-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Prevention and Treatment
p-ISSN: 2167-728X e-ISSN: 2167-7298
2015; 4(1): 8-13
doi:10.5923/j.ijpt.20150401.02
Sexual Behaviour, HIV/Stiprevention Knowledge, and Utilisation of Vct among the Residents in Sagamu Metropolis of Ogun State, Nigeria
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLIlesanmi Ayodele Olusola1, Ezeokoli Rita Nkiruka2, Obasohan M. O.2, Ayodele Kolawole Olanrewaju3, Olaoye Titilayo4
1Medical Laboratory Science Department, Babcock University Ilishan, Ogun State, Nigeria
2Social Work Department, Babcock University Ilishan, Ogun State, Nigeria
3Research and International Cooperation (RIC), Babcock University Ilishan, Ogun State, Nigeria
4Public Health Department, Babcock University Ilishan, Ogun State, Nigeria
Correspondence to: Ayodele Kolawole Olanrewaju, Research and International Cooperation (RIC), Babcock University Ilishan, Ogun State, Nigeria.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
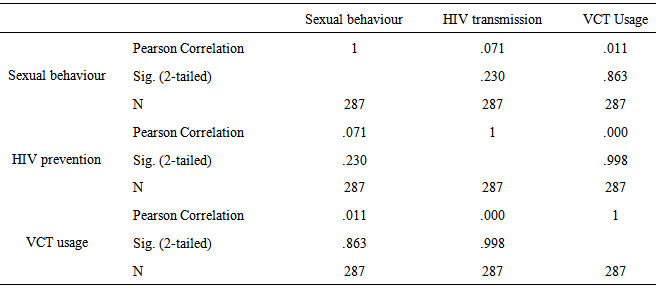
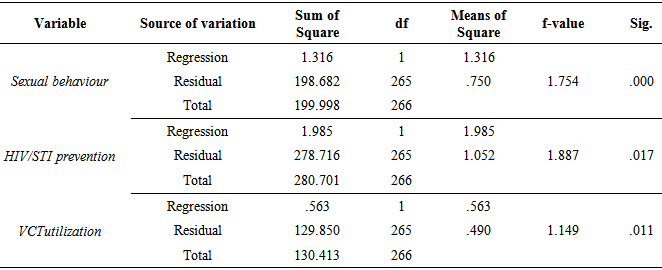
Voluntary Counseling and Testing (VCT) has been seen as a viable tool in curbing permissive sexual behaviour as well as controlling the spread of HIV/AIDS. The aim of the study was to assess and compare the sexual behaviour, HIV preventions knowledge, and VCT utilization among the residents in Sagamu metropolis with the aim of identifying aspects requiring interventions. The study adopted a descriptive cross-sectional design in order to assess the knowledge, perceptions, attitudes and use of voluntary counselling and testing among the residents of Sagamu metropolis of Ogun State in Southwest Nigeria. In this study, a total of 287 participants stratified based on their professions (traders, students, and civil servants) were involved. A self-developed instrument tagged “Knowledge, Perceptions, Attitudes and the use of VCT Questionnaire (KPAVCTQ)” was used data collection. Data analysis was done with descriptive statistics, Pearson Product Moment Correlation, and Multiple Regression Analysis. The results showed a direct relationship between participants’ sexual behaviour and STI preventions (.071), as well as VCT usage (.011); significant moderating influence of demographics was found on the relationship between sexual behaviour, VCT usage and STI preventions. Also, it was revealed that the participants did not differ significantly in their sexual behaviour (F (1,266) = 1.754; P < .05), HIV/STI prevention knowledge (F (3,266) = 1.887; P < .05), and VCT utilization (F (3,266) = 1.149; P < .05) for health purpose. This study underscores the need for the Nigerian society to focus attention on issues that are of some consequences to human sexual health knowledge, social functioning and mental health development.
Keywords: Sexual behaviour, HIV preventions knowledge, VCT utilization
Cite this paper: Ilesanmi Ayodele Olusola, Ezeokoli Rita Nkiruka, Obasohan M. O., Ayodele Kolawole Olanrewaju, Olaoye Titilayo, Sexual Behaviour, HIV/Stiprevention Knowledge, and Utilisation of Vct among the Residents in Sagamu Metropolis of Ogun State, Nigeria, International Journal of Prevention and Treatment, Vol. 4 No. 1, 2015, pp. 8-13. doi: 10.5923/j.ijpt.20150401.02.
