-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Prevention and Treatment
p-ISSN: 2167-728X e-ISSN: 2167-7298
2017; 6(2): 28-33
doi:10.5923/j.ijpt.20170602.02

The Effect of Taping on Isometric Shoulder Strength and EMG Activity of the Shoulder during Functional Movements
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKenneth Groop1, Paolo Sanzo1, 2, Carlos Zerpa1
1School of Kinesiology, Lakehead University, Thunder Bay, Canada
2Northern Ontario School of Medicine, Lakehead University, Thunder Bay, Canada
Correspondence to: Paolo Sanzo, School of Kinesiology, Lakehead University, Thunder Bay, Canada.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Objective: The purpose of this study was to compare the effects of Kinesio Tape (KT) to no tape on shoulder strength and electromyographic (EMG) activity of the teres minor (TM), infraspinatus (IS), and supraspinatus (SS) muscles when completing functional shoulder movements and resisted isometric testing for shoulder flexion, abduction, and external rotation. Methods: Thirty healthy individuals performed three repetitions of reaching into flexion, abduction, and external rotation as well as static resisted isometric contractions with and without KT. The EMG activity was recorded using a Delsys Trigno™ Wireless EMG System. The mean maximal strength force (kg) and EMG activity (mV) was recorded for each of the trials. Results: There was no significant interaction effect for muscle type and taping condition or main effects of taping condition on EMG activity during active shoulder flexion, abduction, and external rotation. There were significant main effects on measures of EMG activity for muscle type during active shoulder flexion (F(2, 171)=29.549, p=.0001, η2=.256), abduction (F(2, 171)=82.766, p=.0001 η2=.492), and external rotation (F(2, 171)=24.971, p=.0001, η2=.262). Post-hoc pairwise comparisons using a Bonferroni correction revealed significant differences between the SS and IS (p=.0001) and SS and TM (p=.0001) for shoulder flexion, abduction, and external rotation. There was no significant interaction effect for muscle type and taping condition on EMG activity or main effects for taping condition during resisted shoulder flexion, abduction, or external rotation. There were, however, main effects for muscle type on EMG measures for resisted shoulder flexion (F(2, 171)=21.379, p=.0001, η2=.20), abduction (F(2, 171)=48.361, p=.0001, η2=.361), and external rotation (F(2, 171)=5.884, p=.003, η2=.06). Post-hoc pairwise comparisons using a Bonferroni correction revealed significant differences for resisted shoulder flexion between the TM and IS (p=.0001) and SS (p=.0001); for resisted abduction between the TM and SS (p=.0001); and for resisted external rotation between the TM and SS (p=.0001). Paired samples t-tests revealed no significant difference in resisted isometric shoulder strength with and without tape for flexion, abduction, and external rotation. Conclusion: The application of KT may assist clinicians in altering (facilitating or decreasing) specific rotator cuff muscle activity levels during functional movements and activities that require static isometric contractions but appears to be context specific to the muscle. Further research is warranted on the use of different types of tape during other shoulder movements or sport specific actions.
Keywords: Kinesio Tape, Electromyography, Shoulder, Strength, Function
Cite this paper: Kenneth Groop, Paolo Sanzo, Carlos Zerpa, The Effect of Taping on Isometric Shoulder Strength and EMG Activity of the Shoulder during Functional Movements, International Journal of Prevention and Treatment, Vol. 6 No. 2, 2017, pp. 28-33. doi: 10.5923/j.ijpt.20170602.02.
