-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Psychology and Behavioral Sciences
p-ISSN: 2163-1948 e-ISSN: 2163-1956
2016; 6(2): 76-81
doi:10.5923/j.ijpbs.20160602.07

Trauma, Depression, and Resilience among Women Living with HIV/AIDS in Kenya
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLJeong Ryu 1, 2, Youngran Kim 2, Youngsook Kim 2, Heesang Yun 3, Dongil Han 2, Namhee Choi 2
1Yonsei University, South Korea
2Seoul Institute for Narrative Studies, South Korea
3DSeoul Women’s College of Nursing, South Korea
Correspondence to: Namhee Choi , Seoul Institute for Narrative Studies, South Korea.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Kenya has one of the world’s worst HIV and AIDS epidemics. In 2011, an estimated 1.6 million people were living with HIV and nearly 62,000 people died from AIDS-related illnesses including Korogocho, the worst slum area with 14% HIV prevalence. Even though awareness of HIV and AIDS in Kenya is high, many people living with the virus still face stigma and discrimination. Studies have shown that although people are aware of the basic facts about HIV and AIDS, many do not have the more in-depth knowledge that address issues of stigma. Especially social stigma of HIV to women is an urgent issue in Kenya. Especially women with HIV suffered from stigma and discrimination to break themselves down. Their severe depression and psychological trauma is the most significant cause of their deprived quality of life. Kenya women have been exposed to intense and ongoing trauma and depression since diagnosis of HIV/AIDS. Among 122 women living with HIV/AIDS in Korogocho, Kenya, we examined the prevalence and severity of pre traumatic experience (PET), impact of event (IES-R), depression (CES-D), internal stigma (ISS), and resilience (RS). Results revealed a high prevalence in emotional impact of event in women living with HIV/AIDS (86%); 65.3% reported severe depression after diagnosis of HIV/AIDS. As expected, depression was significantly correlated with both impact of event and internal stigma. Hierarchical regression analyses revealed the association between IES-R score and CES-D scores persisted even after controlling for relevant demographic variables. The most difficulties on living with HIV/AIDS were emotional distress, physical health, social relationship, and financial problems. Implications for improving the psychological functioning and resilience of women living with HIV/AIDS are discussed.
Keywords: Trauma, Depression, Resilience, Psychosocial distress, Women living with HIV/AIDS (WLHA)
Cite this paper: Jeong Ryu , Youngran Kim , Youngsook Kim , Heesang Yun , Dongil Han , Namhee Choi , Trauma, Depression, and Resilience among Women Living with HIV/AIDS in Kenya, International Journal of Psychology and Behavioral Sciences, Vol. 6 No. 2, 2016, pp. 76-81. doi: 10.5923/j.ijpbs.20160602.07.
1. Introduction
- HIV-status disclosure by people living with HIV/AIDS is widely advocated as a means to prevent HIV transmission (UNAIDS/WHO, 2000) and as such has received much attention in the international health literature (Maman, et al., 2001; Medley et al., 2004). On an individual level, disclosure facilitates HIV-infected individuals to seek treatment and care and supports adherence to complex treatment regimens (Norman, Chopra and Kadiyala, 2005). Broadly speaking, disclosure may also assist HIV-prevention efforts in society as it enables others to learn from the experiences of people living with HIV (Paxton, 2002). The World Health Organization (WHO) suggests that activities used in support groups for people living with HIV may help HIV-positive women develop the confidence to share their status with others (UNAIDS/WHO, 2000). In the last decade, there has been a dramatic rise in the number of HIV/AIDS support groups in Kenya. Despite these propose benefits, many women living with HIV choose not to disclose their status. Literature from sub-Saharan Africa cities fear of blame, violence and abandonment by a partner, as well as stigma and isolation within the home and community as major barriers to status disclosure by HIV-positive women (Greff et al., 2008). Disclosure has significant health implications, firstly because the negative outcomes of disclosure can be detrimental and severe for the women affected, and secondly because low rates of disclosure may increase cases of HIV transmission to others (UNAIDS, 2006).The HIV epidemic remains one of the most significant problems affecting Kenya, with an estimated 5.6% of the population infected (KAIS, 2012). The proportion of women infected with HIV has risen in recent years, and it is estimated that women account for two-thirds of the HIV-positive adults in Kenya. HIV-prevention efforts are hindered by widespread poverty – almost 20% of people live on less than US$ 1.25 a day (UNDP, 2010).Kenya, HIV prevalence has been reducing in the last five years due to better treatment and care. In this period the prevalence reduced from 7.6% in 2007 to 5.6% in 2012 (KAIS, 2012). This survey revealed that fifty eight percent of HIV-infected persons aged 15 to 64 were eligible for ART but only 63% are currently on ART. In spite of the reported reduction in the prevalence of HIV and AIDS, the disease continues to impact women in Kenya significantly. The disease is more prevalent among women aged 15 to 64 years compared to men in all provinces. Central and Nyanza Province were the only regions where the prevalence of HIV and AIDS increased marginally with the rest of the country reporting reduction (KAIS, 2012). An assessment of the psychosocial challenges and health needs of women living with HIV in an area where the prevalence has been increasing in the recent past is necessary in order for health practitioners and the government to implement successful interventions. Hence this study aimed at determining the psychosocial and health needs of women living with HIV in Central Province, Kenya. The study further explored the coping strategies employed by the women to mitigate against the effects of the HIV and AIDS on them.
