-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Prevention and Treatment
p-ISSN: 2167-728X e-ISSN: 2167-7298
2016; 5(2): 25-28
doi:10.5923/j.ijpt.20160502.03

Pit Falls in the Management of a Reimplanted Tooth: A Case Report
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAdrita Nag, Puneeta Vohra, Sridevi Koudri
Department of Oral Medicine and Radiology, Faculty of Dental Sciences, SGT University Gurgaon, Haryana, India
Correspondence to: Adrita Nag, Department of Oral Medicine and Radiology, Faculty of Dental Sciences, SGT University Gurgaon, Haryana, India.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Avusion the total displacement of the tooth out of its alveolar socket is a frequent occurrence among the traumatic injuries in the orofacial region, which often is a cause of extreme anxiety due to fear of losing esthetically important teeth. An emergency situation certainly but a prompt treatment ensures a long lasting prognostic value. Through a short case report on the management of avulsed tooth an attempt is made in this article to understand the rationale of management of avulsed tooth.
Keywords: Avulsion, Luxation injuries, Reimplantation, Root Resorption
Cite this paper: Adrita Nag, Puneeta Vohra, Sridevi Koudri, Pit Falls in the Management of a Reimplanted Tooth: A Case Report, International Journal of Prevention and Treatment, Vol. 5 No. 2, 2016, pp. 25-28. doi: 10.5923/j.ijpt.20160502.03.
1. Introduction
- Dental trauma can be arbitrarily divided into two groups: fractures and luxation injuries, among the luxation injuries, avulsions range from 1%-16% of all traumatic injuries of the permanent dentition. [1] Maxillary central incisors are the most frequently avulsed teeth. Although avulsion can occur at any age, the most common age for the avulsion of permanent dentition is 8-12 years and the most common etiological factors at this age, being the fights and sports injuries, a companion of growing up. Management of avulsed tooth often presents an immediate challenge however, fear of losing esthetically vital tooth at all ages presents with apprehension and emergency decisions remarkably impact on overall prognosis of the reimplanted tooth. [2] Reimplantation of the avulsed tooth can restore esthetic appearance and occlusion for a considerable period of time after injury but, post traumatic root resorption can progressively occur, resulting in progressive replacement root resorption with guarded prognosis. The role of oral physician at managing the emergency situation is of prime importance. The success of reimplantation is multifactorial and is dependent to a large extent on the treatment protocol followed by the doctor and cooperation of the patient as a whole. This article reports a short case of management of an avulsed tooth, which resulted in a delayed root resorption after a period of 8 years eventually compromising the esthetics.
2. Case Report
- A male patient aged 22 years reported to department of Oral Medicine and Radiology with a complaint of mobile front teeth since past 2 days. The patient was 14 years old when he fell from a 15 feet high terrace while playing, he suffered injury to his front teeth which resulted in complete avulsion with respect to upper right and left central incisor with profuse bleeding. On advice of a local dentist patient placed the avulsed tooth in cold milk and reported to the Department of emergency, SGT Medical College and Hospital which was at about 3 hours distance from the place of accident. Patient received first aid treatment and the teeth was reimplanted back in the socket after local wound care. The reimplanted tooth was further stabilized using a thin wire (as reported by the patient) taking support from the adjacent front teeth. Patient was advised soft diet before being discharged, after 10 days following this incident patient observed swelling and pus discharge from the same region of trauma. Patient reported back to the same hospital where he was referred to SGT Dental College & Hospital. The reimplanted tooth was removed, the pus was drained and the avulsed teeth was endodontically treated extra orally and then reimplanted. Following which the patient remained asymptomatic for the last 8 years, recently patient observed sudden drifting of teeth causing midline spacing and mobility associated with mild pain.Patient appeared well built and gave no history of any systemic illness, with vital signs in the normal range and afebrile at the time of examination. On examination of the area of chief complaint, spacing of approximately 2mm was observed with a pinkish hue at the cervical third with respect to right side central incisor 11 (figure:1), with grade 3 mobility in relation to right side central incisor 11, and grade 2 mobility with respect to left side central incisor 21 and right side central incisor 11 was found to be out of alignment of the dental arch (figure:2). The teeth were slightly tender on percussion with no vestibular tenderness or obliteration. Based on clinical examination a provisional diagnosis of internal resorption with respect to right side central incisor 11 and localized periodontitis wrt both central incisor 11, 21 with midline spacing due to pathological migration was given. An intra-oral periapical radiograph was advised for investigation, which revealed an ill-defined radiolucent zone appreciated in both central incisors extending from cervical third to the apical third of the radicular portion resulted in ill-defined root anatomy. A well-defined radiopacity confining to the root canals was appreciated which suggested of endodontic restorative material in both central incisors Based on the radiological finding a diagnosis of pathological root fracture was given. Treatment plan included extraction of fractured tooth followed by prosthetic replacement of missing teeth, with immediate placement of implant which had to be delayed due to excessive bone loss in the region.