Article Outline
1. Introduction
- Shoulder pain is common in healthcare practices and sport [2, 23] and workplace environments [2, 6]. Following the onset of shoulder pain, 50% of all individuals normally recover within six months and 60% within one year [30]. The reported range of prevalence rates of shoulder pain varies considerably due to the different definitions used in defining shoulder pain. The prevalence has been reported to range from 21-55% with the greatest peak occurring in middle aged individuals (45-64 years) [9, 17] but also in 12-57% of individuals during adolescence (12-18 years) [21, 26]. Shoulder pain is also more common in females [22, 29, 31] and in workers exposed to physical loads and vibration, who are required to complete repetitive movements, work in sustained postures, and use computers [6, 11].Conservative treatments range from pharmacological interventions, corticosteroid injection, exercise based treatments, and physical therapies including therapeutic modalities and manual therapies. When conservative treatments have plateaued or failed, often surgery is indicated [28]. It is at this stage that this common musculoskeletal complaint progresses from a stressor in which the patient reports discomfort and symptoms, to a period of increased functional restrictions, eventual lost work time, and finally disability [6]. More recently, another commonly used conservative physical therapy intervention includes therapeutic taping.Kinesio Tape (KT) is a type of therapeutic tape that was developed by Kenso Kase in the 1970s [7]. It has since become an increasingly popular taping technique used by a variety of patient and athletic populations with many unique features reported that separate it from other types of tape. Kase [12] proposed a wide variety of benefits with the application of KT including facilitating or inhibiting muscle activity, decreasing inflammation, and decreasing pain. Kinesio Tape is also believed to have mechanical benefits including altering posture, improving joint function, and improving muscle mechanics possibly aiding in injury prevention [7, 8, 10]. It is also reported that these benefits may result in increased motor unit recruitment and blood flow to the region, and improved lymphatic fluid circulation [7, 8]. More specifically, there is some anecdotal support but limited high quality research examining the effect of KT on the shoulder and the EMG activity of the rotator cuff muscles. The small numbers of studies that are available have used a variety of patient populations with various shoulder disorders along with different types of tape, methods of application, and research designs. Several systematic reviews and meta-analyses have reported mixed results with the majority suggesting a lack of support for the use of therapeutic taping [18, 19, 27]. In a meta-analysis by Csapo and Alegre [5], the application of KT did not result in increased shoulder strength. Similarly, in their studies, Keenan et al. [13] reported no significant effect of tape on shoulder strength, proprioception, or scapular kinematics and Alam et al. [1] also reported no effect on shoulder strength or range of motion.Conversely, Kim and Oh [15] reported that the application of rigid Endura Sports Tape effectively repositioned the humeral head resulting in increased external rotator muscle strength of the shoulder. Similarly, Kim, Kang, Kim, and Oh [14] reported an improvement in shoulder internal rotation strength and a decreased external/internal rotator strength ratio in patients with rotator cuff tendinitis [14]. This ratio has been reported to be a good predictor of shoulder injury [24].As can be seen, the literature is still quite contradictory and unclear on the clinical utility of therapeutic taping in the shoulder. Therefore, the purpose of this study was to examine the effects of KT compared to no tape on shoulder strength and the EMG activity of the teres minor (TM), infraspinatus (IS), and supraspinatus (SS) muscles during the completion of three commonly used functional movement patterns including shoulder flexion, abduction, and external rotation.
2. Methods
2.1. Participants
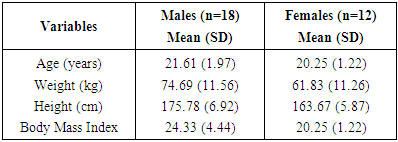
- Thirty healthy individuals (18 male, 12 female) participated in the study. Participants were excluded from the study if he/she: 1) suffered from a diagnosed upper extremity injury in the past six months (e.g., tendinitis, muscle strain, ligament sprain, or dislocation); 2) suffered from an upper extremity fracture or had shoulder surgery in the past five years; and 3) were allergic to any type of tape or adhesive. Demographic information and descriptive characteristics for all participants are highlighted in Table 1.
|
2.2. Instrumentation and Equipment
- A Delsys Trigno™ Wireless EMG System was used to collect and process the data. Three hybrid EMG Trigno sensors were used to acquire EMG activity for the TM, IS, and SS muscles. Resisted isometric shoulder strength was measured using a Lafayette Manual Muscle Test System©.
