-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Psychology and Behavioral Sciences
p-ISSN: 2163-1948 e-ISSN: 2163-1956
2018; 8(1): 7-11
doi:10.5923/j.ijpbs.20180801.02

Ranking the Desirability Indicators of Community-Based Rehabilitation (CBR) Based on Analytical Hierarchy Process
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMehran Emami Eskandar1, Mahmood Otadi2, Toraj Mojibi1
1Faculty of Management, Islamic Azad University, Firoozkooh Branch, Firoozkooh, Iran
2Faculty of Mathematics, Islamic Azad University, Firoozkooh Branch, Firoozkooh, Iran
Correspondence to: Mehran Emami Eskandar, Faculty of Management, Islamic Azad University, Firoozkooh Branch, Firoozkooh, Iran.
| Email: |  |
Copyright © 2018 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Community-based rehabilitation is a strategy for promoting the quality of life of disabled people and protecting their rights through accessing services provided and creating equal opportunities. The present study aims at ranking the desirability indicators of community-based rehabilitation based on the analytical hierarchy process. This is an analytical study. The statistical sample comprised all experts including the director generals of Welfare Organizations, rehabilitation deputies, the chief of rehabilitation departments, rehabilitation assistants, and experts in charge of community-based rehabilitation in Tehran Province. Standard questionnaires were used to elicit data for the analytical hierarchy process which makes a pairwise comparison between primary and secondary indicators in the rehabilitation matrix. The group analytical hierarchy process technique in the Expert Choice 2000 software package was used to calculate the analytical hierarchy process in the present study. Based on the three-round Delphi among the experts, education had the highest rank among other indicators, the effect of which was 37% and empowerment ranked the last with a 7% effect. Based on the results of the present study, all the elements of community-based rehabilitation matrix points towards empowering a disabled person and enjoying their rights in every respect, whether in a family or local community.
Keywords: Community-based rehabilitation, Desirability indicators, Analytical hierarchy
Cite this paper: Mehran Emami Eskandar, Mahmood Otadi, Toraj Mojibi, Ranking the Desirability Indicators of Community-Based Rehabilitation (CBR) Based on Analytical Hierarchy Process, International Journal of Psychology and Behavioral Sciences, Vol. 8 No. 1, 2018, pp. 7-11. doi: 10.5923/j.ijpbs.20180801.02.
1. Introduction
- Disability causes significant damage to affected individuals, their families and on a broader scale, the society in economic, social and emotional terms [1]. It is obvious that existing medical and rehabilitation services are not sufficient to meet the needs of millions of handicap people [2]. Although developed countries have been able to provide some of the needs of handicap people in the field of medicine and rehabilitation (based on their claims), providing adequate opportunities for employment, joining social life, enjoying identical citizenship rights and removing negative attitudes towards disability, are issues that are still encountered by the handicap people in these countries [3].Rehabilitation is currently a philosophy that should not turn into an intellectual foundation of health service delivery, and it is neither merely one stage of the stages of health service delivery, but the preservation of the competencies and potential roles of individuals [4]. Although rehabilitation, like other current scientific subjects, has undergone extensive developments such that its concepts have changed, what is certain is the fact that there are three approaches in the implementation of rehabilitation: center-based rehabilitation, institution-based rehabilitation and community-based rehabilitation [5].Einar Helander, Chief Officer at WHO's Headquarters in Geneva in 1975 introduced community-based rehabilitation for the first time. He defined community-based rehabilitation as: a strategy for promoting the life quality of people with disabilities through accessing services provided, creating equal opportunities and preserving the human rights of handicap people [6]. In community-based rehabilitation, the work axis is the local community such that the start point is exactly the opposite. The disabled person, family members and local community decide on their priorities and then work with each other to access appropriate and existing services along with local rehabilitators, governmental and non-governmental groups [7, 8].The analytical hierarchy process was first proposed in the 1970s. Similar to the human brain, this method analyzes issues. This method enables decision-makers to determine the simultaneous and mutual effects of many complex and uncertain situations [9]. Data analysis is a multi-stage process whereby the data collected through the use of collection tools in a statistical sample (population) are summarized, classified and finally processed to lay the groundwork for conducting analyses and relationships between data in order to test the hypotheses. Such process assists decision-makers in "ranking based on their purposes and knowledge and experience", so as to consider their feelings and judgments. It is necessary to explain the problem in details and depict the "hierarchical structure" to solve decision-making problems through this technique [10]. Thomas Saati (founder of this technique) stated the following as the principles of the analytical hierarchy process and based all calculations, laws and regulations on these principles. These principles are: reverse condition, homogeneity, dependency, expectations [11].Considering that in every society, disability is one of the fundamental concerns of governments, their empowerment reduces the costs incurred by the government and will have a significant effect on the development of that society. The present research was informed by the felt gap in the optimal use of community-based rehabilitation, lack of financial resources and lack of optimal allocation of available funds in the Welfare Organization of Tehran Province. In order to prevent the waste of resources and identify the main needs of disabled persons in the target population, the present research was also conducted to ensure the optimal and purposeful use of existing funds. The purpose of the present study was to "rank the desirability indicators of community-based rehabilitation based on analytical hierarchy".