 | Figure 1. Spacing of approximately 2mm was observed with a pinkish hue at the cervical third wrt right side central incisor 11 |
 | Figure 2. Central incisor 11 was found to be out of alignment of the dental arch (figure:2) |
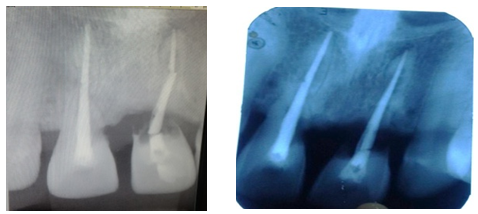 | Figure 3&4. Patient reported after one month with symptom of increased mobility of 11, RVG wrt 21 and 11 revealed pathological fracture wrt 11. (figure:4) |
3. Discussions
- Avulsions occur very often in the anterior teeth of young patients, compromising their aesthetic, mechanical and biological functions lending great impact on the psychosocial status of the patient. Replantation is the first choice of treatment for avulsions under clinical conditions. Interplay of numerous factors will determine the success of treatment, such as intensity of the trauma, vitality of the periodontal ligament, type and time of injury, solutions used for tooth storage in the extra-alveolar period, time elapsed between the avulsion and reimplantation, maintenance of pulp vitality, preparation of the tooth and alveolus for reimplantation, opportunity for endodontic treatment. The damage suffered by the periodontal ligament, such as direct mechanical trauma and dehydration, affects the viability of cells of the periodontal ligament, and worsens the prognostics of the replanted toot. [3, 4]When treating dental trauma, prompt and proper care play the prime role in saving the tooth in many cases. It is, therefore, important for all dentists to have an understanding of how to diagnose and treat the most common dental injuries. This is especially critical in the emergency phase of treatment. The key in proper management of dental trauma is multidisciplinary approach. [5] An informed and coordinated effort from all team members ensures that the patient receives the most efficient and effective care .All luxation injuries will cause some damage to the periodontal ligament and, in some cases, the pulp as well. The immediate treatment is to limit further damage to the PDL and allow for the best possible healing. As with all dental injuries, follow up is essential. Late complications, such as internal or external root resorption and ankylosis are relatively frequent and require endodontic treatment, especially in more severe injuries. As by the recommended guidelines of American association of Endodontics 2011. [2, 4] The time outside of the socket for an avulsed tooth is the most critical factor and determines its prognosis. If the tooth is replanted within 30 minutes, or alternatively kept in a physiological solution of specialized media or milk for a few hours, it has a fairly good prognosis. If the tooth has been dry for more than one hour, the periodontal ligament cannot be expected to survive and the tooth will likely become ankylosed. However in our case the extra alveolar period of the tooth was found to be more than 3 hours. Once reimplanted, most teeth need to be stabilized with a physiological splint for two weeks. If the avulsed tooth has an open apex and was reimplanted within the hour, there is a possibility that the pulp will revascularize. In this case, delaying endodontic treatment at the emergency stage is recommended. Endodontic treatment should only be performed later if signs of pulpal necrosis, root resorption and/or arrested root development are confirmed. [6, 7]In the case of a closed apex, revascularization is not expected. Therefore, endodontic treatment must be initiated two weeks after the tooth is reimplanted, and prior to removal of the splint. Treatment should not be initiated earlier as any further manipulation of the tooth prior to or immediately after reimplantation can cause further damage to the PDL. If the tooth had been kept dry longer than 60 minutes, performing root canal treatment prior to replantation is indicated. After the emergency situation has been managed and the tooth/teeth stabilized, the second phase begins, in which the pulpal condition and likelihood of root resorption have to be carefully evaluated and the patient followed over a period of months, if not years. A follow-up timeline is essential to allow for intervention if signs of complications appear.Avulsed teeth should be replanted in the socket as soon as possible. The long-term success depends mainly on the extra-oral period. Under the circumstances, best results will be achieved if the tooth remains out of the socket for less than 20 minutes. In case the tooth cannot be reimplanted at the place of the accident, it should be stored in special storage media like milk or in a biological medium like Hank’s Balanced Salt Solution (HBSS) to maintain periodontal