-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Probability and Statistics
p-ISSN: 2168-4871 e-ISSN: 2168-4863
2014; 3(2): 30-34
doi:10.5923/j.ijps.20140302.02
Treatise on Anaemia in Pregnancy in Women of Reproductive Age in the Bolgatanga Municipality, Upper East Region, Ghana
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSuleman Nasiru, Luguterah Albert
Department of Statistics, Faculty of Mathematical Sciences, University for Development Studies, P. O. Box 24, Navrongo, Ghana, West Africa
Correspondence to: Suleman Nasiru, Department of Statistics, Faculty of Mathematical Sciences, University for Development Studies, P. O. Box 24, Navrongo, Ghana, West Africa.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
This study investigated the prevalence of anaemia in pregnancy and the determinants of haemoglobin levels and anaemic status among pregnant women. The results showed that 50.4% of the subjects were anaemic. The GLM and the binary logistic regression results revealed that Blood pressure, Gestational Age and BMI are useful in determining the haemoglobin level and the anaemic status respectively. The binary logistic regression revealed that a subject with normal blood pressure is 64.4% less likely to be anemic compared to a subject with abnormal blood pressure. Also, for a unit change in BMI a subject is 7.3% less likely to be anaemic while for a unit change in gestational age a subject is 6.5% more likely to be anaemic. The results revealed that as the Gestational age increases the probability of a subject becoming anaemic increases. It is therefore recommended that medical experts should advise pregnant women to take in foods and or supplements that will increase their Haemoglobin level as the Gestational age increases.
Keywords: Anaemia in pregnancy, Bolgatanga, Haemoglobin level, GLM, Logistic regression
Cite this paper: Suleman Nasiru, Luguterah Albert, Treatise on Anaemia in Pregnancy in Women of Reproductive Age in the Bolgatanga Municipality, Upper East Region, Ghana, International Journal of Probability and Statistics , Vol. 3 No. 2, 2014, pp. 30-34. doi: 10.5923/j.ijps.20140302.02.
Article Outline
1. Introduction
- Anaemia in pregnancy is one of the detrimental diseases that have usurped the minds of Public Health Workers globally. It is one of the major causes of high maternal mortality and morbidity, neonatal mortality and high percentage of low birth-weight worldwide [5, 3]. According to [14], anaemia is a result of having haemoglobin levels of less than 11g/dl and affects nearly half of all pregnant women in the world: 52% in developing countries and 23% in the developed countries. In Ghana, the prevalence of anaemia among pregnant women increased from 65% to 70% between 2003 and 2008. Anaemia in pregnancy is one of the major causes of the unacceptable high maternal mortality ratio of 451 per 100, 000 live births in the country. It is responsible for 20% of the maternal deaths in the country [6].In order to address this canker, the determination of factors that contributes to anaemia in pregnancy in a population is imperative for the implementation of control measures. Various risk factors including inadequate nutrition, infection, age, sickle cell status and poor health status among others are found to be associated with the prevalence of anaemia [8, 9, 11]. This study therefore investigated the factors associated with anaemia in pregnancy among women within the reproductive age group (15-49 years) in the Bolgatanga municipality of the Upper East Region of Ghana.
2. Materials and Methods
2.1. Study Area
- The study was carried out in the Bolgatanga municipality. The Bolgatanga municipality is the regional capital of the Upper East region of Ghana with a total population of 66,685 (2010 census).
2.2. Data and Source
- The study employed secondary data, obtained from the 2012/2013 registers of the antenatal clinic of the Upper East Regional Hospital in the Bolgatanga municipality, where routine records of all pregnant women (subjects) who report at the facility for maternal care services are taken. The study made use of variables such as Maternal age group, Parity, Gravidity, Blood Pressure (normal or abnormal), Gestational age ( in weeks), Haemoglobin level, Sickle cell status (positive or negative) and Season of the year (dry or wet). The study consisted of 617 pregnant women within the reproductive age group (15-49 years).
2.3. Generalized Linear Model (GLM)
- The GLM is an extension of the traditional linear model. It differs from a linear model in the sense that it assumes that the response distribution is related to the linear predictor through a function called the link function. The GLM has a linear component
 and a monotonic differentiable function,
and a monotonic differentiable function,  , that links the expected response,
, that links the expected response,  , to the linear predictor
, to the linear predictor  :
: The response
The response  is assumed to have a distribution from the exponential family. In this study the normal distribution was used. The vector
is assumed to have a distribution from the exponential family. In this study the normal distribution was used. The vector  is called an offset variable.
is called an offset variable.  is the design matrix and
is the design matrix and  is a vector of unknown parameters.
is a vector of unknown parameters.2.4. Binary Logistic Regression
- The binary logistic regression model is used for modeling response variables that are binary or dichotomous in nature. For a binary response,
 , let
, let  be a vector of
be a vector of  regressors, and
regressors, and  be the probability,
be the probability,  . The logistic regression model is a linear model for the log odds, or logit that
. The logistic regression model is a linear model for the log odds, or logit that  , given the values in
, given the values in  . The model is given by;
. The model is given by; and gives the probability of the event of interest occurring.
and gives the probability of the event of interest occurring.2.5. Multinomial Logistic Regression
- The Multinomial Logistic Regression, models the probabilities of
 categories as
categories as  logits comparing each of the first
logits comparing each of the first  categories to the reference category. The logits for any pair of categories are calculated from the
categories to the reference category. The logits for any pair of categories are calculated from the  fitted ones. With
fitted ones. With  predictors,
predictors,  , for
, for  . The logit is given by
. The logit is given by Each coefficient,
Each coefficient,  , gives the effect on the log odds of a unit change in the predictor
, gives the effect on the log odds of a unit change in the predictor  that an observation belongs to category
that an observation belongs to category  versus category
versus category  . The probabilities are calculated as
. The probabilities are calculated as
3. Results and Discussion
- The results revealed that the minimum, maximum and the average Haemoglobin level of the 617 pregnant women were 6.1g/dl, 16.6g/dl and 10.8g/dl respectively. Out of the 617 pregnant women, 311 (50.4%) were anaemic (Haemoglobin < 11g/dl) and 306 (49.6%) were non-anaemic (Haemoglobin >11g/dl). This prevalence rate of 50.4% is consistent with [15] estimated prevalence rate of 40% to 60% in developing countries. However, the prevalence is considerably lower compared to 57.1% in the Sekyere West District of Ghana [8], 76.9% in South Eastern Nigeria [13] and 62.6% in Eastern Sudan [1]. This may be attributable to geographical variations that influence certain anaemic influencing factors and improvement in health policies with time. Also, 163 (26.4%) had mild anaemia (Haemoglobin between 10.0 to 10.9g/dl), 144 (23.3%) had moderate anaemia (Haemoglobin between 7.0 to 9.9g/dl) and 4 (0.6%) had severe anaemia (Haemoglobin less than 7g/dl). The results revealed that mild anaemia was common followed by moderate anaemia. This is consistent with findings in Africa and elsewhere in the world [16, 10, 4, 7]. A Chi-square test of association showed that the Blood Pressure and the Age Group were significantly associated with the subjects’ anaemic status as shown in Table 1. Also, the Chi-square test indicated that there was no association between the Sickle Cell Status and the Season of the year, with the subjects’ anaemic status at the 5% significance level.
|

|
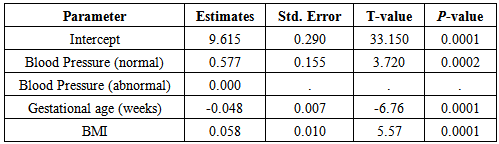
 Figure 1 is a diagnostic plot of the residuals of the reduce GLM. Clearly, the histogram of the residuals and the quantile plot indicates that the residuals are normally distributed. Also, the plot of the residuals and the predicted values revealed that the residuals are random. Thus the residuals of the reduced model are well behaved indicating that the model is adequate.
Figure 1 is a diagnostic plot of the residuals of the reduce GLM. Clearly, the histogram of the residuals and the quantile plot indicates that the residuals are normally distributed. Also, the plot of the residuals and the predicted values revealed that the residuals are random. Thus the residuals of the reduced model are well behaved indicating that the model is adequate.  | Figure 1. Diagnostic plots of residuals |
|

 A diagnostic test of the binary logistic regression model with the Hosmer and Lemeshow test gave a test statistic of 17.3742 with a P-value of 0.2064 indicating that the logistic regression model was adequate. Also, the Deviance and Pearson goodness-of-fit tests (Table 4) further affirmed that the model was correctly specified. The sensitivity test indicated that about 60 percent of the events of interest (anaemic) were correctly classified by the model while the specificity test indicated that about 66% of the non-event (non-anaemic) was correctly classified.
A diagnostic test of the binary logistic regression model with the Hosmer and Lemeshow test gave a test statistic of 17.3742 with a P-value of 0.2064 indicating that the logistic regression model was adequate. Also, the Deviance and Pearson goodness-of-fit tests (Table 4) further affirmed that the model was correctly specified. The sensitivity test indicated that about 60 percent of the events of interest (anaemic) were correctly classified by the model while the specificity test indicated that about 66% of the non-event (non-anaemic) was correctly classified.
|

|

|

4. Conclusions
- In this study, the determinants of Haemoglobin levels and anaemia status (anaemic or non-anaemic) of pregenant women (subjects) in the Bolgatanga municipality of the Upper East Region of Ghana were investigated. The results revealed that Blood pressure, Gestational age and BMI were useful in determining the Haemoglobin level and the anaemic status of the subjects. The study revealed that subjects with normal blood pressure and high BMI are less likely to be anaemic as their Haemoglobin is likely to be high. However, the studies revealed that as the Gestational age increases the subjects are likely to have low Haemoglobin levels which results in anaemia in pregnancy. It is therefore recommended that medical experts should advise the pregnant women to take in foods and or supplements that will increase their Haemoglobin level as the Gestational age increases and also engage in activities that will ensure that they have a normal blood pressure.