Article Outline
1. Introduction
- When Human Immunodeficiency Virus/Acquired Immunodeficiency Syndrome (HIV/AIDS) was first mentioned in the 1980s, few people could imagine what an international plague this virus could be. Though the disease is completely preventable, thousands of people die each day and the numbers continue to rise. East and southern sub-Saharan Africa is the world’s “hot spot” for HIV/AIDS [1]. The low prevalence of HIV and AIDS in the developed countries is partially due to a number of factors: increased awareness by the inhabitants, pro-active government policies, and access to quality healthcare services, positive attitude and minimal incidents of stigmatization among the populace. On the contrary, low literacy level, mystification of disease, poor perception, poverty, lack of access to quality healthcare and stigmatization have all contributed to the high prevalence found in surveys conducted for HIV/AIDS in developing countries [1-5].Africa has been nicknamed the hotbed of HIV infections due to the high infection and mortality data [1, 5], although severity is more pronounced in the South and East Africa. The pro-HIV factors identified above are a common phenomenon in most African countries, yet people there continue to engage in risky sexual behaviors due to a lack of knowledge about the disease and how it is transmitted, cultures that discourage the use of condoms, societal denial, and a low perceived susceptibility of acquiring the disease.HIV/AIDS is a terminal disease. Although no permanent cure has been found but there is aprovision of antiretroviral drugs that assist in prolonging the life of those who have been infected. Knowledge of one’s HIV status is a first step to facilitate accessing care and preventing further infection, and thereby controlling the HIV epidemic [6]. One of the strategies ascertaining one’s HIV status is counselling and testing (VCT).VCT is one among different approaches which have been implemented as an attempt to slow the spread of HIV infection and minimize its impact at the individual, family and society level [7]. VCT for HIV is recognised globally as an effective and pivotal strategy for both preventive and care in HIV/AIDS. Counselling and testing centers are places where people go to know more about HIV and AIDS and / or to check their sero-status so as to make informed decisions about their health and behaviour [8].Studies have also shown that awareness of the existence of HIV/AIDS is relatively high but knowledge about prevention, care and support is low. Myths and misconceptions on HIV/AIDS have also been noted [9]. Some studies in Nigeria have revealed that there is poor knowledge of HIV/AIDS among traders, despite the high awareness of the disease [2, 3]. Thus, VCT services are an important avenue to receive important information about HIV/AIDS. This is further substantiated in a research carried out by Cartoux, Msellati, Meda, Welffens-Ekra, Mandelbrot, Leroy, Van de Perre, and Dabison pregnant women [10]; some of the women took the test but failed to return for the test results for various reasons. However, in other studies, the majority (81%) of the participants returned for their test results following counselling and testing [9]. In Nigeria, several campaigns have been mounted to increase awareness to HIV/AIDS. These include radio and television jingles, rallies, school HIV/AIDS clubs, campaigns mounted by non-governmental organisations (NGOs) at community level, etc. These campaigns, started more than two decades ago, are yet to impact the HIV statistics significantly, although it seems to hover about the same level [11]. Evaluation of the awareness of counseling and testing for HIV holds the key for appropriate interventions in communities. According to WHO, testing and counseling services are a gateway to HIV prevention, care and treatment [12]. This is because it is beneficial for the individual, the community and the larger populace. Also, Ezeiru and Odeyemiobserved that health education, particularly periodic HIV/AIDS education could be one of the strategies in reducing stigmatization and discrimination among the victims of HIV/AIDS and those living around them. Before any intervention however, on-spot situation assessment is vital [5].For the purpose of service delivery, it is important to consider reducing the barriers to access to VCT services for vulnerable populations such as women, students, sex workers, refugees and prison populations [13]. Morin, Khumalo-Sakutukwa, Charlebois, Routh, Fritz, Lane, Vaki, Fiamma, and Coates carried out a study to evaluate a strategy to remove barriers of knowing one’s HIV status by implementing a mobile VCT service that provided free, anonymous rapid testing in public market places in a rural community and a high-density community in Zimbabwe [14]. The majority of the participants (99%) elected to receive HIV test results the same day. Reasons for not testing previously were convenience of location / hours and cost. One could argue that participants could have potential problem with testing in public places or settings. Their finding revealed that those who used same day mobile testing services perceived themselves at higher risk for HIV infection.AIDS related stigmas are another factor that probably influences seeking VCT. Stigmatizing beliefs about AIDS and their associated fears of discrimination can influence decisions to seek HIV testing and HIV treatment services. Stigmas may therefore pose considerable barriers to seeking VCT [15, 16].Due to the busy nature of some occupations, certain groups ought to be specifically targeted for assessment and intervention in the community. Among these groups are traders and workers, who usually leave their respective homes very early and return late, due to the nature of their means of earning a livelihood, and also students who are young and easily influenced by peer relationships. Although awareness may be high about HIV among these groups, the actual knowledge and perception may be a different issue altogether [2, 3]. This study therefore sought to assess and compare the sexual behaviour, HIV preventions knowledge, and VCT utilization among the residents in Sagamu metropolis with the aim of identifying aspects requiring interventions.