2. Materials and Methods
- This is an analytical study. In the present research, the statistical sample comprised all experts including the director generals of Welfare Organizations and rehabilitation deputies in Iran, the chief of the rehabilitation department, rehabilitation assistants, and experts in charge of community-based rehabilitation in the Tehran Province. The sample size of the study was 20 consisting of 2 director generals of the Welfare Organization, 2 rehabilitation deputies, 2 members of the rehabilitation department, 1 rehabilitation assistant, 12 rehabilitation experts and 1 professor of medical sciences in Iran.A standard questionnaire was used to elicit data for the analytical hierarchy process. The panel of experts was asked to determine the significance of the indicators derived from the research literature based on verbal variables ranked thus: very low, low, lower than medium, medium, more than medium, high and very high.The analytical hierarchy process is used to decide and select an option from a variety of decision options, considering the indicators determined by the decision-maker. The basis of this decision-making technique lies in latent pairwise comparisons. This approach starts with providing a decision tree which indicates the compared factors, and competing choices evaluated in the decision. Then a pairwise comparison is made, the results of which determines the weight of each of the factors in line with the competing options. Eventually, this logic integrates matrices from pairwise comparisons to make an optimal decision [12]. The steps for implementing this technique are as follows: Step 1: Modeling (developing a decision tree), Step 2: Preferential judgment (conducting pairwise comparisons), Step 3: Calculating the relative weights of the group pairwise tables, Step 4: Calculating the final weights [13].In ranking the decision options, we must multiply the relative weights of each element by the weight of the higher elements to obtain the final weight. The final