perception assessment for Lassa fever
 |
| |
|
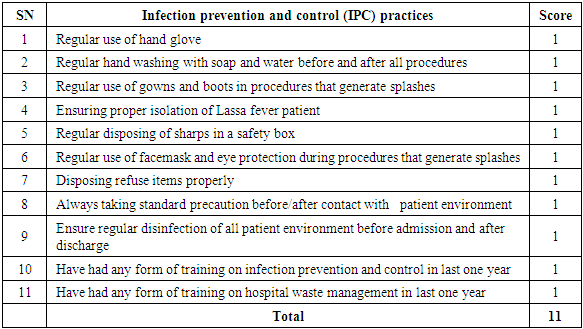
The practices of IPC measures among healthcare workers who participated in the study were assessed and graded using an 11-point scoring system with a point for each of the under-listed activities in the course of patient care (Box 3). A score of less than 6 was graded as poor IPC practice; 6 – 8 was graded as fair IPC practice while a score of 9 – 11 was graded as good IPC practice.Box 3. IPC Practice assessment for Lassa fever
 |
| |
|
Results were presented in frequencies, proportions and percentages. Statistical significance of association between variables was assessed using Chi-square test with significance level set at p<0.05.Ethical considerations: Informed consent was obtained from the heads of all selected healthcare facilities and respondents that participated in the study. Participation was voluntary and there was no consequence for non-participation. All information obtained was kept confidential.
3. Results
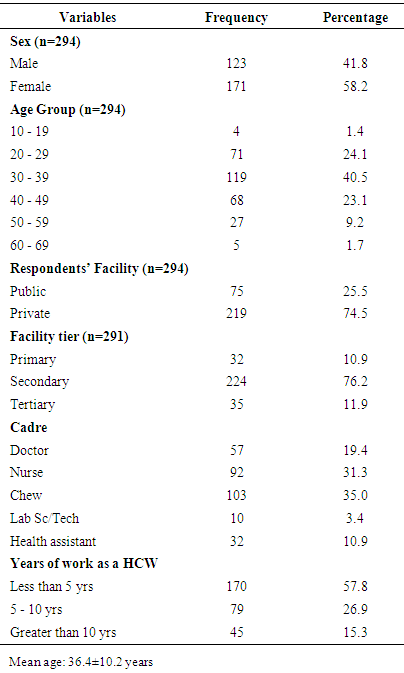
Socio-demographic characteristics of Participants (Table 1)A total of 294 HCWs participated in the study. More female (58.1%) participated in the study than males (41.8%). A higher proportion of the respondents (74.5%) were HCWs working in privately- owned health facilities while a lesser proportion (25.5%) working in government-owned health facility. Majority (76.2%) of respondents were workers in secondary health care facilities. More of the respondents were in the age-groups of 20 – 29 years, 30 – 39 years and 40 – 49 years as the proportion of participants in these age-groups were 24.1%, 40.1% and 23.15% with a mean age of 36.4 ± 10.2 years. The nurses and community health extension workers (CHEW) accounted for a higher percentage of the participants having 31.3% and 35.0% respectively. The medical doctors made up 19.4% of the study participants.Table 1. Socio-demographic characteristics of respondents
 |
| |
|
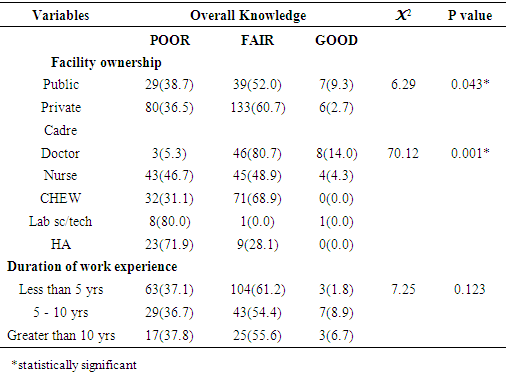
Knowledge of Lassa fever among respondents (Figure 1 and Table 2)An assessment of the overall level of knowledge among respondents showed that the proportions having good knowledge, fair knowledge and poor knowledge were 4.4%, 58.5% and 37.1% respectively (Figure 1). Over 50% of respondents working in both privately-owned and government facilities had fair knowledge of Lassa fever. The differences in knowledge between participants working in both privately-owned and government facilities and between different cadres of health care workers were found to be statistically significant (X2= 6.29, p= 0.043; and X2= 70.12, p= 0.001 respectively). There was no statistically significant difference in the knowledge of HCWs based on the number of years they have worked for.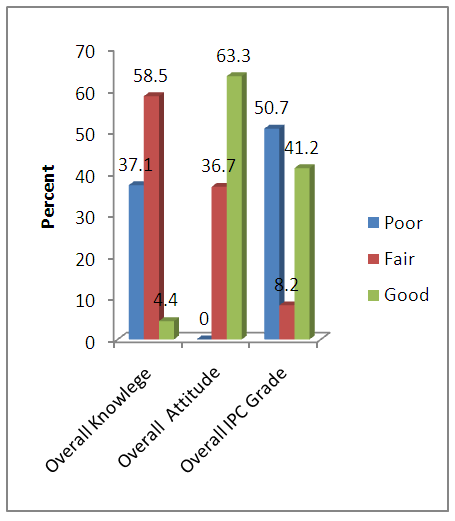 | Figure 1. Percentage performance grades of respondents in knowledge, attitude and IPC practicess |
Table 2. Knowledge of respondents regarding Lassa fever
 |
| |
|