2. Research Questions
- In order to achieve the purpose of the study, the following research questions were generated;1.Would there be any significantinter-relationship between the sexual behaviour, HIV preventions knowledge, and VCTutilization among the residents in Sagamu metropolis?2. Would there be any significant moderating influence of demographics on the relationship between sexual behaviour, VCT usage and STI preventions among the residents of Sagamu metropolis?3. Would there be any significant difference in the participants’ sexual behaviour, HIV/STIprevention knowledge, and VCTutilization for health purpose?
3. Research Method
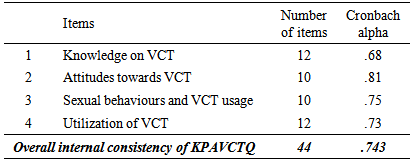
- Research Design: This study adopted a descriptive cross-sectional design in order to assess the knowledge, perceptions, attitudes and use of voluntary counselling and testing among the residents of Sagamu metropolis of Ogun State in Southwest Nigeria. The study was conducted in September 2014 in Sagamu, the economic center of Sagamu local government area of Ogun State.Population: The accessible population in this study included all the public/civil servants, traders, secondary school students. This includes male and female, educated and illiterates, as well as those from high/average socio-economic class and low socio-economic class. The inclusion criteria were those who were willing to participate in the study, while those who were willing to participate in the study were excluded.Sampling Technique: Stratified random sampling technique was used to select the sample for this study. Probability sampling was used because it increased the likelihood that all the elements in the population would have an equal chance of being included in the sample. The participants were stratified based on their professions (traders, students, and civil servants). After stratification, a proportional simple random sample was obtained by selecting participants randomly from the sampling frame until the intended sample size was attained. The sample includes a total of 300 participants, 100 each from each stratum.Measures: The name of the tool is “Knowledge, Perceptions, Attitudes and the use of VCT Questionnaire (KPAVCTQ)” which was developed by the investigators. The total numbers of items in the Scale were fifty four. Thirty-four items out of fifty four items of the questionnaire were with three options. These options were “YES”, “NO” and “DON’T KNOW”. The response of a participant was registered by making a tick mark against anyone of the above options of a single item. The other twenty items were with four options ranging from ‘not likely at all’ to ‘very likely’. The internal consistency measured by Cronbach alphas for overall KPAVCT Questionnaire and for Knowledge, Perceptions, Attitudes and the use of VCT sub-scales are 0.74, 0.68, 0.81, 0.75, and 0.73 respectively.
4. Data Analysis
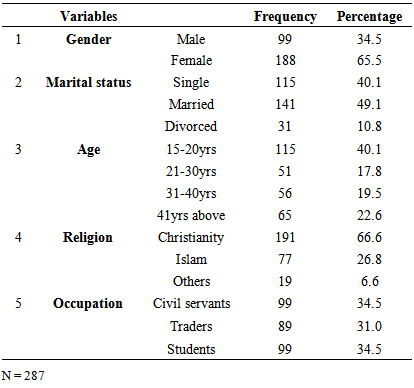
- Data were edited, cleaned, coded, entered and analysed using the Statistical Package for Social Sciences (SPSS) version 19 software program. Data were summarised by means of descriptive statistics including the frequency table.