2.3. Procedures
- Before data collection commenced, ethical approval was obtained from the academic institution. All participants provided written consent and completed a Physical Activity Readiness Questionnaire. Upon completion of the required documents, the participant was guided through a brief warm up activity. The participant was then asked to indicate which side was his/her dominant shoulder and this was then used for data collection. Prior to the placement of the EMG electrodes, the participant’s skin was prepped, scrubbed, and cleaned with an alcohol swab to remove excess skin oils or dry skin. The Delsys Wireless EMG sensors were then placed on the TM, IS, and SS muscles according to the guidelines described by the Surface Electromyography for the Non-invasive Assessment of Muscle [24] and Perotto [20]. The participant was then positioned in sitting with his/her back resting against a chair with a back support and feet resting on the ground. The shoulder was positioned in the scapular plane and the participant was asked to maximally abduct the shoulder against resistance applied by the researcher. The maximal voluntary contraction (MVC) EMG activity (mV) for the SS was recorded. Similarly, maximal resisted external rotation was used to determine the MVC for both the IS and TM muscles. Once the MVC was obtained for each of the muscles of interest, the participant was asked to complete three trials of reaching into maximal forward flexion, out to the side into abduction, and finally external rotation. The mean EMG activity was recorded for each trial completed without tape. A 20 second rest period was allotted between each trial. Resisted isometric shoulder strength and the EMG activity while performing the static isometric contraction for shoulder flexion, abduction, and external rotation was measured next. Resisted isometric shoulder strength was measured using a Lafayette Manual Muscle Test System©. The participant was asked to maximally resist three trials of isometric flexion, abduction, and external rotation for a static three second hold generating as much force as they were capable of. The maximal strength (kg) and mean EMG activity (mV) was recorded for each trial without tape with 30 seconds of rest in between each trial. These specific shoulder movements were assessed as research highlighted their reported relationship and importance with regards to shoulder injuries. Repetitive overhead movements involving repetitive flexion and/or abduction and weakness in the shoulder external rotators have been described to be associated with an increased risk of shoulder injury and surgery [4, 32]. After completing the functional movements without tape, KT was applied using a facilitatory mechanical correction technique as described by Kinesio Taping Association International [16]. The taping technique was applied using a single I-strip; the length of the piece of tape was determined by measuring the distance from the medial end of the spine of the scapula to the lateral side of the humeral head. The KT was cut to that length and corners of the tape were rounded. The I-strip was then anchored with no tension starting at the medial end of the spine of the scapula. While holding the anchored position in place, the tape was laid down with 50-75% paper off tension and applied against the skin. The tape extended across the lateral aspect of the head of the humerus, ending on the anterior side of the humeral head where it was anchored with no tension (see figure 1). The tape was then rubbed against the participant’s skin to ensure that it was firmly adhered to the skin, activating the adhesive in the KT. The participant was then asked to perform the same procedures as previously described for the no tape condition and the EMG activity and resisted isometric shoulder strength measured as described previously.
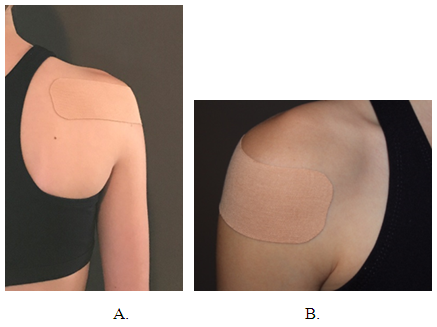 | Figure 1. Glenohumeral glide mechanical correction KT technique |
2.4. Signal Processing
- The raw EMG data was rectified using a mathematics absolute value function. A 10 Hz low pass filter was applied to the rectified signal to eliminate any high frequency noise that could potentially interfere with the EMG readings. The mean EMG from each rectified signal was computed and normalized and compared to the MVC for each muscle.
2.5. Data Analysis
- Descriptive statistics were used to compare means and standard deviations of the filtered and rectified mean absolute value EMG activity and mean shoulder strength values. Two independent variables (type of intervention – no tape and KT; and type of muscle – TM, IF, and SS) and two dependent variables (mean EMG activity and isometric strength) of the shoulder were examined. Statistical analysis was completed using IBM SPSS statistics version 24 with a significance level set at p<.05. The data was then analysed using two-way factorial ANOVAs to determine the interaction effect for each muscle in relation to the taping conditions with respect to EMG activity and shoulder strength; paired samples t-tests were used to assess differences in shoulder strength in relation to the tape and no tape conditions.
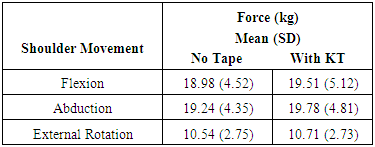
3. Results
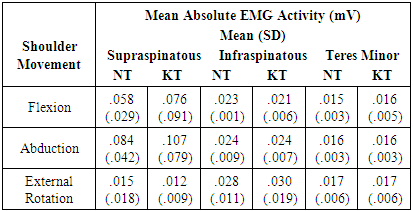
- Descriptive statistics for the EMG activity of the TM, IS, and SS muscles during functional movement testing is summarized in Table 2.
