-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Prevention and Treatment
p-ISSN: 2167-728X e-ISSN: 2167-7298
2016; 5(1): 1-6
doi:10.5923/j.ijpt.20160501.01

Radial Shockwave Therapy Improves Pain, Range of Motion, Strength, and Function in Patients with Chronic Lateral Epicondylitis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLPaolo Sanzo
School of Kinesiology, Lakehead University, Canada
Correspondence to: Paolo Sanzo, School of Kinesiology, Lakehead University, Canada.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Objective: Lateral epicondylitis (LE) is characterized by inflammation and later degenerative angiogenetic changes of the wrist extensors. The optimal treatment of LE remains elusive with contradictory findings reported. The purpose of this study was to assess the effects of radial shockwave therapy (RSWT) on function, range of motion (ROM), strength, and pain in patients with chronic LE. Methods: Functional status using the Upper Extremity Functional Scale (UEFS), ROM, strength, and pain was measured with the P4 Scale and Visual Analog Scale (VAS) before and 3 months post-treatment. Twenty-eight subjects received 3 treatments (2000 shockwaves, 2.5 bars, 10-15 Hz, 11.5 Mp) on the painful elbow. A Wilcoxen Signed Rank Test and Dependent t-Test was used to analyze the data. Results: There was no significant improvement in VAS pain score at rest (p=.142) and in grip strength (p=.319). There was statistically significant improvement in VAS scores for pain after activity (p=.0001) and overall improvement in pain (p=.0001); P4 Scale scores (p=.0001); UEFS scores (p=.0001); elbow flexor (p=.014) and extensor (p=.008) ROM; elbow flexor, extensor, supinator, and pronator strength (p=.008); and wrist flexor, extensor, radial deviator, and ulnar deviator strength (p=.003). There was no statistically significant improvement in ROM for all other elbow and wrist movements. Conclusions: The use of RSWT is an alternative and effective treatment option for patients diagnosed with chronic LE. This intervention resulted in a reduction in elbow pain and an improvement in function, ROM, and strength in the elbow and wrist.
Keywords: Radial shockwave therapy, Lateral epicondylitis, Pain, Range of motion, Strength, Function
Cite this paper: Paolo Sanzo, Radial Shockwave Therapy Improves Pain, Range of Motion, Strength, and Function in Patients with Chronic Lateral Epicondylitis, International Journal of Prevention and Treatment, Vol. 5 No. 1, 2016, pp. 1-6. doi: 10.5923/j.ijpt.20160501.01.
Article Outline
1. Introduction
- Patients presenting with lateral elbow pain are often diagnosed and labelled using a variety of terms to explain the same disorder. What is commonly referred to as Tennis Elbow, or Lateral Epicondylitis (LE) was first described in 1873 as Writer’s Cramp and later in 1883 as Lawn Tennis Elbow [30]. The terminologies used to describe this disorder have created some confusion and are not consistent with the underlying pathogenesis and cause since this disorder is neither inflammatory nor does it commonly occur in tennis players [32].Lateral epicondylitis is one of the most common causes of elbow pain with an annual incidence of 1-3% in the general population [23, 30, 32] and 15% in the work force [31]. The peak onset often occurs during the fifth to sixth decades of life [23, 31] with equal incidence between males and females [31, 32]. Often, the dominant elbow is affected more than the non-dominant side with a higher incidence in the non-athletic population [31]. This often results in lost work time with significant direct and indirect healthcare costs [23]. Patients often present with subjective elbow pain and palpable tenderness localized to the lateral epicondylar and wrist extensor region [1]. Decreased grip strength and the decreased ability to complete daily functional and sport specific tasks are often reported. Another common complaint is pain with repeated forearm supination or pronation movements completed with the elbow positioned at or near full extension [1, 31]. Other reported causes of LE include overload, age related degeneration, micro-trauma, and overuse [31]. Although the actual cause of LE is not known, a correlation has been reported between the development of LE and specific repetitive movements performed for two hours per day, handling tools greater than 1 kg, handling loads greater than 20 kg at least 10 times per day, low job control, and the lack of social support at work [7].The pathogenesis associated with LE may be affected by a variety of factors as described above causing the tissues to progress through the inflammatory, degenerative angiogenetic, fibrotic, and calcific stages [24, 31]. Various treatments have been proposed for each stage ranging from conservative to surgical during each of these stages but the optimal treatment remains elusive.Often, LE is a self-limiting disorder that may resolve irrespective of the treatment used [2]. Approximately 90% of patients will recover within a 12 month period of time and the remainder recovering within a 12 to 18 month period [7, 24]. Fifty percent of LE patients, however, that do not respond to conservative treatment consult with an orthopedic surgeon with 12% having some form of surgical intervention [30]. Proposed conservative treatments range from the use of therapeutic exercise such as eccentric strengthening, electrotherapeutic modalities including ultrasound therapy, transcutaneous electrical nerve stimulation, laser, and shockwave therapy, to pharmacological interventions [6, 7]. The available research on the use of radial shockwave therapy (RSWT) treatment for LE have revealed contradictory results. Prior systematic reviews regarding the effectiveness and use of shockwave therapy support the notion that shockwave therapy is safe and technically easy to perform and helpful in certain orthopedic conditions [21]. Many of these reviews on shockwave therapy, however, are dated and have added to the already pre-existing confusion due to the diverse terminology, protocols, energy levels, and treatment parameters used [20, 24, 30, 32]. Several authors have reported positive and beneficial effects when using shockwave therapy in the treatment of LE [9, 15, 17, 18, 26]. Conversely, contradictory findings have been reported in other randomized controlled trials, systematic reviews, and meta-analyses highlighting the need for further investigations [2, 4, 7, 13, 20, 24, 32]. Therefore, the purpose of this study was to assess the effects of RSWT on function, range of motion (ROM), strength, and pain in patients with chronic LE.