Attitude and perception of Lassa fever among respondents. (Figure 1 and Table 3)The level of attitude/perception was generally good (63.3%) among all categories of HCWs (Figure 1) and even high in many participants as over 90% of doctors and almost 90% of nurses had good attitude towards prevention of Lassa fever. The CHEWs had almost 90% of fair attitude among those that participated in the study. Over 88% of participants who had worked between 5 and 10 years and over 90% of workers who had worked for over 10 years had good attitude towards the prevention of Lassa fever. These findings were all found to be statistically significant among participants.Table 3. Attitude of respondents regarding Lassa fever
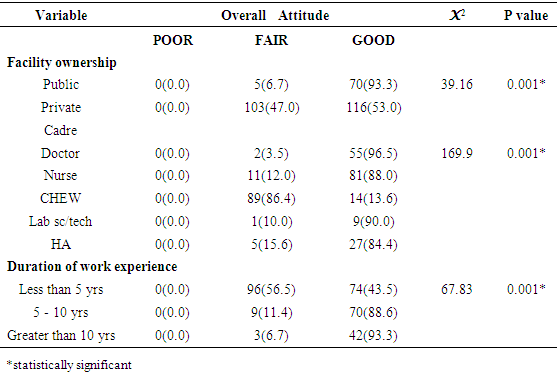 |
| |
|
Infection prevention and control practices among respondents (Figure 1 and Table 4)The overall level of IPC practice among respondents showed that the proportions having good, fair and poor practices were 41.2%, 8.2% and 50.7% respectively (Figure 1). Almost 70% of both doctors and nurses that participated in the study had a poor level of IPC practices. Over 80% of the CHEWs showed a good level of IPC practice while about half (50.2%) of participants in the privately-owned facility had good levels of IPC practice. Greater proportion of participants with had worked for less than five years had good IPC practices (60.6%). Table 4. Infection prevention and control practice among respondents regarding Lassa fever
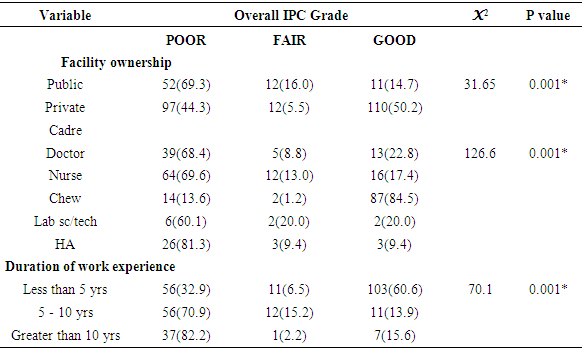 |
| |
|
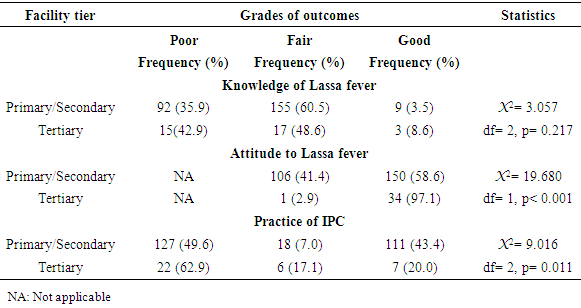
Association between facility tier and knowledge and perception of Lassa and practice of IPC (Table 5)Table 5 shows that a higher proportion of respondents from tertiary facilities (compared to other tiers) had good perception of Lassa fever (97.1% versus 58.6%). Conversely, a smaller proportion of HCWs in tertiary facilities had good practice of IPC in regards to Lassa fever (20.0% versus 43.4%). In both associations, the differences were statistically significant (X2= 19.680, p< 0.001; and X2= 9.016, p= 0.011 respectively).Table 5. Association between facility tier and knowledge, attitude and practice of IPC
 |
| |
|
4. Discussion
Majority of the health workers that participated in this study were working in privately-owned facilities, majority of the participants are nurses/midwives and CHEWs just as most of them are females. This demographic pattern is similar to findings in other related studies. [14, 15]Over three-fifth of participants had at least fair knowledge of Lassa fever. This is similar to findings from an earlier study in one of the participating LGAs (Esan West) where about the same proportion had at least fair knowledge of Lassa fever among all cadres of HCWs including medical doctors. [15] However this finding is different from findings in another related study done in Esan Central and Esan West LGAs of Edo state where almost four-fifth of the study participants were reported to have a good knowledge of Lassa fever. [4] The reference study was carried out among primary HCWs in government-owned PHCs and did not involve HCWs in privately owned facilities and study did not explore in-depth technical preventive measures as was done in this index study. The finding of this study is also different from the findings of another