tissue in as good a state as possible until the patient receives appropriate treatment at a dental office. One of the best and most available mediums in which to store an avulsed tooth is HBSS. It is a form of balanced salt solution (BSS) made to a physiological ph and salt concentration. Solutions may commonly include sodium, potassium, calcium, magnesium and chloride. They provide the cells with water and inorganic ions while maintaining a physiological ph, and osmotic pressure. Milk to be remembered as, another recommended medium, though not as good as the HBSS but its osmolality and ph is within acceptable biological range, also it has been reported that milk preserves the periodontal ligament cells up to six hours is easily available. In order of priority, sterile saline is the next medium to be used, even though it cannot easily be found in public places. [6, 8]Fully developed teeth with an extra oral dry time of 1 hour or less or teeth stored in a biological medium should be treated carefully to avoid further damage to the root surface and remaining periodontal ligament tissues. The tooth should be held by the crown, irrigated with sterile saline, and replanted with a gentle digital pressure. In cases of teeth with a partial development of the root, it is recommended to soak the tooth in Doxycycline 0.005% for 5 minutes before replantation. It was found that pulp revascularization was significantly enhanced in up to 40% to 60% of the treated cases. [9, 11]Teeth with more than 60 minutes extraoral dry time; It can be assumed that, in cases of avulsed teeth stored in dry conditions for more than 1 hour, the periodontal ligament (PDL) will be necrotic and, consequently, replacement root resorption is expected to develop. To attenuate or slow down the resorption process, it has been recommended to follow a root preconditioning protocol. Damage to the socket during the replantation is directly related to the long-term success of the treatment. The socket should be rinsed with sterile saline. If the alveolar bone has collapsed, it should be repositioned gently. The use of an air syringe should be avoided to dry the socket. After all the aforementioned treatment is performed, the tooth should be repositioned very gently in the dental socket with a light digital pressure. The tooth is further stabilized with semi rigid splints for a period of 7-10 days. The administration of systemic antibiotic prevents the development of external root resorption by preventing the bacterial invasion of the necrotic pulp, thus reducing the inflammatory root resorption. The antibiotic of choice is Amoxicillin 500 mg × 3/day for 7 days (children=50 mg/kg/day in divided doses every 8 hours). Doxycycline 100 mg × 1/day for 7 days (children=2 mg/ kg/day) has also been successfully used in cases of avulsion. Oral hygiene measures must be strictly followed and the patient should be advised a soft diet. In cases of incomplete root development and extraoral dry time greater than 60 minutes, tooth replantation is not recommended as in such situations replacement root resorption can take place which results in ankylosis in many patients. [1, 3, 7]
4. Conclusions
- Several factors unfortunately may have contributed in the ultimate extraction of the reimplanted tooth in the case reported. Reimplantation if attempted by the local dentist if not the reimplantation of the avulsed tooth, at least the knowledge of transferring the avulsed tooth to a better medium like HBSS would have noticeably improved the prognosis in our case also reducing the extra oral time. At the emergency department although local wound care was provided and the tooth was reimplanted antibiotic cover was not advised thus resulted in infection and pus discharge within 10 days further affecting the prognosis in terms of duration of successful reimplantation. However endodontic therapy that was carried out subsequently, contributed to a large extent to the period of functional and aesthetic role the teeth played for a period of 8 years. Lack of follow up on the part of patient might have played a significant role in subsequent resorption and ultimate loss of teeth. The loss of tooth structure in the cervical third of tooth gave a pinkish colour to the crown of tooth, and the resorption of roots resulted in pathological fracture of the teeth. The role of an oral physician is of paramount importance in deciding the treatment protocol, however the teeth served its purpose for a long period of 8 years, but had to succumb to its fate, if only it could be retained longer in a functional state.
ACKNOWLEDGEMENTS
- To all my teachers of past present and future in this.