5. Results
|
|
|
|
|
6. Discussion
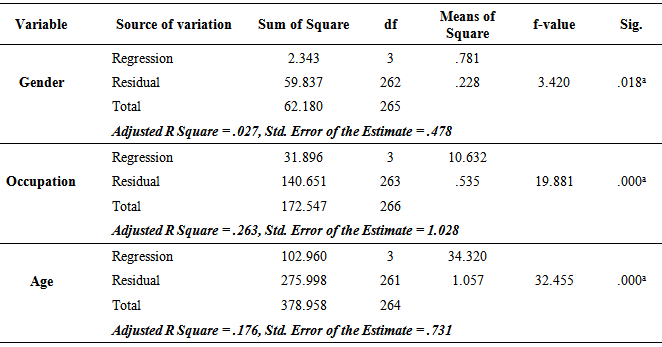
- This study sought to assess and compare the sexual behaviour, HIV preventions knowledge, and VCTutilization among the residents in Sagamu metropolis. This research theme is hinged on the need to provide an empirical basis for the improvement of mental health of the people on the adequate utilization of VCT among the residents of Sagamu Metropolis in Ogun State Nigeria with the aim of identifying aspects requiring interventions.The finding on the relationship between the participants’ sexual behaviour, VCT usage and STI preventions indicated significant positive relationships among the variables of the study. This is also in agreement with Akindele-Oscar and Ayodele; Ogunsanwo and Ayodele who revealed that lack of knowledge of sexual health behaviour have a significant relationship with permissive sexual expressions [17, 18]. This tend to show, that engaging in casual sex was not necessarily always a deliberate choice, often times it was due to lack of adequate sexual health knowledge or complete ignorance on the subject matter.This finding has demonstrated the moderating influence of demographics (gender, age, occupation) on the relationship between sexual behaviour, VCT usage and STI preventions among the participants. Among the three demographical factors, age was found to have more influence on participants’ sexual behaviour, VCT usage and STI preventions. This result is in agreement with the outcome of many research studies affirming that gender [19-21] and age [22, 23] to some extent are demographical factors that have direct and indirect impact on outcome variables such as behavioural change.The finding does not only demonstrate the moderating influence of demographics in determining the relationship between sexual behaviour, VCT usage and STI preventions among the participants, it also affirms the significant indifference in the participants’ sexual behaviour, HIV/STI prevention knowledge, and VCT utilization for health purpose. Since the long term objective of the study is to determine the differential behaviour of participants’ sexual behaviour, HIV/STI prevention knowledge, and VCT utilization, thereby leading to better sexual behaviour and sexual mentality in Ogun State, Nigeria. This finding is therefore in agreement with the ones reported by Ayodele and Akindele-Oscar, Ogunsanwo and Ayodele, and Ogunsanya that sexual behavior depends not only on learning and pleasurable reinforcements but also on opportunities and limitations including those established by the individual’s own standards, concepts, perception, and wellbeing [17, 24, 25]. Also, the study of Ogunsanwo and Ayodele showed that individual sexual health behaviour was influenced by psychological wellbeing, emotional intelligence, and locus of control [18].
7. Implications and Recommendations
- The findings of this study underscore the need for the Nigerian society particularly urban communities, semi-urban communities, rural communities and families to focus attention on issues that are of some consequences to human sexual health knowledge, social functioning and mental health. Poor sexual behaviour, HIV/STI prevention knowledge, and VCT utilization to a large extent affect the quality of individuals’ sexual health knowledge, social functioning and mental health. To this extent, government and policy maker may need to take seriously their share of responsibility in educating the citizenry on sexual health knowledge. Presently the state of sexual behaviour in the community examined is very poor. As noted by Ayodele and Akindele-Oscar there is need for government, school management and/school counselors (counseling psychologist) [24], and various work organization to design quality programs at different level of life that will enhance positive sexual behavior among the community members – families, workers, and students at all levels, promote better interpersonal relationship skills, psychological functioning, and through skill building programs such as sex education, interpersonal communication, critical thinking and problem-solving skill trainings, and the likes.Governments and community leaders need to be conscious of how improve and increase individual’s social and psychological functioning which may lead to enhanced interpersonal and intrapersonal relationship. This in turn will promote a meaningful and fulfilled life among the citizenry regardless the age, gender or work status. This is important because the perception of sex and sexual behavioral patterns are manifestation of some psycho-sociological dispositions deepened within the society cultural milieu in which the individuals find themselves.