-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Prevention and Treatment
p-ISSN: 2167-728X e-ISSN: 2167-7298
2017; 6(1): 4-11
doi:10.5923/j.ijpt.20170601.02

The Use of Therapeutic Taping in Individuals with Patellar Tendinopathy
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMichael Massei1, Paolo Sanzo1, 2, Eryk Przysucha1
1School of Kinesiology, Lakehead University, Thunder Bay, Canada
2Northern Ontario School of Medicine, Lakehead University, Thunder Bay, Canada
Correspondence to: Paolo Sanzo, School of Kinesiology, Lakehead University, Thunder Bay, Canada.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Objectives: Patellar tendinopathy is a common injury found among active populations. Typically, tendon pain is the most prevalent symptom associated with patellar tendinopathy and can range from mild to severe. This can be detrimental considering that the presence of these symptoms can also negatively affect range of motion (ROM), power, balance, and strength. Currently, there is much discrepancy regarding the effectiveness of conservative treatments like therapeutic taping using Kinesio tape (KT) or Leukotape (LT). Consequently, it is unknown which type of tape is beneficial for decreasing the common symptoms of this overuse injury when compared to no tape (NT) or placebo tape (PT). Therefore, the purpose of this pilot study was to examine the effects of therapeutic taping on pain, ROM, power, balance, and strength in physically active individuals with patellar tendinopathy and whether this testing protocol was feasible and able to detect changes in the variables described. Methods: Ten participants with patellar tendinopathy were recruited (M = 25 years; SD = 8.0) and attended four testing sessions. The baseline testing session involved NT and the subsequent taping sessions were randomized for the PT, LT, and KT conditions for each participant. The participant’s pain level was first measured and the testing sequence then examined ROM and strength of the knee, and power and balance measures. Pain levels were also measured again after the participant performed the balance task. To analyze the differences in perception of pain across the different tapes and times of administration, a 4 x 2 (Tape [KT, LT, NT, PT] x Time [Pre, Post]) repeated measures factorial ANOVA was conducted. To examine the potential effects of different taping conditions on ROM, power, balance, and strength, a one-way ANOVA, with taping condition as a repeated measures factor was used. Results: A significant effect was found between the taping conditions in the anteromedial (F(3,27)=2.96, p<.05, η2=.25), lateral (F(3,27)=7.2, p<.05, η2=.44), and posterolateral (F(3,27)=3.8, p<.05, η2=.30) directions for balance testing. In regards to knee flexor strength, a main effect for therapeutic tape was found (F(3, 27)=5.04, p<.05, η2=.32). There was a significant difference in knee flexor strength when comparing the KT and LT (t(9)=3.01, p<.05), KT and NT (t(9)=2.84, p<.05), and KT and PT conditions (t(9)=4.05, p<.05). There was no significant effect on pain, ROM, and power otherwise. Conclusions: Certain aspects of motor functioning, such as knee flexor strength and balance (anteromedial, lateral, and posterolateral directions), improved with the application of KT. This was not the case with other tape as the effect of the tape appeared to be limited to certain contexts.
Keywords: Patellar tendinopathy, Kinesio tape, Leukotape, Pain, Range of motion, Strength, Power, Balance
Cite this paper: Michael Massei, Paolo Sanzo, Eryk Przysucha, The Use of Therapeutic Taping in Individuals with Patellar Tendinopathy, International Journal of Prevention and Treatment, Vol. 6 No. 1, 2017, pp. 4-11. doi: 10.5923/j.ijpt.20170601.02.