study among HCWs at a tertiary facility in Enugu in South-eastern Nigeria which showed that majority of the HCWs assessed had at least good knowledge of Lassa fever. [16] It must, however, be noted that the reference finding is not unexpected in a tertiary healthcare facility where training and retraining of HCWs is expected to be a continuous exercise. Furthermore, the above observation is buttressed by the finding of higher level of good knowledge of Lassa fever among HCWs in tertiary compared to those in primary or secondary healthcare facilities in this study. In a related study at Owo and Ose LGAs of Ondo State, in south-western, Nigeria less than half of participants had good knowledge of Lassa fever. [2] The low proportion of HCWs with good knowledge may be due in part to inadequate reinforcement in the knowledge of Lassa fever among HCWs and absence of training/retraining of HCWs on Lassa fever control. This is very important given the fact that Edo state is endemic for Lassa fever with a recent history of recurrent outbreaks. The attitude and perception regarding Lassa fever among the participants was generally good in this study as none of the participants was found to have poor attitude. The level of attitude was found to be good in majority of HCWs in privately-own health facilities as against about half of HCWs in government-owned health care facilities. This agrees with findings from a related study where a higher proportion of HCWs in privately-owned health facilities had good attitude towards Lassa fever compared to those in public facilities. [14] This may be due to the fact that there is a higher degree of HCWs supervision in the privately-owned healthcare facilities occasioned by smaller-sized structures as well as commercial factors. In addition, though tertiary HCWs who were mostly in public health care facilities had better attitude to Lassa fever, the number was too small to significantly influence the overall attitude of HCWs in public facilities. Well over four-fifth of the doctors and nurses that participated in the study also showed good attitude regarding the prevention and spread of Lassa fever and about the same proportion showed fair attitude among the CHEWs that participated in the study. This also is not far-fetched as the doctors and nurses are expected to demonstrate higher levels knowledge and corresponding attitudinal dispositions in the management of Lassa fever, although this is not so in all cases.The practice of IPC was found to be generally poor among the participants in this study across government and privately-owned health care facility and among the different cadres of HCWs irrespective of the number of years of work experience. This finding is consistent with the findings of a study done previously in one of the LGAs where this study was carried out. [4] It also noteworthy mention that this finding regarding poor IPC practices has been recurrent in several studies done in different parts of the country in the last few years: in a federal medical centre in South-south, Nigeria [17]; in a tertiary referral center in North-west, Nigeria [18]; in several selected hospitals in