-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Psychology and Behavioral Sciences
p-ISSN: 2163-1948 e-ISSN: 2163-1956
2021; 11(1): 1-5
doi:10.5923/j.ijpbs.20211101.01
Received: Jan. 21, 2021; Accepted: Feb. 12, 2021; Published: Feb. 26, 2021

Quality of Life in a Sample of Women in Puerto Rico Diagnosed with Breast Cancer: A Comparison Between Two Groups
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLEstefanía Texidor Vega1, José Rodríguez-Gómez1, 2
1Carlos Albizu University, San Juan Campus, San Juan PR
2University of Puerto Rico, Medical Sciences Campus, San Juan PR
Correspondence to: Estefanía Texidor Vega, Carlos Albizu University, San Juan Campus, San Juan PR.
| Email: |  |
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Introduction: According to the American Cancer Society, breast cancer is the most prevalent type of cancer reported in women in Puerto Rico. It is a phenomenon that impacts the lives of women and their families, In addition, cancer treatment can be serious stressors. Method: The present investigation sought to evaluate the health-related quality of life in a group of women diagnosed with breast cancer. We pretend to explore whether there are differences in patients who have not obtained a cancer diagnosis and those who have. Also, it was intended to establish relationships between the scale that measures quality of life in patients diagnosed with cancer in Puerto Rico (SMQLPWC-PR). Purpose: Although death rates have been declining over time, the death rates of women with breast cancer in PR remain high. Recognizing this phenomenon and understanding the impact it has on lives of these women and their families, we would like to help woman with cancer to reduce their suffering; in addition to educate patients to manage the disease. The study consisted of a group of participants with cancer (n = 27) and a control comparison group (n = 61). The group of cancer patients completed the scale that measures the Quality of Life of cancer patients in Puerto Rico (SMQLPW-PR) and the comparison group completed the SF36 scale (Short Form Health Survey in Spanish) that measures Health Quality of Life and the Personal Spirituality Scale. Results and conclusions: Social support was observed as a construct that affects how women with cancer in Puerto Rico feel. Moreover, physical exercise and the religious element seem to contribute positively to the quality of life in those women. We conclude that the three previously mentioned elements should be promoted in these patients to enhance their quality of life.
Keywords: Breast Cancer, Spirituality, Quality of Life related to health, Puerto Rico, Public health
Cite this paper: Estefanía Texidor Vega, José Rodríguez-Gómez, Quality of Life in a Sample of Women in Puerto Rico Diagnosed with Breast Cancer: A Comparison Between Two Groups, International Journal of Psychology and Behavioral Sciences, Vol. 11 No. 1, 2021, pp. 1-5. doi: 10.5923/j.ijpbs.20211101.01.
1. Introduction
- Cancer is known in Puerto Rico as the leading cause of death according to the 2016 Health report, with 52% the figure for women and 48% for men [1]. Breast cancer is recognized worldwide as one of the highest cancer incidences in women. In Puerto Rico, it is reported as having the highest incidence and mortality and the main type of cancer in women according to the American Cancer Society. For the years 2008-2012, 29.6% of women out of a population of 33,247 women are diagnosed with breast cancer [2-5]. Currently, the prevalence of breast cancer in Puerto Rico is followed by colon and rectal cancer, and thyroid [6]. It is considered a phenomenon that impacts the lives of women and their families and the cancer treatment process can be one of many stressors. Although death rates have been declining over time, the death rates of women with breast cancer on the island remain relatively high. Recognizing this phenomenon and understanding the impact it has on the lives of these women and their families helps us reduce suffering and educate people susceptible to developing the disease. Quality of life as a concept related to health is important to lead a healthy life that is worth living. It is pertinent to take into consideration when a person is diagnosed with this disease, since despite being a lethal disease, technological advances have somewhat corrected the obstacles that accompany the disease and the patient is more likely to experience a remission [7]. The aim of the study was to evaluate quality of life of women with breast cancer in the island and to evaluate differences with control group in regards to psychological, physical, spiritual and social aspects.
2. Methods
- The present investigation pretends to evaluate the health-related quality of life in a group of women diagnosed with breast cancer in order to analyze whether there are differences in relation to patients who have not obtained a cancer diagnosis. Also, it was intended to establish relationships between the dimensions of the scale that measures quality of life in patients diagnosed with cancer in Puerto Rico (SMQLPWC-PR). Although death rates have been declining over time, the death rates of women with breast cancer on the island remain relatively high. Recognizing this phenomenon and understanding the impact it has on the lives of these women and their families helps us reduce suffering and educate people susceptible to developing the disease. Group criteria for cancer group were to be older than 21 years old, express consent to participate in the study and must have lived a minimum of 5 years in Puerto Rico. For the control group, group criteria consisted in being older than 21 years old, express consent to participate and not having or having had a diagnosis of breast cancer or another type of cancer in the last 5 years. The study was made up of a group of participants with cancer (n = 27) and a control comparison group (n = 61). Measures:The group of cancer patients completed the scale that measures the Quality of Life of cancer patients (SMQLPWC). The scale was developed and validated in Puerto Rico by Dra. Janelly Muriel Sanoguet [8]. The scale is a Likert-type questionnaire with a total of 190 items that is divided into four categories (Spirituality, social support, psychological aspect and physiological aspect) and has a series of 17 categorical questions that measure specific symptoms. The Likert scale goes from 0 indicating “never” to 3 indicating “a lot”. The administration time of such a scale is from half to an hour. The scale obtained a final Cronbach's alpha index of 0.927 and in the validation study they describe it as “excellent reliability” [5]. The comparison group completed the SF36 scale (Short Form Health Survey in Spanish) that measures Health Quality of Life and the Personal Spirituality Scale [9-11].The SF36 is a questionnaire used to measure Health Related Quality of life and has the ability to compare between participants. SF-36 measures physical, mental, social and emotional aspects. The administration time of this scale is 5-10 minutes, it can be administered to anyone over 14 years of age and the answers to the questions are based on a self-report. This is based on 36 questions and has 8 subscales. These 8 scales measure: perception of health in general, physical appearance, physical role, emotional aspect and emotional role, social functioning, body pain and mental health. Scores on the scale range from 0-100, high scores indicating better quality of life status and are answered on the basis of a Likert scale. Studies indicate that the SF-36 RAND scale contains good internal consistency between 0.68-0.93 and good construct validity [12-14]. On the other hand, the translation of the scale into Spanish responds to having an equivalence to the original instrument and an acceptable internal consistency, between 0.71-0.94 [15].The Personal Spirituality Scale was developed and validated in Puerto Rico by González Rivera, Veray-Alicea y Rosario-Rodríguez (2017) to study spiritual dimension. The same is based in the Model of Multidimensional Spiritual Connection (MMCE) de González-Rivera (2017). This is a Likert-type questionnaire (1-4; fluctuating between totally disagree to totally agree) that consists of 12 items distributed in three subscales. Scores range from 12 to 48 and it is understood that the higher the score, the more spiritual. The answer itself takes about 5 minutes. It measures three domains: intrapersonal connection, interpersonal connection, and transpersonal connection.
3. Results
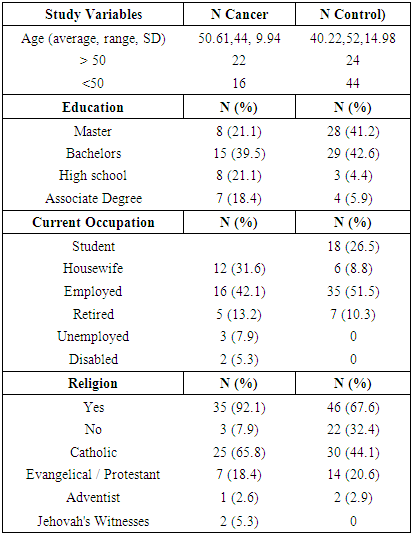
- The study sample consisted of 88 participants who completed the scales. All analyzes were performed with the SPSS-X version 21 program. Regarding the participants who answered the scales, the groups are divided between the group of participants with cancer (n = 27) and a comparison control group (n = 61). In relation to the comparison group, the majority of the women are Puerto Rican, single, with an average level of high school and middle-class education. Most of the women did physical exercise and practiced the Catholic religion (44%); 21% of these are Evangelical / Protestant, and 2.9% are Adventist. As for the group of women diagnosed with cancer; the majority of the study sample are married, have undergraduate and postgraduate studies, their occupation is housewives or employees, and they reported being middle class. Most of these are Puerto Rican and American living in Puerto Rico. The majority reported that they do not exercise, being 66% and 92.1% practicing some religion, with the largest group being Catholic (65.8%) followed by evangelical / Protestant 18.4% (See table 1).