Article Outline
1. Introduction
- Patellar tendinopathy is a common musculoskeletal injury found in individuals who have active lifestyles [25, 26, 37]. Nearly 10% of all hospital visits are related to tendinopathies and their growing prevalence among active individuals is concerning [16, 29]. It is believed that repetitive tasks like jumping, squatting, and running may lead to inflammation of the patellar tendon and possibly to degeneration and other adverse effects [32]. If untreated, these effects can negatively influence the quality of life, activities of daily living, and further participation in activity [10]. The use of therapeutic taping has been proposed as a treatment option in high-level athletes suffering from patellar tendinopathy [15], but little research exists involving the non-elite population. Therefore, it remains unclear if conservative treatments like therapeutic taping will be beneficial to these individuals. There are many intrinsic factors related to the onset of patellar tendinopathy. These factors are determined by an individual’s genetic expression and include age, gender, biomechanics, muscular imbalances, and leg length discrepancies [36, 42, 44]. Instances of patellar tendinopathy can be found in individuals upwards of 30 to 55 years of age [37]. With increasing age, the tendon structure may become rigid resulting in a failed healing response [10, 20, 36]. Extrinsic factors have also been associated with the development of patellar tendinopathy and include variations in activity frequency, intensity of the activity, the type of training surfaces, and the type of footwear [20, 25, 32]. In both acute and chronic cases, symptoms are commonly reported after activity or repetitive use of the knee joint [3, 23, 32]. Early intervention is needed in physically active individuals, as recovering from patellar tendinopathy can take upwards of eight months [37]. If left untreated, the tendon may potentially rupture or structural damage can occur in other areas of the knee joint [37, 40]. Therapeutic taping is commonly used in rehabilitation programs because of its reported beneficial properties. As the use of therapeutic taping becomes more common in sport and clinical settings, research must be continuously conducted to examine its utility and effectiveness regarding pain, range of motion (ROM), lower body power, balance, and leg strength. In clinical practice, there are several types of tape used to treat knee conditions; the two most common include Leukotape (LT) and the Kinesio taping (KT) methods [6]. Given the structural characteristics of both LT and KT, each tape and taping technique/method could serve as potential treatments for patellar tendinopathy. The exact relationship between pain and tendinopathy is not fully understood [9]. Some research has been conducted examining the effects of therapeutic tape as a potential treatment option for pain in other knee disorders other than patellar tendinopathy. Campolo et al. [6] investigated the effectiveness of therapeutic taping on anterior knee pain in patients with patellofemoral pain syndrome and reported statistically significant improvements with KT compared to no tape (NT) during stair climbing and squatting activities. Similarly, Osorio et al. [31] examined the effectiveness of two therapeutic patellofemoral taping techniques and reported significant improvements in pain, strength, and endurance tests with both LT and KT. Witvrouw et al. [44] has shown that decreased knee ROM is present and associated with the development of tendon pain. Maintaining adequate flexibility may, therefore, be imperative in the prevention of patellar tendinopathy [10]. Sanzo et al. [38] examined the effects of therapeutic tape on lower quadrant ROM and strength in healthy university students and found that LT significantly decreased knee flexion and extension when compared across taping conditions. Although LT decreased ROM in healthy individuals, the researchers reported that these results were valuable from a clinician’s perspective, as it may determine which type of therapeutic tape to apply in certain contexts or patient populations [38]. For example, the application of LT may not be beneficial for healthy individuals who require full ROM of the knee to carry out specific task demands or activities of daily living but may be useful if trying to decrease the knee range of motion or avoid certain positions in some pathological populations [38]. It is not clear whether this will also be the case for patients with patellar tendinopathy. Lower body power is imperative to jumping performance [7, 24]. Power has been defined as the ability of a muscle, or group of muscles, to produce force in order to overcome minimal resistance in a short period of time [12, 24]. Nakajima and Baldridge [30] examined the effectiveness of KT on power measured via vertical jump height and dynamic postural control measured using the Star Excursion Balance Test (SEBT). The results revealed no significant differences between taping conditions in vertical jump height and dynamic postural control for the SEBT. This was contrary to the results for female