South-east, Nigeria [19] and in South-west, Nigeria. [2] In addition, in this study, good practice of IPC was lower in tertiary facilities than in primary or secondary healthcare facilities and this may be adduced to high work load and inadequate staffing in tertiary facilities in Nigeria. [20-22] The low level of good practice among tertiary HCWs observed in this study is consistent with that reported in a tertiary health care facility in Edo State where less than half of respondents had good ratings in the practice of IPC. [1] The consistently poor findings across the country with regard to IPC practice is indicative of the low level of priority accorded IPC measures in healthcare management in both government-owned and privately-owned health care facilities in country. This situation undoubtedly predisposes many HCWs to healthcare associated infections, including Lassa fever.
5. Conclusions
In conclusion, this study showed that the knowledge of Lassa fever, attitude of HCW towards preventive measures and IPC practices in both government-owned and privately-owned health facilities in the study area were less than desirable and put the HCWs at risk of healthcare associated infections including Lassa fever. As a matter of urgency, Edo State Government should ensure that education and training regarding Lassa fever with special emphasis on IPC is enhanced and sustained for HCWs in all public and private health facilities across the state. In addition, priority should be given the setting up of functional IPC committees at the State level and in all LGAs to ensure all health facilities in the LGAs meet the minimum IPC requirements necessary to guarantee effective control of nosocomial Lassa fever.
ACKNOWLEDGEMENTS
The authors acknowledge the support of all staff of Edo State Office of WHO.
References
| [1] | Tobin EA, Asogun AD, Odia I, Ehidiamhen G. 2013, Knowledge and practice of infection control among health workers in a tertiary hospital in Edo state, Nigeria. Direct Res. J. Health Pharm. Vol.1 (2), pp.20-27. |
| [2] | Ijarotimi IT, Ilesanmi OS, Aderinwale A, Abiodun-Adewusi O, OkonI. 2018, Knowledge of Lassa fever and use of infection prevention and control facilities among health care workers during Lassa fever outbreak in Ondo State, Nigeria. Pan African Medical Journal. 30:56. doi:10.11604/pamj.2018.30.56.13125. |
| [3] | Fisher-Hoch SP, Tomori O, Nasidi A, Perez-Oronz GI, Fakile Y, Hutwagner L. 1995, Review of cases of nosocomial Lassa fever in Nigeria: the high price of poor medical practice. BMJ. Sep 30; 311(7009): 857-9. |
| [4] | Aigbiremolen AO, Duru C, Awunor NS, Abejegah C, Abah S., Asogun D. 2012, Knowledge and Application of Infectious Disease Control Measures among Primary Care Workers in Nigeria: the Lassa Fever Example. International Journal of Basic, Applied and Innovative Research, 1(4), 122–129. |
| [5] | Ajayi NA, Nwigwe CG, Azuogu BN, Onyire BN, Nwonwu EU, Ogbonnaya LU et al. 2013, Containing a Lassa fever epidemic in a resource-limited setting: outbreak description and lessons learned from Abakaliki, Nigeria (January-March 2012). Int J Infect Dis. Nov; 17(11): e1011-6. PubMed | Google Scholar. |