weight is obtained for each option and is thus called absolute weight. Then the question posed is: to what extent can we rely on the ranking of the proposed method? The compatibility rate was used to answer this question. The compatibility rate is the mechanism that specifies the compatibility of the comparisons. Usually, when the compatibility rate, CR is ≤ 0.1, the referee is multiplied and the weight is considered reliable. The matrix index is first multiplied by the weight vector of the indices to determine the compatibility rate [14].The group analytical hierarchy process technique on the Expert Choice 2000 software package was used to calculate the analytical hierarchy in the present study. The acceptable compatibility rate for this study was less than 0.1 hence, the software reported the ranking according to this criteria.
3. Results
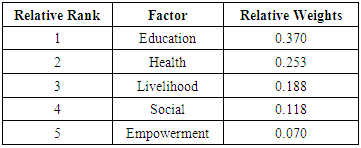
- Based on three-round Delphi method among experts, education had the highest rank among other indicators, the effect of which was 37% and empowerment ranked the least, with a 7% effect (Table 1; Figure 1):
|
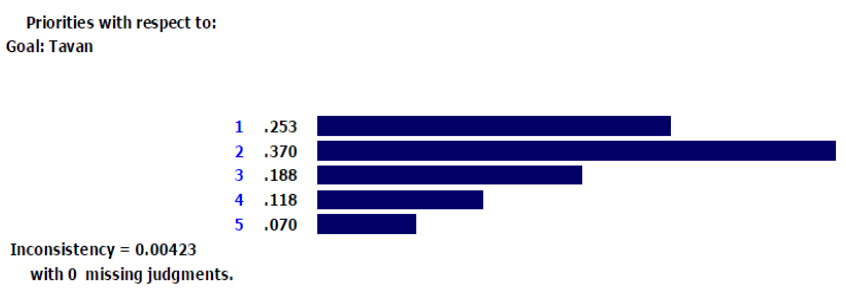 | Figure 1. Weights of the main indicators |
|
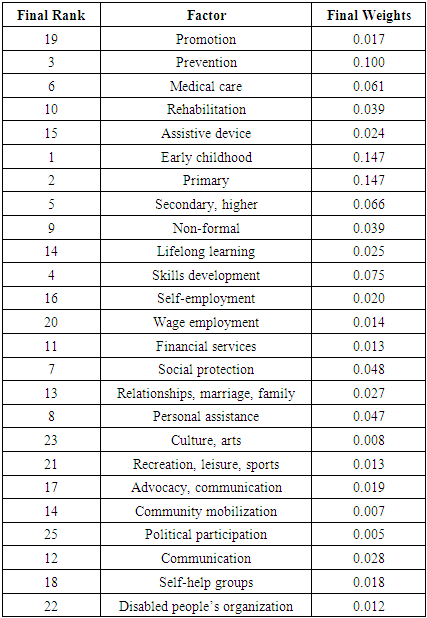
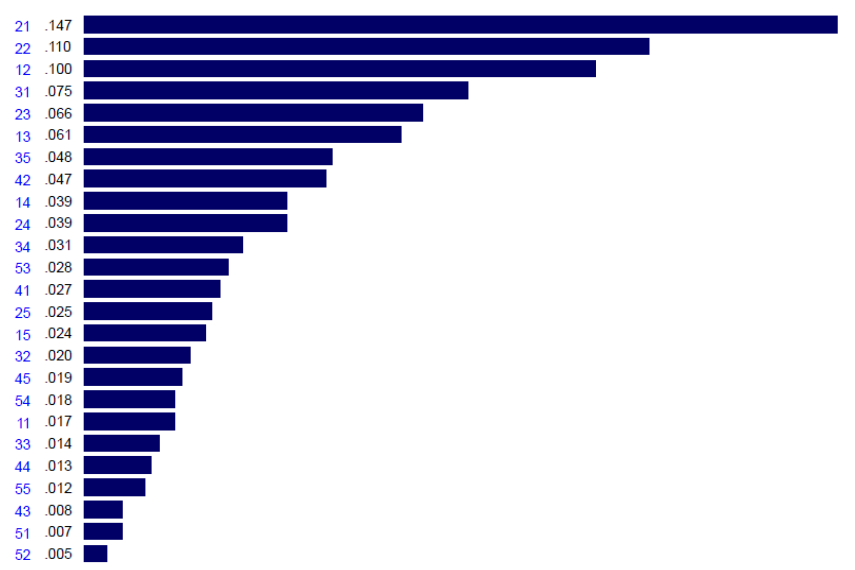 | Figure 2. Weights sorted under the main indicators |
4. Conclusions
- The purpose of the present study was to rank the desirability indicators of community-based rehabilitation based on an analytical hierarchy process. Thus, the final model of community-based rehabilitation was obtained as shown in "Figure 3".
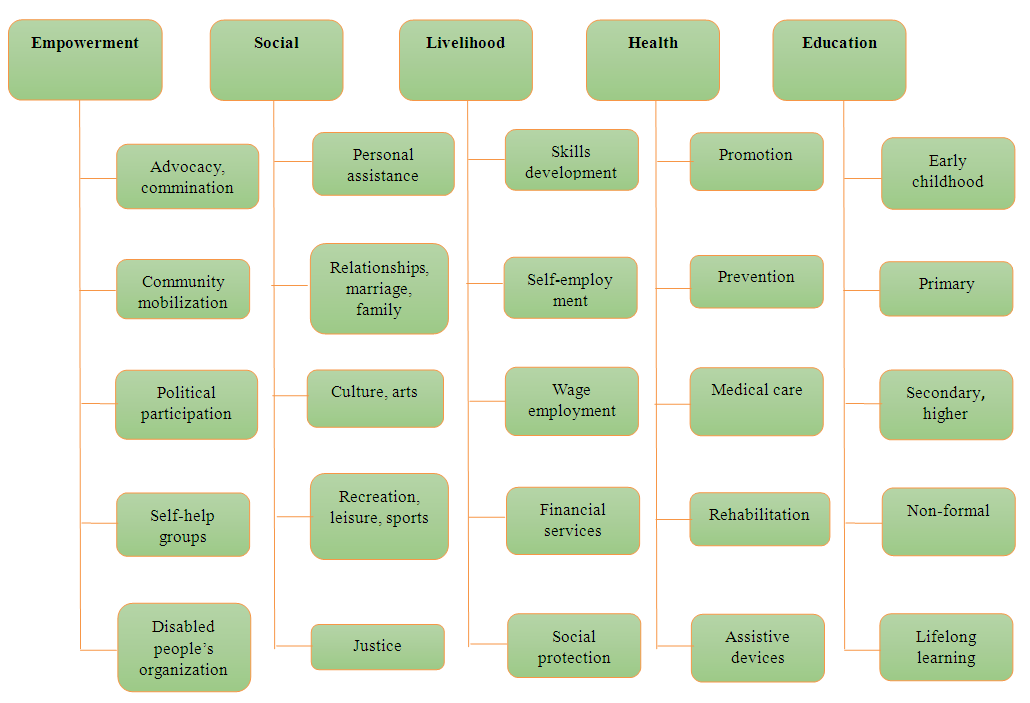 | Figure 3. Ranking matrix of community-based rehabilitation elements in Tehran Province |
ACKNOWLEDGEMENTS
- Thanks are due to all the experts of the Welfare Organization who co-operated in accomplishing this research. This article is the result of a Master's Degree thesis in Business Administration (Internal), approved by the Faculty of Management, Islamic Azad University, Firoozkooh Branch, Firoozkooh, Iran.