participants who demonstrated significant improvements in the posteromedial and medial directions, respectively. The researchers concluded that KT might have an effect on dynamic postural balance but this may be affected by sex [30]. Maintaining dynamic balance is imperative to sport performance and the completion of everyday functional and occupational tasks. During gross movements such as jumping, the knee joint is constantly adapting to varying force loads [14, 18]. Athletes suffering from patellar tendinopathy may have difficulty in maintaining adequate balance since the structure and function of the patella and overall quadriceps strength has been compromised. Currently, however, research examining the effectiveness of therapeutic taping on balance in athletes suffering from patellar tendinopathy remains limited.To date, few studies have been conducted examining the effectiveness of therapeutic taping on knee strength in pathological knee populations. Aktas and Baltaci [2] compared the effectiveness of KT and knee bracing on knee strength during jumping performance and using the Isomed 2000 isokinetic dynamometer. Significant increases were seen in isokinetic knee extension torque at 180°/sec with the application of KT and in the hop distance with both legs [2]. Conversely, Sanzo et al. [38] also found that therapeutic tape had no significant effects on knee flexion or extension strength when compared to the application of NT and placebo tape (PT). Despite the growing trend of using KT and LT in high-level sports and as part of rehabilitation programs, few comparative studies have examined the effectiveness of different types of tape to NT and/or the application of PT. Consequently, there is limited evidence supporting the beneficial claims associated with therapeutic taping, especially in pathological populations. Since patellar tendinopathy remains a common overuse injury in high-level sport and with individuals maintaining active lifestyles [16, 29, 37], it is unknown which type of therapeutic tape, if any, is most beneficial for decreasing the common symptoms associated with this injury. Therefore, the purpose of this pilot study was to examine the effects of therapeutic taping on knee pain, ROM, power, balance, and strength, in individuals with patellar tendinopathy and whether this testing protocol is feasible and able to detect changes in the variables described.
2. Methods
2.1. Participants
- After obtaining ethical approval from the academic institution, participants were recruited through purposive sampling. Participants included men and women between the ages of 18 and 45 years diagnosed with patellar tendinopathy by a healthcare provider. Moderately physically active individuals engaging in 150 minutes of moderate to vigorous exercise were included in the study. Participants were excluded from the study if he/she participated in excess of 300 minutes of moderate to vigorous exercise a week, had knee surgery within the past five years, or were currently experiencing any additional lower body injuries or conditions. Also, those who received corticosteroid injections in the knee within the past year or were allergic to adhesives or athletic tape, were excluded.
2.2. Procedure
- After informed consent was obtained, participants committed to four, 30-minute testing sessions with at least one day of rest between them. One session was allocated to each of the following conditions: NT, PT, KT, and LT. The baseline testing session involved NT and the subsequent taping sessions were randomized for each participant. During the initial NT session, participants were informally interviewed about his/her injury and height and body mass measured. Following the interview, the participant’s pain level was measured using the Numeric Pain Rating Scale (NPRS). The NPRS [19] consists of an 11-point scale with zero indicating no pain, one to three indicating low pain, four to six indicating moderate pain, and seven to ten indicating severe pain. After this was completed, the testing sequence was implemented as follows: ROM of the knee joint, strength, power, and balance measures. Knee ROM (°) was assessed with a standard goniometer following the procedures adapted from Reese and Bandy [35]. All measurements were taken in a supine position. The mean of three trials was used in the subsequent analysis for each taping condition. Power was measured using a counter movement vertical jump procedure [27]. Before performing the jump, the participant stood with his/her dominant arm facing the wall with both feet flat on the ground. A piece of tape was then wrapped around the participant’s third and fourth finger. He/she then extended the dominant hand as high as possible and touched the wall using these two fingers. The tape was adhered to the wall marking the highest point reached by the participant. Once the reach height was recorded, the participant was instructed in the proper jumping technique and was given one practice trial. The participant was cued to jump as high as possible and the highest point touched on the wall was recorded with another piece of tape, as previously described. The participant was asked to use countermovement of the arms to project the body upwards. The mean of three trials (cm) was used to determine peak leg power (Watts) as calculated by the equation used in previous research by Bicici et al. [4] and Sayers et al. [39]:
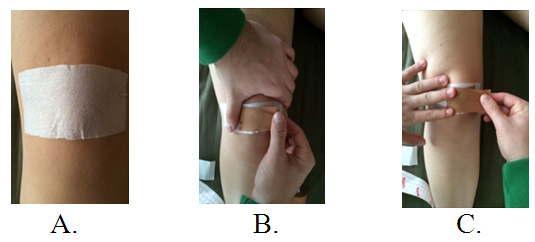
 The SEBT was used to measure dynamic balance [17]. Participants stood with his/her affected leg over the center of a grid. The grid had eight lines and each of these lines extended at 45° increments in the anterior, anterolateral, anteromedial, posteromedial, posterior, posterolateral, medial, and lateral directions. Before the formal testing was completed, the participant’s leg length was measured to account for inter-individual differences. Once the affected leg was placed over the center mark, the participant was asked to extend the opposite leg as far as possible on each line following a clockwise direction. In order to complete the trial, the participant had to touch the ground with the toe of the reaching leg. A total of 24 attempts were carried out, with three reaches in each of the eight directions. A coloured piece of tape was placed at the point of contact between the toe and the ground. After each reach, a 30-second break was allotted to measure the distance between the center mark and tape. This value was then divided by the participant’s leg length and the mean of the three trials (%) was used for the subsequent analysis. Lastly, knee strength was measured using a Baseline Electronic Hydraulic Push-Pull Dynamometer [1, 5]. Measurements were obtained while the participant was in a seated position with the knee flexed to 90°. Three trials (lbs) for each movement (flexion and extension) were carried out, with one minute of rest between them; the mean strength value was used in the subsequent statistical analysis. Pain levels were also measured once again after the participant performed the balance task. During the PT, KT, and LT sessions, the application of the tape commenced after the initial pain level was recorded. For all of the taping interventions, a topical adhesive spray was applied to the participant’s knee directly over the taping area. The PT application procedure consisted of a piece of Hypafix applied over the anterior aspect of the patella without any tension or compression [8]. See Figure 1.
The SEBT was used to measure dynamic balance [17]. Participants stood with his/her affected leg over the center of a grid. The grid had eight lines and each of these lines extended at 45° increments in the anterior, anterolateral, anteromedial, posteromedial, posterior, posterolateral, medial, and lateral directions. Before the formal testing was completed, the participant’s leg length was measured to account for inter-individual differences. Once the affected leg was placed over the center mark, the participant was asked to extend the opposite leg as far as possible on each line following a clockwise direction. In order to complete the trial, the participant had to touch the ground with the toe of the reaching leg. A total of 24 attempts were carried out, with three reaches in each of the eight directions. A coloured piece of tape was placed at the point of contact between the toe and the ground. After each reach, a 30-second break was allotted to measure the distance between the center mark and tape. This value was then divided by the participant’s leg length and the mean of the three trials (%) was used for the subsequent analysis. Lastly, knee strength was measured using a Baseline Electronic Hydraulic Push-Pull Dynamometer [1, 5]. Measurements were obtained while the participant was in a seated position with the knee flexed to 90°. Three trials (lbs) for each movement (flexion and extension) were carried out, with one minute of rest between them; the mean strength value was used in the subsequent statistical analysis. Pain levels were also measured once again after the participant performed the balance task. During the PT, KT, and LT sessions, the application of the tape commenced after the initial pain level was recorded. For all of the taping interventions, a topical adhesive spray was applied to the participant’s knee directly over the taping area. The PT application procedure consisted of a piece of Hypafix applied over the anterior aspect of the patella without any tension or compression [8]. See Figure 1. | Figure 1. Placebo taping technique |
 | Figure 2. McConnell taping technique with LT |
 | Figure 3. Pitchfork taping technique with KT |
2.3. Design and Analysis
- A repeated measures factorial design was implemented in this study. Descriptive statistics were used to compare the mean and standard deviations for individual ROM, power, balance, and strength data. To analyze the differences in the perception of pain across the different tapes and times of administration, a 4 x 2 (Tape [KT, LT, NT, PT] x Time [Pre, Post]) repeated measures factorial ANOVA was conducted. To examine the potential effects of different taping conditions on ROM, power, balance, and strength, a one-way ANOVA, with taping condition as a repeated measure factor was used. The alpha level was set at .05.
3. Results
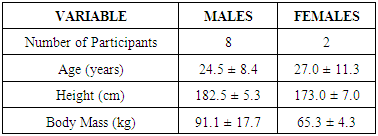
- A total of 10 participants with patellar tendinopathy were recruited into the pilot study. The descriptive characteristics of the sample are highlighted in Table 1. No adverse effects were reported with the application of tape or with the testing protocol administered.
|
3.1. Pain
- The results from the repeated measures factorial ANOVA revealed no significant interaction or main effects for time, as well as taping condition.
3.2. Range of Motion
- In terms of ROM, there were no significant differences in performance between the taping conditions for knee flexion and no significant differences between the taping conditions for knee extension.
3.3. Power
- There were no significant differences in power between the taping conditions. In regards to knee flexor strength, a main effect for therapeutic tape was found (F(3, 27)=5.04, p<.05, η2=.32). The results from the paired samples t-test revealed that there was a significant difference in knee flexor strength when comparing the KT and LT (t(9)=3.01, p<.05), KT and NT (t(9)=2.84, p<.05), and KT and PT conditions (t(9)=4.05, p<.05). Analysis of individual performances further confirmed this finding as nine participants produced greater strength with KT and LT when compared to NT and PT. When performances with therapeutic tape were compared, all but one participant generated greater strength with KT. The effects of KT and LT were consistent among participants. This trait was also apparent across the taping conditions, indicating that the differences in performance may be related to therapeutic effects. With respect to knee extensor strength, there were no significant differences between the taping conditions.
3.4. Balance
- There was no significant effect in SEBT with the application of therapeutic tape in the anterior, anterolateral, medial, posterior, and posteromedial directions. A significant effect was found between the taping conditions in the anteromedial (F(3,27)=2.96, p<.05, η2=.25), lateral (F(3,27)=7.2, p<.05, η2=.44), and posterolateral (F(3,27)=3.8, p<.05, η2=.30) directions. During the SEBT, greater performances are associated with greater reach distances. The results from the paired samples t-test revealed that reach distances were greater with the application of KT when compared to NT in the anteromedial (t(9)=3.39, p<.05) and posterolateral (t(9)=2.57, p<.05) directions. As for the lateral direction, significant differences in performance were found between KT and NT (t(9)=3.89, p<.05), LT and NT (t(9)=4.55, p<.05), and PT and NT (t(9)=-2.69, p<.05) conditions. The effects with the application of KT and LT were relatively consistent among the participants and the directional movements being performed. Similar consistencies were also revealed across the taping conditions, indicating that the differences in performance may be related to the effects of the condition applied.
4. Discussion
- The purpose of this pilot study was to examine the effects of therapeutic taping on pain, ROM, power, balance, and strength in physically active individuals with patellar tendinopathy and whether this testing protocol was feasible and able to detect changes in the variables described.
4.1. Pain
- Pain is a symptom of patellar tendinopathy and research regarding its etiology remains inconclusive [10, 34, 43]. The present results showed that the application of therapeutic taping (LT or KT) did not significantly decrease pain when applied to individuals with patellar tendinopathy. However, despite the lack of statistically significant changes in the pain levels across the different experimental conditions, clinically significant findings were found in the NPRS scores for the individual profiles. A clinically significant difference in pain is defined as a two-level fluctuation in the NPRS score [13]. When therapeutic tape (LT and KT) was compared, the participants pain levels remained unchanged post-treatment but during the NT condition, these participants experienced a clinically significant increase in pain. It is plausible that both KT and LT may be beneficial for preventing increased pain when applied to the knee if the participant performs similar tasks to those tested in the current study. The positive clinically significant findings partially support the use of tape as an effective method of reducing pain. The effects of tape on pain may be more pronounced if the initial pain levels were at a more moderate or higher level or during the acute phase of the onset of symptoms but further research is required to explore this.As previously mentioned, few studies have examined the effectiveness of therapeutic taping on pain in individuals with patellar tendinopathy. The results of the current study differ with those previously reported on other knee pathologies (e.g., patellofemoral pain syndrome) as different taping techniques and functional or sport specific tasks were used. The effects of therapeutic tape on pain may be context specific to certain tasks, injuries, and taping methods. Osorio et al. [31] examined the effects of KT and LT on pain in physically active individuals with PFPS. They found that both KT and LT significantly decreased pain when applied to the knee. Osorio et al. [31] reported that when therapeutic tape was applied, the mechanoreceptor stimulation underlying the taped skin might have contributed to the decreased transmission of pain [22, 31]. Additionally, Osorio et al. [31] speculated that the pain reduction associated with KT might also be attributed to the amount of tape applied to the knee, as more tape was required with KT than with the LT technique. The increase in tape used might have further influenced the underlying sensory receptors, ultimately decreasing pain symptoms [31]. Based on the previous research, it appears that the effects of KT and LT on pain are constrained by the type of technique, injury, population, and the tasks being performed.
4.2. Range of Motion
- Individuals suffering from patellar tendinopathy often experience pain, which restricts knee ROM [43, 44]. The application of KT and LT did not result in changes in knee flexion or extension in individuals with patellar tendinopathy. It is possible that the amount of pain the participants were experiencing was not high enough to limit knee flexion ROM. Perhaps individuals suffering from patellar tendinopathy only experience deficits in range when their subjective pain levels are at a more severe level. The effects of therapeutic tape may be more evident in this regard and could lead to improved ROM but further research is required. In this specific context, the application of KT may be more beneficial than LT, given the fact that KT is more elastic and has the potential to elicit other therapeutic effects (e.g., preventing further pain) [22]. In the acute stages, or if pain or discomfort is present at the end of range of knee flexion, the goal of the health care provider may be to reduce knee mobility. This will prevent the individual from moving into this painful range that further tensions the patellar tendon. Therefore, in this clinical example, a more rigid tape like LT may be suitable. Overall, it appears that neither KT nor LT significantly affect knee ROM; however, the elasticity present within the tapes may be appropriate in certain contexts (e.g., decreasing knee flexor ROM). The effects of therapeutic tape on ROM are unclear but may be specific to certain populations, body segments, and goals of the health care provider. Given the limited results, it is difficult to infer the appropriateness of therapeutic tape on knee ROM. In essence, the application of therapeutic tape does not appear to alter ROM in individuals with patellar tendinopathy.
4.3. Power and Strength
- Activation of the quadriceps muscles is a fundamental component to the vertical jump task, where greater contraction contributes to increased power production and a higher vertical jump height [12, 39]. The application of therapeutic tape is believed to generate greater muscular contraction when applied to the knee [22, 28]. The results of the current pilot study failed to support these reported hypotheses, as no substantial changes in power were revealed across the taping conditions. Although the amount of power produced remained unchanged across the different experimental conditions, a trend revealed greater power with LT when compared to KT. Therefore, it is possible that the taping methods involved may have contributed to these results. The LT technique incorporated a mechanical correction that realigns the patella into the trochlear groove [28]. It is believed that this realignment increases the activation of the quadriceps muscles, relieving any potential joint compression [11, 28]. Unlike the LT technique, the KT method incorporated a tendon correction technique [22]. This method is believed to reduce pressure surrounding the patellar tendon and increase mechanoreceptor (sensory) activity underlying the taped area [22]. The results of the current study are in line with the findings reported by Nakajima and Baldridge [30] who reported that KT did not affect vertical jump height and dynamic postural control (SEBT) in healthy individuals. The researchers believed that the lack of changes was due to the fact that the application of KT failed to stimulate the mechanoreceptors underlying the taped skin [30]. Generally, greater power production contributes to a greater jump height [27]. In the current study, the application of KT or the mechanical correction with LT did not affect the power generated at the knee.
4.4. Balance
- During sport or recreational activity, the knee joint is continuously adapting to various dynamic constraints [14, 18]. These constraints may further stress the patellar tendon [10] and potentially compromise the individual’s ability to maintain balance during dynamic tasks. The results of the current study revealed that performances were substantially greater with KT in the anteromedial, lateral, and posterolateral directions. It is possible that performances during the SEBT may be enhanced when individuals are able to achieve full knee ROM [21]. The elastic and supportive characteristics of KT did not appear to restrict knee ROM, which could explain why participants were able to improve performances by reaching further in the anteromedial, lateral, and posterolateral directions. Since the primary objective of the SEBT is to maintain postural control while reaching with the non-supported leg as far as possible without losing balance, underlying somatosensory systems are believed to be active when performing the directional movements [21]. The Pitchfork technique applied with KT has been reported to heighten mechanoreceptor activity underlying the taped skin [22]. It is possible that the tape may have activated the somatosensory system when the participants were performing the directional movements in the anteromedial, lateral, and posterolateral directions. The elastic properties of KT may allow for greater ROM and stimulation of the mechanoreceptors underlying the taped area. To date, there have been few studies that have compared the effectiveness of both KT and LT on patellar tendinopathy, especially during the performance of the SEBT. Further research is required, however, to determine any definitive effects. It appears that the effectiveness of LT on balance performance may be injury specific and that the effectiveness of KT, as related to balance, can be joint specific. Hence, it may have a different therapeutic effect when applied to the ankle as opposed to the knee. In the context of the current study, health care providers should give special consideration to KT, as it may improve balance during specific directional movements. This may be beneficial for individuals that require adequate balance when performing certain dynamic movements.
4.5. Strength
- Individuals suffering with patellar tendinopathy often reduce activity levels in order to decrease or prevent further pain associated with this injury [9]. Consequently, decreased activity levels due to pain may lead to strength impairments in the lower quadrant. Additionally, the presence of swelling or edema within the knee joint has been reported to inhibit muscular strength [41]. The results of the current study revealed that the application of KT increased knee flexor strength, when compared to NT, PT, and LT. It is possible that the application of KT may have dissipated any swelling within the knee, ultimately heightening underlying motor neuron activity, and resulting in greater muscular contraction and strength [22, 41]. In terms of LT, the McConnell taping technique incorporated a mechanical correction that realigned the patella into the trochlear groove [28]. The realignment of the patella along with the direction of the LT’s application may not have affected the swelling within the knee or muscular strength. Ultimately, it appears that KT may be more beneficial to the improvement of knee flexor strength in individuals with patellar tendinopathy. Further research, however, is required exploring the effects of therapeutic tape as this may be more effective in some pathological populations that are experiencing greater strength impairments than others. Limitations to the current pilot study included a small sample size, an uneven ratio of participants with acute versus chronic patellar tendinopathy, and a male dominated sample. These limitations make generalizability of the findings limited and conservative. Participants were also asked to attend a total of four testing sessions in order to complete the study. Four testing sessions was challenging for participants from a time commitment perspective and may have contributed to the small sample size. Future research should also consider combining the use of more sophisticated laboratory equipment (e.g., electromyography, force platform, video motion capture) in order to help determine the underling effects of therapeutic tape and changes in biomechanics. Additional research should also compare the effectiveness of therapeutic tape in participants with acute versus chronic symptoms of patellar tendinopathy.
5. Conclusions
- The present pilot study examined the effects of therapeutic taping on knee pain, ROM, power, balance, and strength in individuals with patellar tendinopathy. The results showed that certain aspects of motor functioning, such as knee flexor strength and balance (anteromedial, lateral, and posterolateral directions), improved with the application of KT. This was not the case with LT, as the effect of the tape appeared to be limited to certain contexts. To date, there is an increasing trend incorporating therapeutic tape into the clinical setting. Surprisingly, few studies have been conducted examining the effectiveness of the tapes using pathological populations and even fewer have compared therapeutic tape to NT and PT conditions. As evident within the current pilot study, there is a potential that therapeutic tape may have a distinctive effect on pain when symptoms are in the acute stage of the injury. In order to make any definitive conclusions, a larger study with an equal ratio of males to females is needed. The current methodology appears feasible and is able to detect changes in ROM, strength, power, and balance with no adverse effects reported by the participants. The information obtained from this study may guide future research to examine standards of care practices for individuals suffering from patellar tendinopathy and potentially determine the appropriateness of therapeutic tape in acute versus chronic cases.