| [6] | Ijarotimi IT, Oladejo JA, Jegede O, Nasidi A. 2015, Lassa fever in the State Specialist Hospital Akure, Nigeria: Case report, Contact tracing and outcome of hospital contacts. International Journal of Infectious and Tropical Diseases. 3(1): 20-28. |
| [7] | World Health Organization. 2016, Lassa fever in Nigeria. Accessed on 25th November 2016 from www.who.int/mediacentre. |
| [8] | Nigerian Centre for Disease Control. 2018, An update of Lassa fever outbreak in Nigeria, 2018 Week 22. Abuja. |
| [9] | Mayank D, Anshuman M, Singh RK, Afzal A, Baronia AK, Prasad KN. 2009, Nosocomial cross-transmission of pseudomonas aeruginosa between patients in a tertiary intensive care unit. Indian Pathol Microbiol. 52:509-513. |
| [10] | Joseph NM, Sistla S., Dutta, T.K., Badhe, A.S., Rasitha, D, Parija, SC. 2010. Role of intensive care unit environment and health-care workers in transmission of ventilator associated pneumonia. J. Infect Dev., 4: 282-291. |
| [11] | Viral Hemorrhagic Fever Consortium.2016, About Viral Hemorrhagic Fever Consortium. Accessed on 24th November 2016. |
| [12] | Cochran, G. W. 1963, Sampling techniques (2nd ed.). New York: John Wiley and Sons. |
| [13] | Araoye, M.O. 2003, Research Methodology with statistics for Health and Social Sciences. Nathadex Publishers. |
| [14] | Bilqisu JibrilIdris, Victor Inem, Mobolanle Balogun. 2015, Comparing the knowledge, attitude and practices of health care workers in public and private primary care facilities in Lagos State on Ebola virus disease. Pan Afr Med J. 22(Supp 1):19. |
| [15] | Tobin EA, Asogun DA, Isah EC, Ugege OG, Ebhodaghe P. 2013, Assessment of knowledge and attitude towards Lassa fever among Primary care providers in an endemic suburban community of Edo state: implications for control J. Med. Med. Sci. 4(8): 311-318. |
| [16] | Omotowo Babatunde I, Eyisi IG, Obi IE, Agwu-Umahi RO. 2016, Assessment of knowledge, attitudes and practices regardingLassa fever among healthcare workers in a tertiary hospital, Enugu, South-East, Nigeria: Implications for control. J Infect DisTher. |
| [17] | Isara AR, Ofili AN. 2010, Knowledge and practice of standard precautions among health care workers in the Federal Medical Centre, Asaba, Delta State, Nigeria. Niger Postgrad Med J.Sep; 17(3): 204-9. |
| [18] | Iliyasu G, Dayyab FM, Habib ZG et al. 2016, Knowledge and practicesof infection control among healthcare workers in a TertiaryReferral Center in North-Western Nigeria. Ann Afr Med. Jan-Mar; 15(1): 34-40. |
| [19] | Osuala Eunice Ogonna, Oluwatosin Abimbola O. 2017, Infectioncontrol by nurses in selected hospitals in Anambra State, Nigeria. Tropical Journal of Medical Research. 20(1): 53-60. |
| [20] | Eriki P, Oyo-Ita A, Odedo R, et al. 2015, Surgical workforce in Nigeria. Kampala, Uganda. |
| [21] | Adeloye D, David RA, Olaogun AA, et al. 2017, Health workforce and governance: the crisis in Nigeria. Hum Resour Health 15: 1–8. |
| [22] | Bello S, Ajayi D, Asuzu M. 2018 Determinants of Job Satisfaction among Physicians in Public Hospitals in Calabar, Nigeria Keywords: J Community Med Prim Heal Care 30: 19–33. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML