-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Prevention and Treatment
p-ISSN: 2167-728X e-ISSN: 2167-7298
2016; 5(3): 39-45
doi:10.5923/j.ijpt.20160503.02

Epidemiological Study: Research of Urolithiasis in Those with Metabolic Syndrome in Western of Algeria
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLDjahida Hadj Merabet1, Karima Bereksi Reguig2
1Department of Biology, Faculty of Natural and Life Sciences, Djillali Liabes University, Sidi Bel Abbes, Algeria
2Laboratory of Environment, Faculty of Natural and Life Sciences, Djillali Liabes University, Sidi Bel Abbes, Algeria
Correspondence to: Djahida Hadj Merabet, Department of Biology, Faculty of Natural and Life Sciences, Djillali Liabes University, Sidi Bel Abbes, Algeria.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Backgroundandobjective:Closer the links between these two pathologies that have alarmingly propagated into all the world without exception by assessing the epidemiological parameters.PatientsandMethods:An epidemiological investigation was conducted in the city of Sidi Bel Abbes (western Algeria). Our study was performed on patients files at the endocrinology service during three years [(12/2006-11/2009)] and the methodology of the epidemiological analysis was based in two axes: descriptive (Prevalence & Incidence) and analytic epidemiology (exposed /non exposed: Relative Risk (RR)).Results: The epidemiological study of 600 files shows that prevalence of Metabolic Syndrome (MetS) according the NCEP ATP III diagnostic criteria is 42.66% which is 1,7 times higher among women compared to men and that of Urinary Lithiasis (UrL) in the general population is 6.16% whereas in those with MetS is 11.32%. We also noted an increase in the incidence of MetS and its risk factors parallel to that of the UrL. The results show that the Relative Risk of urinary lithiasis is > 1 among patients who have the MetS than those unscathed and this proves that metabolic syndrome is a risk factor of urinary lithiasis; We also noted that the risk is 1,7 times higher among men compared to women. Conclusions:Our study shows the emergence in the incidence of MetS and its risk factors over time. This emergence has affected also UrLin those with MetS. It is therefore essential to identify this insidious couple.
Keywords: Metabolic syndrome, Urinary lithiasis, Risk Factors, Epidemiology
Cite this paper: Djahida Hadj Merabet, Karima Bereksi Reguig, Epidemiological Study: Research of Urolithiasis in Those with Metabolic Syndrome in Western of Algeria, International Journal of Prevention and Treatment, Vol. 5 No. 3, 2016, pp. 39-45. doi: 10.5923/j.ijpt.20160503.02.
Article Outline
1. Introduction
- Metabolic syndrome is a worrying entity which does not cease increasing not only in the developed countries but in the whole world. It is well established that the subjects reached of this syndrome are three times exposed at the risk to undergo a heart attack or a stroke compared to those which are unscathed [1]. Moreover, it seems that the frequency of all disturbances of the metabolic syndrome coincides with the urinary lithiasis.As urinary lithiasis, metabolic syndrome or syndrome X is multifactorial. Several epidemiological studies have focused on the search for a pathophysiological relationship between the different components of this syndrome (obesity, hypertension, diabetes, dyslipidemia) and urolithiasis.In metabolic syndrome, insulin resistance and renal ammoniagenesis defect are the main disorders causing lithogenesis. [2]. The main consequence of renal insulin resistance induced by metabolic syndrome is a deficit in production and excretion of ammonium ions, which leads to lower urinary pH and a decrease in the solubility of uric acid [3-5]. Thus, patients who are overweight or obese, the excessive animal protein intake tend both to lower the urinary pH by increasing the urinary excretion of phosphate and the uricosuria, promoting component of uric acid super-saturation [3, 6].The first study suggesting this relation was conducted out by Pak and al. the group of Dallas characterized the biochemical profile of patients presenting a idiopathic uric lithiasis, compared to a reference group paired for the age and the BMI, these patients presented a hyperuricemia, an acid urinary pH but curiously a defect of urinary urate excretion [7]. After that, many studies showed an increased incidence of stones with overeating and overweight among both men and women [8, 9].In Algeria, we are also concerned in the occurrence of metabolic syndrome and urinary lithiasis, but we lack the clinical and epidemiological data.The objective of this study is to make the links closer between these two pathologies that have alarmingly propagated into all the world without exception by assessing the epidemiological parameters.
2. Population and Methods
2.1. Participants
- An epidemiological investigation was conducted in Sidi Bel Abbes (city in northwestern Algeria). Our study was performed on patients’ files at the endocrinology service of the University Hospital Dr HASSANI Abdelkader during three years [(12/2006 - 11/2007) (12/2007 - 11/2008) (12/2008 - 11/2009)].600 files have been treated to seek subjects with the metabolic syndrome and within this population we searched patients who suffer or have suffered from the urinary lithiasis (Figure 1).
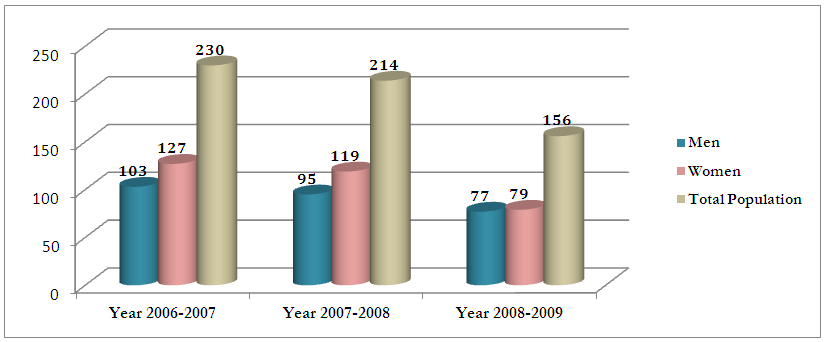 | Figure 1. Repartition of study population by Year |
2.2. Epidemiological Statistics
- “Epidemiology is the study of the distribution and determinants of health-related states in specified populations, and the application of this study to control of health problems.” [11]. Epidemiologic studies may be [12] descriptive, organizing data by time, place, and person; or [13] analytic, incorporating a case-control or cohort study.Our data were seized into Excel database. After coding, they were treated in: 2.2.1-Descriptive epidemiology (Prevalence & Incidence): It describes the distribution of health events and their determinants in the population. It is divided into:ü Prevalence survey: This is a survey to determine the total number of people presenting the phenomenon (metabolic syndrome, urinary lithiasis, type 2 diabetes, obesity ......) in a population. The prevalence rate is the ratio of the number of cases on the manpower of the population during the investigation period (12/2006 to 11/2009).ü Incidence survey: This is a survey that estimates the number of new cases of a phenomenon of health in a population during a given period [(12/2006 to 11/2007), (12/2007 to 11/2008) & (12/2008 to 11/2009)].2.2.2-Analytical epidemiology (exposed /non exposed: RR) They analyze the relationship between exposure to a risk factor and a phenomenon of health. Etiological investigations are always comparative (they compare two different groups).The investigation exposed / unexposed estimate the relative risk of the disease (RR). Relative risk is the ratio of risk among patients who have the metabolic syndrome on the risk of those unscathed. [14] The interpretation of the relative risk is as follows:• RR = 1: no relationship between the risk factor and disease• RR> 1: increased risk of disease (risk factor)• RR <1: reduced risk of disease (protective factor)
3. Results and Discussion
3.1. Descriptive Epidemiology
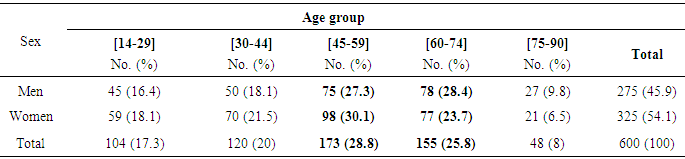
- 3.1.1. Prevalence study q The distribution of the population by age shows that 55.63% of men have an age range [45-74] years Vs 53.84% women (Table 1). q The epidemiological study of 600 files shows that the prevalence of metabolic syndrome according the diagnostic criteria of NCEP ATP III, 2002 is 42.66 % which is higher among women compared to men (15.66% Men Vs 27% Women).
|
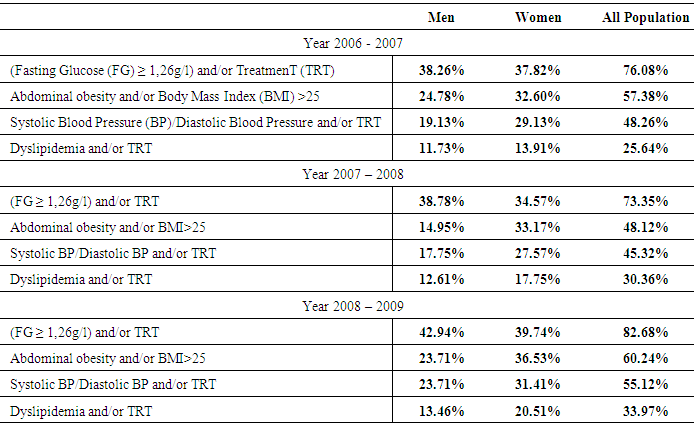
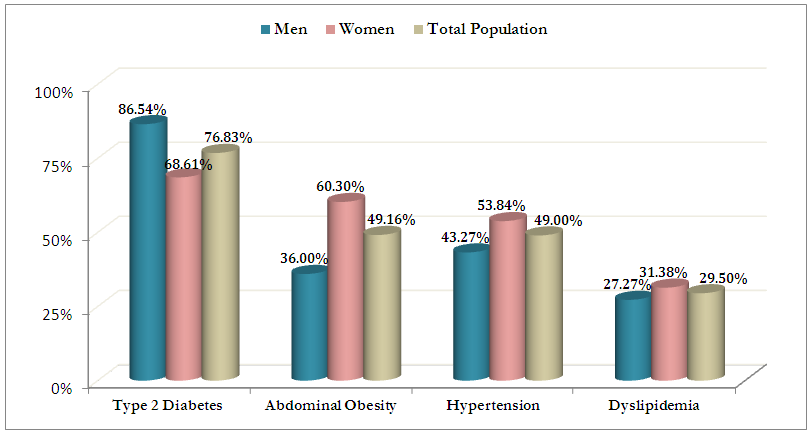 | Figure 2. Incidence of different component of Metabolic Syndrome |
|

|
|
3.2. Analytic Epidemiology
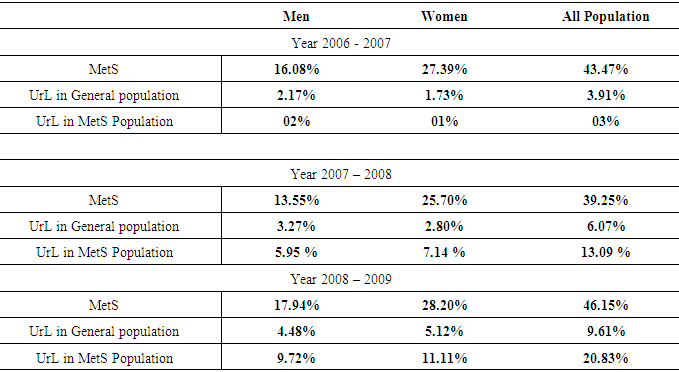
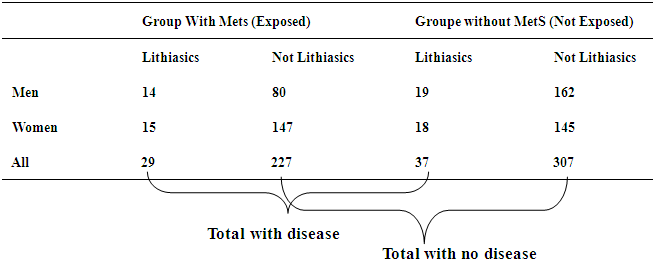
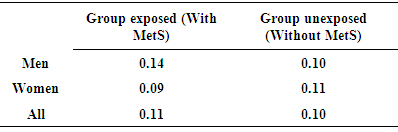
- q The results show so that the Relative Risk of urinary lithiasis is > 1 among patients who have the MetS than those unscathed and this proves that metabolic syndrome is a risk factor of urinary lithiasis. (table 5 & 6)
 Metabolic syndrome has become the subject of increased urologic research because of continued observations that it is associated with an increased risk of urinary stone disease. West and colleagues [34] examined the association between the number of metabolic syndrome traits and risk of urolithiasis using a national sample of patients in the United States. Prevalence of kidney stones increased with the number of traits, from 3% with 0 traits to 9.8% with 5 traits.
Metabolic syndrome has become the subject of increased urologic research because of continued observations that it is associated with an increased risk of urinary stone disease. West and colleagues [34] examined the association between the number of metabolic syndrome traits and risk of urolithiasis using a national sample of patients in the United States. Prevalence of kidney stones increased with the number of traits, from 3% with 0 traits to 9.8% with 5 traits.
|
|
4. Conclusions
- Our study shows the emergence in the incidence of MetS and its risk factors over time which there was an increase of 1.2 times.Moreover, the results show that women are more predisposed to Metabolic Syndrome than men (1.7 times ≈ (2) higher among women than men).This emergence has affected also Urinary Lithiasis and especially in those with metabolic syndrome which there was an increase of 1.5 times and till 6.9 times.We note that the incidence of urolithiasis in men is higher compared to women in the general population while in the population affected by the metabolic syndrome, in women is higher compared to men. This can be explained by the fact that women are more predisposed to Metabolic Syndrome.Our study show that metabolic syndrome is a risk factor for urinary lithiasis. The different components of syndrome X (type 2 diabetes, hypertension, visceral obesity and dyslipidemia) coincide with urolithiasis. It is therefore essential to identify this insidious couple and to recognize and seek the metabolic syndrome in the management of urolithiasis.Prevention of urinary lithiasis related to metabolic syndrome is based on the prevention of metabolic syndrome plus the commonly recommended measures to urolithiasis patients.