|
|
|
|
4. Discussion
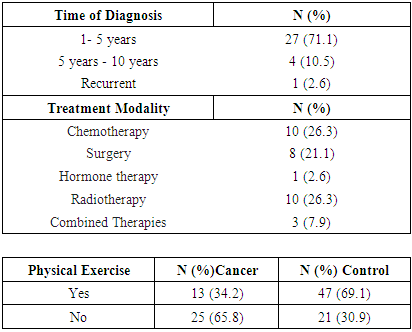
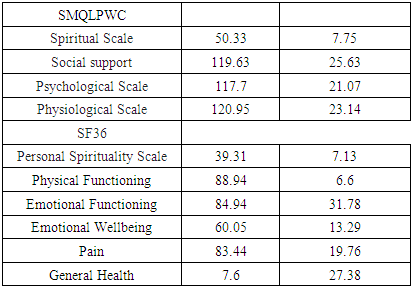
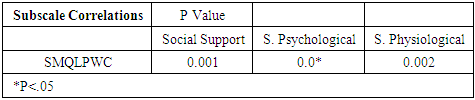
- The purpose of this study was to know the Health Quality of life of women diagnosed with breast cancer in Puerto Rico and those areas of need according to the dimensions of the Quality of Life Scale. Likewise, they wanted to know the quality of life in general of this sample of women in Puerto Rico. For this, three questions were established with their respective hypotheses. The data found in the study is consistent with what has been demonstrated in the reviewed and cited literature, and suggest that Social Support may play a role in maintaining the quality of life of cancer patients and people in general.Quality of Life of both groups: According to the results obtained when performing analysis on the total Quality of Life scores in both groups, variable scores were observed. Despite the differences in the size of the sample and the questionnaires performed, the majority of the participants in both groups scored between good, adequate and excellent. As for the comparison group, lower scores were observed in the emotional domain, which was shown to be the area of greatest need. Even though the quality of life scores are different and the group is smaller, it was observed that many women diagnosed with cancer reported low scores in Quality of Life (see Table 3). This is consistent with studies that reported that women who experience health problems, such as cancer, have a decline in quality of life related to many domains of their life, even when they were diagnosed many years ago [16]. However, these scores were not as negative compared to the control group. This suggests that other variables could be related to the maintenance of Health-Related Quality of life in these women. Regarding the descriptive aspects, it was observed that in comparison with the control group, the patients with the diagnosis of cancer reported reduction in physical exercise, or that they did not perform it, being 59% (n = 27) of the sample. According to Trentham-Dietz, et al (2008), cancer patients report a reduction in the domains of health and physical activity and they remain, even after 10 years of cancer diagnosis, with the same reduction. However, the scores on the physiological scale remained between good and excellent.The treatment received demonstrated a significant impact on quality of life. Therefore, it could have an impact on the quality of life of patients. This could be related to the side effects of some therapies which can have an impact on the person's ability to adjust to the cancer condition. It would require exploring this area more specifically. Regarding social support, we could observe that the participants use social support as a method to face / mitigate the disease. It was observed as the best predictor of quality of life, it was perceived social support. Regarding what is evidenced in the reviewed literature, factors such as optimism, personal efficacy, and social support have been shown as protective factors in cancer patients [17].Correlations between quality of life and subscales: Statistically significant scores were obtained between the Quality of Life Scale for Cancer patients (SMQLPWC) and the variables: Social Support (r=0.605, p=0.001) Psychological Scale (r=0.797, p <.00) and Physiological Scale (r=0.641, p=0.002). The spiritual aspect was not a significant variable, however, the majority of the participants (92% (n=27) of the cancer group indicated belonging to some religion, which confirms its impact on the well-being of these participants since they showed high scores on the spiritual side. The results highlight that within the sets of factors and conditions that an individual must have in order to enjoy a good quality of life, the perception of feeling loved and having support, as well as feeling well physically and emotionally, are very important factors. This also confirms the multidimensionality of the concept of Health Quality of Life which encompasses physical, social, psychological and spiritual well-being according to the biopsychosocial-spiritual theory [18].Culture, Spirituality and Religion: Research findings on the impact of breast cancer on women highlight the emotional impact after the disease, such as low self-esteem, guilt, a sense of loss of femininity, and frequent symptoms such as pain, and financial problems. However, spirituality can function as a double version: women can accept illness as something that God put on their path and something that can be overcome, but also as anger or punishment [19]. They even highlight that life factors tend to be cultural, which is why it is known that lower-income women hold on to God to achieve healing (Cordero, et al., 2020), however, there are other methods such as use of humor, among other techniques, for management and even personal healing that are accepted and used in other cultures, such as American culture. Regarding the data found in this study, Puerto Rican women diagnosed with cancer were described as strongly influenced by spiritual and religious beliefs. Although the relationship was not significant, it proved to be positive, so the higher the level of spiritual beliefs and the better quality of life. Consequently, the majority of the participants indicated that they were part of a religion and reported a considerable and strong relationship to turning to religion or spiritual beliefs in cancer care.Study limitations:The research has its methodological limitations that must be taken into consideration in future research. One of the limitations was the size of the sample used due to the difficulties imposed during the COVID-19 pandemic where the collection of the sample was limited. Another limitation was the place where the sample was collected, since it was collected mostly in social media forums, which makes it impossible for other people to participate due to access to these places. Also, the collection of the results in two different tests and the small sample made it impossible to carry out more complex statistical tests, which could impact the precision of the data. Another reason was the use of the SF36 scale, Spanish version due to the difficulty of knowing Cronbach's alpha. Finally, the cooperation of the participants to answer all the questions impacted the veracity of the scores for the element of social desirability when answering multiple questions. This highlights the impact of collecting information in person with patients, something that can maximize the efficiency of the investigation.
5. Conclusions
- In general, social support is a multi-complex construct that affects how women with cancer feel, helping them to move forward. In the same way, physical exercise and the religious element seem to contribute to their quality of life in favorable terms. We suggest further investigation with different types of samples to reaffirm and corroborate these findings in other samples / populations.
6. Recommendations
- Based on the findings the current research; we suggest further investigation with different types of samples to reaffirm and corroborate these findings in other samples / populations.