|
|
|
4. Discussion
- Based on the results of this study, there were significant main effects noted in the EMG activity with the application of KT to the shoulder compared to no tape when participants completed functional movements and resisted isometric contractions for shoulder flexion, abduction, and external rotation. There was increased EMG activity for the SS compared to the IS and TM muscles during shoulder flexion and abduction (EMG activity was greatest with the application of KT for both movements). There was reduced EMG activity for the SS compared to the IS and TM muscles during external rotation (EMG activity was least in SS with the application of KT). During resisted isometric strength testing for shoulder flexion, there was decreased EMG activity for the TM compared to the IS and SS muscles (EMG activity was greatest with the application of KT). During resisted shoulder abduction, there was decreased EMG activity for the TM compared to the SS muscle (EMG activity increased with the application of KT) and decreased EMG activity for the TM compared to the IS muscle for resisted shoulder external rotation. The higher EMG activity observed may be the result of an increased firing rate of the motor units or the recruitment of larger motor units involved in the activity. With the application of KT, this may have contributed to the greater force production. The increased external rotation force may impact the performance of overhead functional movements or activities that require increased amounts of shoulder external rotation. This may be beneficial during throwing or serving and in overhead racquet sports. External rotator strength has also been reported as one of the key contributors in the prevention of shoulder injuries and surgery [4, 32]. In fact, the force produced for all shoulder movements were generally higher with the application of KT compared to no tape. The functional or sport specific importance and application of this may be related to activities that require explosive movements or require high force outputs but more research is required to examine this relationship.These findings are in line with other researchers [14, 15] who reported increased strength in the external rotators with the application of tape. The mechanism and explanation for this phenomenon, however, is not clear. It is hypothesized that this may be related to mechanical repositioning of the humeral head, alteration of the length tension relationship of the muscles, or simply the proprioceptive input into the mechanoreceptors in the underlying tissue, but the exact mechanism is not understood. Conversely, these findings are not in line with those reported by Csapo et al. [5], Keenan et al. [13], and Alam et al. [1]. The differences in the types of tape and methods used, including the amount of stretch and direction of application, and methodological variations in study designs can explain the differences reported. In the present study, a facilitatory taping technique was used for the KT application. A facilitatory technique involves the application of KT from the origin of a muscle to the insertion of the muscle [13]. Questions have been proposed as to whether a facilitatory versus inhibitory effect can actually occur. Cai et al. [3] examined the effect of applying KT from the origin to the insertion (facilitatory technique) compared to the application from the insertion to the origin (inhibitory technique) in the forearm when completing a grip strength test. They did not find any significant changes in maximal grip strength, self-perceived effects, or EMG activity. It may be hypothesized that the application of the direction of tape (inhibitory versus facilitatory) may be specific to the underlying joint and tissue and the task being completed. In the present study, the EMG activity and strength generally increased for most movements (flexion and abduction). Further research, however, is required to expand on this concept in its application to other movement patterns and regions of the body.Conversely, the reduction in muscle activity in select muscles may be beneficial clinically in reducing or preventing over activity and possibly the development of overuse injuries and tendinopathy. This reduction in activity was evident with the application of tape in the SS muscle during active external rotation or the IS during active abduction. This finding may support the use of taping in individuals that must perform repetitive abduction or external rotation as part of their functional movement patterning, sport, or occupational task to prevent overuse in these muscles. This intervention may also help as a preventative strategy or, alternatively, may help to prevent further injury in individuals who may already have damage to that tissue (e.g., individual with a partial tear in the rotator cuff such as the SS or IS muscles).Some limitations of the current study include the fact that the effect of larger muscles (e.g., deltoid or upper trapezius) where not simultaneously monitored to assess how they impacted on the findings. Also, the effect of fatigue and the ordering of the tests were standardized for all participants but in the future altering the order may help get a better grasp of the effect of fatigue on performance.The results of the current study, however, add to the limited research about the proposed effects of KT on the shoulder. Further research is required examining the effect of taping in pathological populations with rotator cuff tendinopathy or tearing to see if similar results are found. Also, future research should examine how larger muscles and prime movers of the shoulder and cervical spine are affected with and without the application of tape (e.g., deltoid, pectorals, latissimus dorsi, upper trapezius muscles) compared to the smaller rotator cuff muscles. The combination of EMG with motion capture technologies may also aid in monitoring some of the possible changes that occur when completing functional or sport specific movements with and without tape. Comparing different types of tape and taping techniques would also aid in trying to better understand the clinical effects in the shoulder to determine which type of tape or technique should be used and when.
5. Conclusions
- In conclusion, there is very limited research into the effects of KT on the rotator cuff EMG muscle activity and strength. Our findings suggest that therapeutic taping applied to the shoulder may alter muscle activity when completing reaching or functional movement patterning into a flexed, abducted, or externally rotated position and when contracting the muscles isometrically in these positions. Further research into the effect of KT on the rotator cuff muscles is required so that a better understanding of the clinical utility of therapeutic taping in the shoulder during rehabilitation and how it relates to occupational or sport performance applications is understood.