2. Methods
2.1. Subjects
- Participants included 28 individuals (12 females and 16 males) diagnosed with chronic LE. Descriptive data for age, height, weight, and the duration of the symptoms is summarized in Table 1.
|
2.2. Apparatus
- A long arm Baseline® Absolute-Axis™ plastic goniometer was used to complete all of the ROM measures. The use of goniometric measurements have strong evidence of reliability and validity and is an important prerequisite for assessment in clinical practice, as well as for the collection and interpretation of research results. This method of ROM measurement has been reported to be an accurate, valid, and reliable method of determining elbow and wrist joint mobility [3, 19, 11, 14]. Grip strength was measured using a Jamar hand dynamometer and has also been reported to be a valid and reliable measure in patients with LE [25]. A Storz D-Actor 100© RSWT unit was used for the treatment for all participants.
2.3. Procedure
- Once the project received ethical approval by the university ethics board, the purpose and methodology of the study was explained and consent to participate was obtained, anthropometric measures were taken and self-report outcome measures completed. Age, height (cm), weight (kg), and length of time that the pain was present (weeks) was recorded.Functional status was measured using the Upper Extremity Functional Scale (UEFS). The UEFS is a 20-item self-report questionnaire that is scored on a 5-point Likert scale (0 to 4) and is used to assess upper extremity functional status on a variety of conditions and levels of severity [16, 28]. The total calculated UEFS score ranges from 0 to 80 with higher scores indicating greater functional ability. The UEFS has been validated in upper extremity dysfunction and post-surgical patients with a test-retest reliability ICC of .85-.95 reported [28].Elbow pain was measured using a visual analog scale (VAS). The subject was asked to consider the following questions when filling out the linear VAS scale: (1) his/her level of elbow pain at rest; (2) his/her level of elbow pain following activity; and (3) his/her overall improvement in elbow pain. Overall improvement was defined as the change in elbow pain level from the onset of treatment related to the study with subjects considering the pre-treatment overall improvement score as being zero. Subjects marked the VAS at the point that corresponded to his/her pain intensity or overall improvement level. The amount of pain or overall improvement level was estimated by measuring in millimeters the distance from the “no pain” marker to the mark provided by the subject for each question. The VAS has been shown to have good validity, reliability, and psychometric properties. The reported test-retest reliability for the VAS ranges from .71-.99 [8, 22] and the pooled value for construct validity ranges from .71-.98 [10, 29].Elbow pain was also measured using the P4 Scale. The P4 is a four item self-report questionnaire scored on an 11-point Likert scale (0 to 10). The total P4 Scale score ranges from 0 to 40 with higher scores indicating greater pain. It has a reported internal consistency of .90-.92 and test-retest reliability of .79-.81 [27]. This alternate measure was also used in order to examine changes in elbow pain and prevent any ceiling or flooring effects that may occur when using a VAS. The minimal detectable change for the VAS has been reported to be a change in ±2.8 mm [5] so if a participant reported a starting score of less than 2.8 or greater than 7.2, the VAS may not be sensitive enough to detect pain changes; whereas the P4 Scale has a larger score range and may provide an alternate measure without some of the described limitations at the extremes of the VAS.After the self-report measures for pain and function were completed, active ROM and strength of the elbow and wrist were assessed with the participant in sitting. Active ROM for the wrist and elbow joints were measured and recorded in degrees using a Baseline® Absolute-Axis™ goniometer. Resisted isometric strength of the elbow and wrist was measured, graded, and recorded using the 5-point Oxford scale (grade 5 - movement against gravity with full resistance; grade 4 - movement against gravity with some resistance; grade 3 - movement against gravity only; grade 2 - movement with gravity eliminated; grade 1 - visible and palpable muscle contraction but no movement and; grade 0 - no contraction).After the baseline pre-treatment measures were completed, the subject was treated with RSWT. Each subject received 2000 shockwaves set at an intensity of 2.5 bars, 10-15 Hz, and 11.5 Mp using a Storz D-Actor 100© RSWT unit. The applicator was positioned so that treatment was completed over the painful region of the elbow over the lateral epicondyle without the use of anesthesia to the region. Each subject received three treatments in total spaced one week apart over a three week period of time. Elbow and wrist ROM and strength and the UEFS, P4, and VAS for elbow pain at rest, after activity, and for overall improvement were measured again three months post-treatment. A Wilcoxen Signed Rank Test and Dependent t-Test were used to analyze the data comparing pre-treatment to post-treatment scores.
