-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Psychology and Behavioral Sciences
p-ISSN: 2163-1948 e-ISSN: 2163-1956
2021; 11(1): 13-19
doi:10.5923/j.ijpbs.20211101.03
Received: Mar. 22, 2021; Accepted: Apr. 9, 2021; Published: Apr. 25, 2021

People’s Perception of Their Health Status Assessment and Notion of Illness in Rural Bangladesh
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLS. M. Raysul Haque1, Humayun Kabir2, Shifat Khan3, Shabareen Tisha1
1Dept. of Public Health, Independent University Bangladesh, Dhaka, Bangladesh
2Research and Development, Thinkthrough Consulting Pvt. Ltd, Dhaka, Bangladesh
3Infectious Disease Division, International Center for Diarrheal Disease Research, Bangladesh, Dhaka, Bangladesh
Correspondence to: Humayun Kabir, Research and Development, Thinkthrough Consulting Pvt. Ltd, Dhaka, Bangladesh.
| Email: |  |
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Bangladesh, a densely populated developing country experiences geographic maldistribution of human resources for health services. Moreover, poor health expenditure and lack of knowledge on comprehensive health measurements are another vital issues to have a suitable health assessment system yet. The contemporary single global question of self-rated health measurement requires certain educational qualification to understand the depth and dimension of that question-which often misleads the actual assessment of health. This study's aim was to explore rural peoples’ perceptions of their own health and disease with an attempt to add few relevant and comparative questions along with that single global subjective question to measure health in rural community. Without questioning the importance of objective measures to assess health we gave more emphasis on subjective measures considering our country’s socio-economic, educational and health service resources. This was an explorative qualitative study using in-depth interviews and focus group discussion which was then thematically analyzed. Data were collected from three different villages in a district of Bangladesh. Regarding defining the theme of health although the study participants have uttered the word mental or psychological satisfaction, for the vast majority, health means physical health and they also consider disease as an obvious part of life. To combat disease or for being healthy majority preferred to take medicines. About majority of the study participants have some ideas about health assessment. Most of them considered subjective measures should be used to assess health and disease as it is quick and inexpensive and the majority of them were not interested to visit doctors as they prescribed objective measures. Within the subjective measures, they prefer a collective approach of using a few questions which should be easy to understand as well as not too long or even not too short like a single question. After a detailed discussion with the collective approach reported bad health boosted 23% to 47%. On the other hand, reported good health declined from 77% to 53%. Considering gender females are more cautious about both for their own and families' health than males. The majority of the participants expressed their uncertainty of health condition for upcoming years and most of them rely on the creator’s will. To identify the most vulnerable people or people’s health perception needs to add few collective questions along with the global single question to understand the actual scenario in developing countries like Bangladesh. Within very minimum resources this quick and easy collective subjective health measure tool might easily be used on a large scale to identify the most vulnerable group in the community to provide further support.
Keywords: Self-reported health, Subjective health, Bangladesh
Cite this paper: S. M. Raysul Haque, Humayun Kabir, Shifat Khan, Shabareen Tisha, People’s Perception of Their Health Status Assessment and Notion of Illness in Rural Bangladesh, International Journal of Psychology and Behavioral Sciences, Vol. 11 No. 1, 2021, pp. 13-19. doi: 10.5923/j.ijpbs.20211101.03.
Article Outline
1. Introduction
- Quality of life depends on health and often it is believed that unawareness, illiteracy and poverty are responsible for ill health. Generally, Health is a direct measure of human well-being and is an achievement in itself. In a developed country, befalling chronic health condition may have lower effect on the quality of life on the patient than the same disease would have higher impact in a lower income country because of scarcity of resources [1]. According to WHO “an individual’s perception of his/her position in life in the context of the culture and value systems in which he/she lives, and in relation to his/her goals, expectations, standards and concerns”. Senses regarding life experience are subjective and individual perceptions regarding factors influencing the consideration for wellbeing may differ from another’s perception [1]. Persons create of their health situation and regular life understanding that is self-perceived health status. Self-perceived health is a process and information about health and disease, prior involvement and the social, cultural and historical settings are required for this process [2]. To improve health and measure individuals need, understanding the people’s perception about their health is important. Knowledge about people’s perception regarding their own health is essential to promote healthy behavior [3]. Self-perception of own health is considered to be a powerful predictor of mortality [4-6]. Living conditions and nutritional status boosted the occurrence of illnesses in poor people. They cannot earn during illness. On the other hand, they have to spend a considerable amount of money for treatment. As they were not earning moreover sending for treatment either from borrowing or selling household products which leads to long-term poverty to them [7]. There are some factors involve with treatment choices, these are illness type and severity, existing belief, availability and accessibility of healing options, convenience, costs, quality of service, staff attitudes as well as the age, gender and social circumstances of the sick individual [8-9].In many developing countries, the existence of several healing systems in a single cultural setting is an important feature of health care. Poverty and gender determine both illness incidence and treatment options, ranging from self-care to folk and western medicine [10]. The easy accessibility of medicines plays an important role in medicine consumption with one’s perceived health conditions and symptoms [11-12]. Lack of medical facilities and the free accessibility of drug stores and poor national drug regulatory policy are the reason of self-medication [13] and practicing self-medication can lead to various health hazards. Like many other developing country Bangladesh experiences geographic mal-distribution of Human Resources for Health. Health expenditure is only 2.8% of GDP and there is very limited information on population health for complete measures [14]. Over the last few years Bangladesh has achieved considerable success in health and population sectors but there are also significant challenges in the areas of system losses, access and quality of services [15]. In rural areas people suffers from the availability and accessibility to proper health systems [16]. In order to plan the improvement of a country’s health system the health status information of entire nation is needed. Moreover, it cannot afford to measure population health through standard objective health measurement tools. To identify the vulnerable group in the society, the only alternative tool is the subjective health measurement tool. The subjective health measurement can measure very basic general health status without any objective measurement. Though Self rated health measurement is a subjective status, World Health Organization (WHO) approves it for routine use in population studies as it is versatile [17]. This self-perception of health can help us to investigate the other indicators of health that can be collected from large numbers of individuals with least expenditure and resources [17].Objective measurement of health requires consultation fees, pathological tests, time and other logistic support [9]. On the other hand, simple self-rated health assessment is fairly easy and inexpensive to execute [17]. In population studies self-rated health can be routinely used to recognize a person of higher risk with poor health consequences which is approved by World Health Organization [18]. There are two conventional ways of subjective measurement of health, such as multiple questions tool and a single question tool. The first question of the Short form 36 Health Survey Questionnaire “What is your current health status- very good, good, moderate, bad or very bad?” [1] is widely using as a global question to assess the general health status in developed countries. Both of these tools are either too lengthy or too short and directly linked with educational status of the participants [19-20]. Usually people with higher educational qualification respond well with these tools compare to lower educational status. Developing country like Bangladesh is no exception and majority lives in villages and have relatively low educational qualification compared with urban people. Considering this country context, this study aimed to understand rural people’s perception of assessing their own health status. Majority of the similar study was follow the quantitative methods. To find out the suitable subjective tool along with the global single question for health measurement with minimum resources this study followed the qualitative methods. Considering all these evidences, this qualitative study focuses on to gain an in-depth understanding of people’s perception of their health, disease and health status assessment with a combined approach of few culture sensitive subjective questions.
2. Methodology
- This study was qualitative in nature and collected data from primary source and contently analyzed. There were two different qualitative tools used for this study - In-Depth Interview (IDI) and Focus Group Discussion (FGD). IDI open the scope of informal discussion or conversation that helps to grasp the whole scenario of responses. On the other hand, FGD gives us the platform to have more structured conversation involving a group of people from where we can get a comprehensive picture on a particular issue. A guideline was developed to follow the process with important probing during interview and discussion. FGD were chosen to understand one’s perception in front of his/her peer, may not be his opinion while s/he asked individually especially regarding medicine buying and selling without prescription etc. The interview tools were developed based on literature review, expert opinions and the Short Form 36 Health Survey Questionnaire [18]. Using different tools permitted the triangulation of findings and enriched the data interpretation (figure 1).
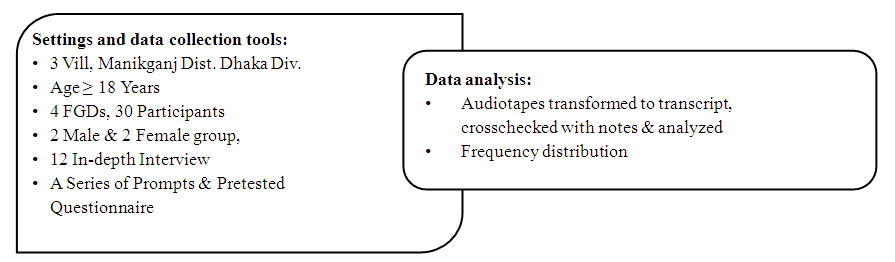 | Figure 1. Settings, data collection tools and data analysis |
2.1. Site Information
- For the site selection this study utilized the platform of LFE (Live in Field Experience) of Independent University Bangladesh (IUB) through which IUB has been maintaining a Health and Socio-Demographic surveillance for years. Currently IUB has eight different sites. All the sites had been selected purposively based on the availability of local collaborative institute or NGOs and then three villages were randomly selected in each site. Within the villages 100 household were randomly selected and by this way 300 household were selected and followed in each site. Our study area Saturia, an Upazila of Manikganj district, is one of the eight sites of LFE platform. This study used to collect data during June 2017 with prior approval and consent of university authority.
2.2. Participants’ Characteristics
- Participants with good and bad health were purposively selected from the low socioeconomic or needy; from relatively solvent and the high socioeconomic or the leading group of the society. There was question “what is your current health status?” in the LFE Socio-demographic surveillance. Based on the response of this subjective question respondents were treated as good and bad health groups. These health statuses were self-reported by the global question approved by WHO, “What is your current health Status?” from the selected villages participants of 19–60 years old were included. Four FGD and eight IDI were included in the study: FGDs were conducted in two villages with both good and bad health male and female participants to understand their perception. In-depth interviews were conducted in the selected villages with medicine sellers, rural doctors and good and bad health status participants.Population and geographic characteristics were homogenous among all selected villages. The number of respondents in the discussion groups ranged from 6 to 9. Total 12 in-depth interview was conducted with different types of participants like medicine seller, rural doctor, male and female with good and bad reported health, rural health assistant etc. And 6 FGD were conducted with different types of group like male and female needy group and solvent group with reported good and bad health separately.
2.3. Process
- The focus group discussions (FGD) with the participants were conducted at school, mosque and at a local NGO premises. A team with one facilitator, one note-taker and one organizer, were deployed to conduct the FGDs. After welcoming participants in each session during FGD, the facilitator gradually introduced a series of prompts to explore the desired information. A guideline was used for the in-depth interviews. Open ended questions were used for FGD and IDI i.e. what your current health status is, how would you assess your current health status etc. Before the interview or discussion, the aims of the study were explained to the participants, confidentiality guaranteed, and permission asked to record the interview, thus obtained informed verbal recorded consent.Facilitators conducted the interviews and the focus group discussions in the preferred language of the participants. All interviews were recorded and transcribed with expanding the detail hand notes.
2.4. Analysis
- Data analysis process followed the manual qualitative data analysis. We called this ‘manual content analysis’ where the contents were first identified from the guideline and prompts, then cross checked were done with the findings and themes were identified. Finally, investigator interpreted the themes and facilitators’ feedbacks were taken on regular basis. (table 1)
|

3. Results
3.1. Health and Disease Perception
- All the participants were asked about their current health status and most of them stated that it was good. Generally, the common people of Bangladesh at their first appearance always offer such statement. But during the conversation it gradually reveals the real situation. After probing they mentioned that their health condition was not so good at present. The reasons behind their bad health condition were hot weather, food adulteration, lack of money to avail proper nutrition and medicine, below quality of medicine and new diseases with existing ones. A bad health status woman with high blood pressure and headache said that she would be better if she took medicine, but she could not tolerate the odor of medicine. One group discussion participants were mostly working in a local NGO and a recent strike create a critical situation for them. This incidence triggers them to high blood pressure due to tension, lack of sleep and appetite. They also suffer from fever, gastric, headache and gastric problems. The job insecurity and the worry about future lead them mentally ill and suffering from various diseases. One male participant from focus group discussion stated that,“Due to our job stress my (blood) pressure is fluctuating for 10 to 12 days and it is 100/140 or 90/150. This is happening for tension. Moreover, it is too hot, and we are moving here and there for escaping the police harassment, many employees are living in the same place and all these are the reason for bad health condition.” In order to get rid of this stressful situation a part of male participants was taking medicine for controlling blood pressure and for good sleep. The focus group participants believed that, consumption of medicine gave them both physical and psychological support. An in-depth interview with a bad health status woman whose daughter had just passed away said, “I have internal pain due to my daughter’s lose. Medicine cannot cure it.”Her daughter was the main earning member of the family. She did not know about her upcoming days. As a concept or theme of health majority conclude that health means just free from physical diseases with very few added mental diseases or psychological issue as well. On the other hand, as a concept of disease all most all participant opined that they do not know much about health, but they understand disease very well because they only realize the important of being healthy when they become sick. The female focus group participants assumed medicine as to protect them from illness and it also had a divine power in it. One female participant stated that,“Diseases are common, everybody suffers from diseases, we cannot survive without medicine and none is completely disease free. We need to take medicine for better health.”
3.2. Health Perceptions in Gender Perspective
- Considering the sex difference in understanding the “Health and Disease” we found that females are more concern about their own health status as well as the health of their entire family in comparison to their counterpart, but usually they had least access to avail any health facilities. One of the female FGD participants said,“For the betterment of our own family we the female members are more careful for our own health as well as the health of our children and husband.”On the other hand, the males are relatively reluctant about their own health status, to them health means free from major disease as minor issues do not need any such interventions. One of the male FGD participants said,“I am the main earning person of my family. I do not have enough time to care about my health. I only care when a major illness happens and due to that I cannot go out for earning.”Females are usually more likely to take medicines and continue until the health problems apparently resolves, on the other hand males are usually take first few doses of medicine and in majority cases they discontinued the medicines upon getting primary relief.
3.3. Assessment of Health
- How do the local people assess their health status? Answer varied from person to person depending on their cultural belief, age, education and social class. The current study tried to reveal answer to some general question pointing to preference of subjective or objective measurements of health and a detail feedback on subjective health measurement. Considering the existing knowledge about health assessment or screening among 30 FGD participants 20 participants (67%) had some idea about it while four participants (13%) had no idea and six (20%) had relatively good idea on it.Majority of the participants were not in favor of objective health measurements as it involves both cost and time. They were okay with measuring blood pressure or temperature but not with different pathological test like blood, urine, stool test and X-ray or Ultrasonogram. Their view was these things should only be done when a person is seriously ill or for a very complex disease where a patient is going to die and not well responded with treatment. These objective measurements should not be practiced for normal health problems. One male participant said,“Majority MBBS and senior doctors’ advice lots of tests and in most cases, they were normal or fail to detect their problem or even the doctors were not looking the reports properly with attention. It is wastage of our valuable money which we can spend on medicine purchase.” The participants who were from solvent group of the society they opined that objective measurement of health should also be performed in selective manner along with subjective measurement. In general, where majority went for only subjective measurement where a doctor will provide adequate time to a patient to hear his/her problem and prescribe medicine accordingly. Only two out of thirty participants (7%) were in favor of objective measurements, four (13%) were in favour of both objective and subjective assessments and rest (80%) were only in favour of subjective health assessment.
|
3.4. Health Assessment Compared to Others
- Participants were asked to compare their current health status with others of their own age in the village; they stated that others of their own age were in good health. In one group discussion the reason mentioned was stressful lifestyle and in another group discussion it was poverty as it required money to buy medicine. Only two good health status female FGD participants said they feel better than others of their own age. One female participant said,“My health condition is good, but it does not mean best. Sometimes I feel sick. I used to go to the medicine shop besides my house and purchase medicine. I feel better when I take medicine.” A female FGD participant said, “We are more unwell than the elders as they did not intake foods with fertilizer but now, we take all with fertilizer whether it is milk, fish or meat. Now a day’s cow needs to feed artificial vitamins and medicines for milk, same for fish and chickens. The elders took fresh foods; my grand-mother-in-law can work more than the women of our aged.”
3.5. Health Assessment Compared to Time
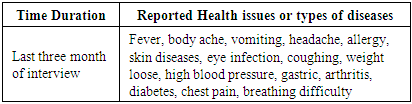
- The participants were asked about their current health status compared to the same time of last year. About half (14/30) of the FGD participants said they were in good health situation during this time of last year. Now they were not in such good health status. An older female participant of FGD said,“One year ago, I was better than now. I had breathing difficulty and it is worse now. If I take medicine, I feel good otherwise my situation deteriorates.” About 27 out of 30 FGD participants reported the following health issues for the last three months (table 3).
|
3.6. Anticipation of Health in Upcoming Years
- In all focus group discussion participants expressed their uncertainty of health condition for upcoming years. They said “It would be either good or bad.” Although 67% of the participants were optimistic for the good health in future but most of the cases people share the view that future health condition/ status completely depends on the creator’s will. The cultural and spiritual believes often dictates their health perception considering future projection.
4. Discussion
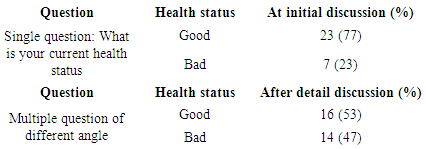
- This qualitative study investigates the rural Bangladeshi people’s perception of assessing their own health status and medicine consumptions as a proxy of seeking health care. After asking all the participants with single conventional question “What is your current health status?” most of the respondents answered they were “good”. But after probing actual scenario exposed and reveal that most of them were not good in their present situation. By asking global questions about current status majority of the participants reported “good” health but real situation was revealed by additive few questions denoting peer/person comparison, time comparison and predictive for future health status. After probing with combine questions, 77% of reported “good” health gone down to 53%. On the other hand, 23% of reported “bad” health rose to 47% with those combined approach in comparison to that single global question [14].Some study shows that self-rated health may differ in developing countries with developed countries because of differences in levels of economic development and disease patterns [17,21-22]. Respondents described the reason behind the “bad” health is poverty as some studies documented that educated and rich people has reported better health than uneducated and poor. The finding is also similar with mortality patterns that educated and rich people had lower mortality than uneducated and poor [23]. Similarly, improvement of economic status can pick up the ability to purchase better health care service and also can provide better nutrition and housing [24]. Most of the FGD participants practiced self-medication and consider it is good for health and psychological support. Some studies showed that the choice of medicine depends on individual’s psychological condition which is not unintentional or coincidental especially for the choice of particular drug [25]. To get relief from specific condition individual choice their drugs. Most of the study participants like to rely on subjective health measures and opined that objective health measures should only be done in severe illness. According to most of the SRH studies subjective health capture the full range of illness and possibly even symptom of disease yet undiagnosed at present or even in preclinical stage [20]. These study findings support that an individual can efficiently evaluate their own health in locations where communication with professional health caregivers is low [26-27]. Regarding health seeking behavior findings of this study shows that seeking treatment from informal health professional, village doctor or traditional healer were more frequent form of managing health along with self-care which is also found in some other studies. In comparison of gender, women are more concern about their health. Other study showed that range of reporting poor/ very poor health and good/ very good health is higher among women than men [28]. But another study revealed that men are more likely to seek health care than women probably due to powerful patriarchy practice and socio-economic status [10]. In Bangladesh aged people do not get enough treatment from the formal health service providers and most of them depend on informal or traditional health providers [29]. In comparison of time most of the participants reported “bad” health. Similar findings we found in different studies that most of the elderly people reported very poor health compares to previous age cohort [30]. All of the participants expressed the uncertainty about their health in upcoming years and they only rely on God. Religious belief may decrease fear and provide relieve when people are in stress. Possibly, the nervous system symbolizes the locus of a mechanism by which religious faith or beliefs support well-being. Another study shows those who are involve in higher level of religious activity mean more expected years lived [31].This study also has weakness like majority of the studies. This self-perception of health may not always exactly capture the specific health problems and rely on subjective health assessment may not always showed the similar diagnosis in comparison with objective health evaluation. Considering few of the shortcomings like culture sensitive, reliant on educational status and subjective in nature this can be used in large scale with very minimum resources to easily identify the most vulnerable group in the community. Later these identified groups can be assessed objectively and then treated accordingly. So from our country perspective considering its nature and execution few of its weakness may easily be compromised. Further research is necessary including a large scale quantitative and other tools of qualitative research as this study could not capture all the variables which have high effects on people’s perceptions of health.
5. Conclusions
- Adding few questions with the global single question will be a suitable subjective tool to understand the rural people’s perceptions about their own health status of developing countries like Bangladesh. To identify the most vulnerable group in the community and to provide further essential health services, a collective approach of few subjective questions might easily be used in large scale specially in developing countries. This subjective tactic is simple, comparative, not too long or too short as single question and easy to execute. A further large scale quantitative research is needed to make it more generalizable, valid and reliable.
ACKNOWLEDGEMENTS
- We are obliged to all the respondents for giving time and valuable information. We are grateful to the authority, Independent University Bangladesh for giving permission to use the platform of “Live in Field Experience (LFE)” courses. We are indeed thankful to Late Dr. Mahbub Alam, Dean of School of Liberal Arts and Social Sciences (SLASS) for inspiring and guiding us to commence this study.