3. Results
- After completing the pre-test evaluations and receiving three treatments of RSWT, the 28 participants with chronic LE completed the post-test evaluations at three months post-treatment. The Wilcoxen Signed Rank Test revealed that following the RSWT intervention, participants did not have a statistically significant improvement in elbow pain on the VAS at rest (Z=1.52, p=.142); however, there was a statistically significant improvement in elbow pain after activity (Z=4.85, p=.0001); and for overall improvement in elbow pain (Z=-5.25, p=.0001) (figure 1). Similarly, a Wilcoxen Signed Rank Test revealed that following the RSWT intervention, participants had a statistically significant improvement in elbow pain reported on the P4 Scale (Z=5.176, p=.0001) (figure 2). An improvement in function was also found with the Wilcoxen Signed Rank Test for the UEFS scores (Z=-4.057, p=.0001) (figure 3). A statistically significant improvement in elbow ROM for flexion (p=.014) and extension (p=.008) was found. There was no statistically significant improvement in elbow ROM for supination (p=.10) and pronation (p=.10). There was also no statistically significant improvement in wrist ROM for flexion (p=.477); extension (p=.369); radial deviation (p=.10); and ulnar deviation (p=.10).
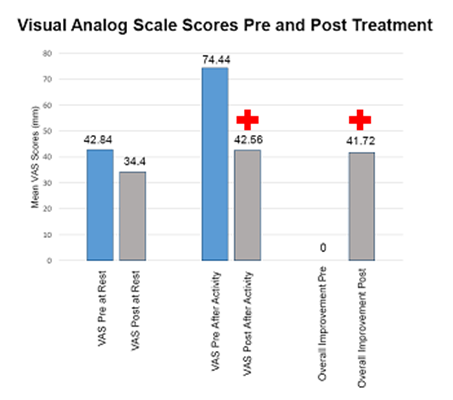 | Figure 1. Mean visual analog scale scores pre- and post-treatment for elbow pain at rest, elbow pain after activity, and overall improvement in elbow pain ( indicates statistical significance) indicates statistical significance) |
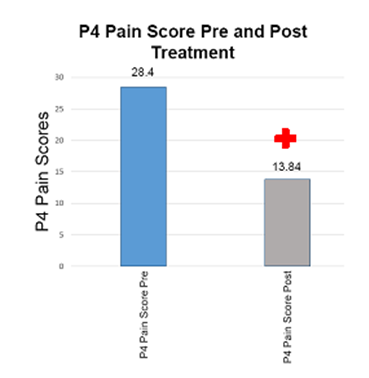 | Figure 2. Mean P4 Pain Scores pre- and post-treatment ( indicates statistical significance) indicates statistical significance) |
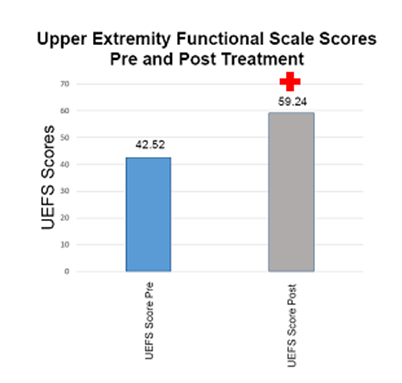 | Figure 3. Upper Extremity Functional Scale scores pre- and post-treatment ( indicates statistical significance) indicates statistical significance) |
4. Discussion
- This study examined the effects of RSWT on function, ROM, strength, and pain in patients with chronic LE. The results revealed that RSWT improved overall elbow pain and pain after activity. It was also evident that RSWT improved elbow flexor and extensor ROM and elbow and wrist strength. Radial shockwave therapy has been reported to be an effective treatment in some trials and ineffective in others, but the evidence and efficacy remains controversial [21, 24, 31]. The results of this study add to the merit and body of literature supporting the use of RSWT clinically for chronic LE.In some cases, RSWT has been reported to produce no effects or the same results as placebo or sham treatment [4]. In other clinical trials, shockwave therapy has been reported to be an effective treatment for LE [9, 13, 15, 17, 18, 26]. It has also been reported that RSWT is equally effective in the treatment of both acute and chronic LE and has been proposed to limit the progression of acute cases to the chronic phase with this treatment [13]. This is contrary to some of the reported findings suggesting that optimal treatment should incorporate a wait-and-see philosophy. This approach recommends simply educating the patient that this problem is self-limiting and will likely resolve on its own. It has been proposed that this simple observation and reassurance of the patient is a practical and cost effective management strategy for patients [20]. Does this mean that clinicians should not offer patients treatment in the short term if the evidence is contradictory or if the suggested treatments offer only short term relief? In an effort to integrate best practices, some clinicians and clinical researchers, sometimes forget that the primary goal of treatment is to improve the overall quality of life for our patients and help them to ultimately recover [2]. The findings of the current study support the use of RSWT for patients with chronic LE especially if elbow pain and elbow ROM and strength issues are present.The clinician attempting to critically analyse the available literature and determine if this is a useful treatment option, needs to be aware that determining the utility of this modality and whether treatment is effective or not may be related to the length of follow up for that patient or whether the elbow pain was acute versus chronic in nature [7, 13]. Other determining factors that have been reported to impact on the success of the treatment include if a worker’s compensation claim is present or if a prior injection was completed in the area [12]. If there is the presence of neurological involvement of the radial nerve, previous orthopedic surgery to the region, and the duration of symptoms of greater than 12 months were also predictors that conservative treatment may be ineffective and surgery may be indicated [12]. Our findings support the use of RSWT for chronic cases as the participants had a mean duration of 127 weeks. Similarly, participants in the current study did not have any neurological symptoms and prior surgery to the area, and were followed for a period of 3 months post-treatment and this is also consistent with the above recommendations when considering RSWT. So for the clinician considering the use of RSWT for the treatment of chronic LE, the integration of the above factors and predictors and selectively using this therapeutic modality may help with the overall success of the treatment.Clinicians reviewing the available clinical trials, systematic reviews, and meta-analyses must cautiously review the findings reported as several design and methodological questions arise. In some cases, no significant differences have been identified and systematic reviews have not supported the use of RSWT in the treatment of LE and various other conditions [2, 4, 7, 13, 20, 24, 32]. In some of the systemic reviews examining the effects of RSWT on LE, the reviewers did not take into consideration the differences between generation principles; the useful effects of local anesthesia and how this negatively impacted on the treatment outcome; or the fact that comparisons were made between acute and chronic cases and the fact that these may respond differently to treatment [30]. Other factors that have affected the reviews available is the fact that many studies used different shockwave generators and different treatment protocols but were still clustered together for the purpose of review and also the fact that even the sham group, in many instances, received shockwave therapy treatment as well but at what was described as a sub-therapeutic dosage and then labelled as a sham/placebo group [30]. These extrinsic and research design factors may help to further explain the lack of support for positive treatment effects and the reasoning and rationale behind the confusion. Although the current study did not incorporate a control or placebo group, the parameters and device used has been clearly explained and is consistent with recommendations made in the available literature [21] and clearly resulted in positive effects post-treatment.The limitations of the present study included the lack of a placebo or control group and small sample size. The design of the perfect clinical trial is a challenge from a design perspective but future studies should include a larger sample with the inclusion of a control/placebo group with a longer follow up period (6, 12, or 24 months). Similarly, combination of treatments such as the use of eccentric strength training in isolation and combined with RSWT or comparing this to a wait and see group may provide valuable insight and simulate what actually occurs in the clinical environment. This also will assist with knowledge translation in bringing the information from the bench to the bed side and simulating more true clinical applications of multimodal treatment applications. This will also aid in the development of clinical trials that can be used for future systematic reviews and meta-analyses that may further critically assess and reflect the effects of RSWT in the treatment of chronic LE.
5. Conclusions
- The use of RSWT is an alternative and effective treatment option for patients diagnosed with chronic LE. This intervention resulted in a reduction in elbow pain and an improvement in function, ROM, and strength in the elbow and wrist. Future research using multi-site and larger sample sizes, implementing a true placebo or control group, and possible multimodal treatment interventions is required.