2. Methods
- This was exploratory study carried out in Central Province in Nairobi, Kenya. Participants were drawn from Korogocho and Nyeri. They comprised 122 women living with HIV and AIDS aged between 24 to 60 years. An interview schedule was used to determine the challenges that the women faced and how they coped. The schedule interrogated women on their background education levels, occupation, when they got infected, how infection with HIV altered their lives, the psychosocial and health needs that they faced and how they coped with them. MeasuresGeneral InformationParticipants completed measures addressing demographics (age, education status, employment status, marital status, the number of family member, experience of losing their child (ren), income), the number of HIV-related physical symptoms, needs after notifying HIV-positive, social support, number of pre-experience traumatic event etc.Psychological StatusPsychological distress were used to assess to psychological Impact of trauma, depression, internal stigma from their surrounds through IES-R (Impact of Event Scale – Revised), CES-D (Center for Epidemiologic Studies - Depression), ISS (Internal Stigma Scale). The 22-item IES-R (Greenberg, 2013) was used to assess psychological trauma from HIV-positive with factors of intrusive, avoidance, hyper-arousal, and chance using a 5-point likert-type response ranging from 0 (not at all) to 4 (always). Participants were asked to respond during past 7 days. Depression were assessed using measures 20-item CES-D (Radloff, 1977; 1986). Participants were asked to respond on 4-point scale ranging from 0 (few, under 1 day) to 4 (quite often, 6~7 days) during last week. The 28-item HIV stigma scale; internal stigma scale (Sowell et al., 1997) were used to assess persons’ internalized stigma from their community, and based on a 7-day period using five response items from 0 (not at all) to (always). Benefit FindingsThe extent to which participants found benefits in their situation was assessed using a short-version 6-item resilience scale (Cambell-Sills & Stein, 2007) from original version 27-item the Connor-Davidson Resilience Scale; CD-RISC using 6-point response items from 0 (not at all) to 5 (very much).
3. Results
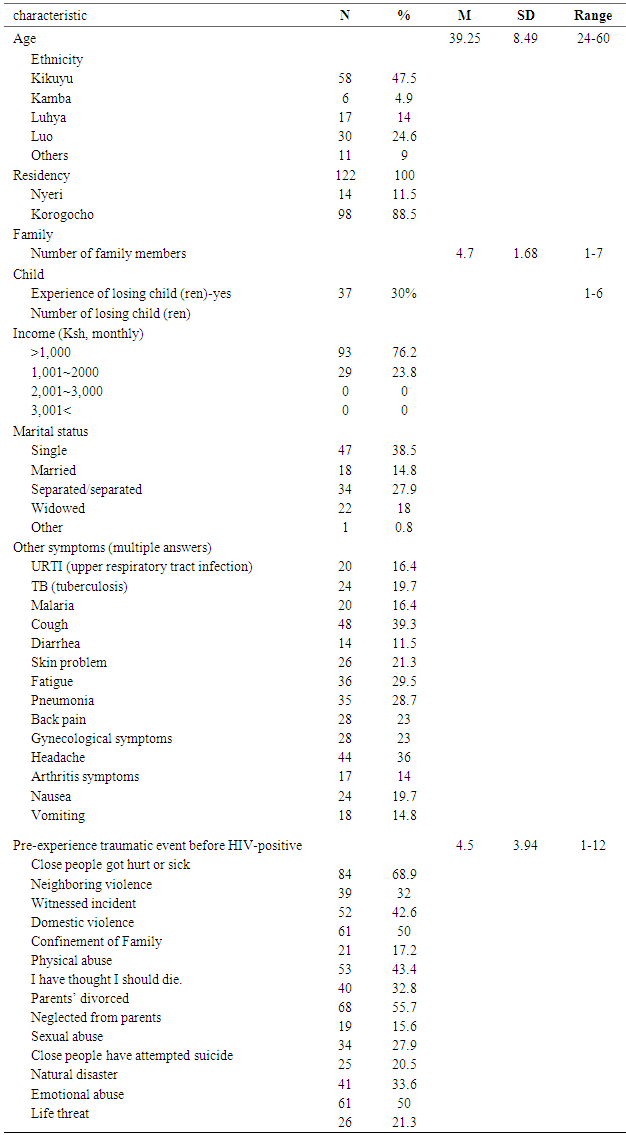
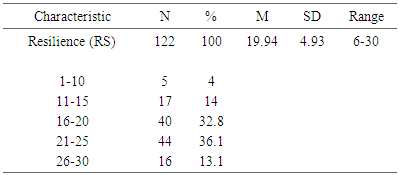
- General InformationThe demographic, general information, symptoms, and traumatic experience before HIV-positive of the sample are presented in table 1.
|
|
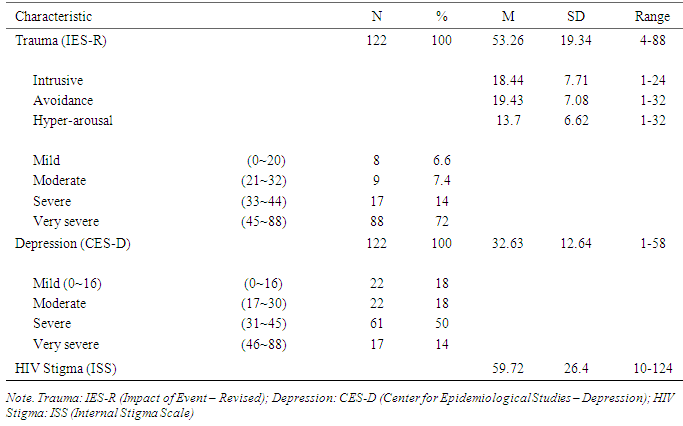
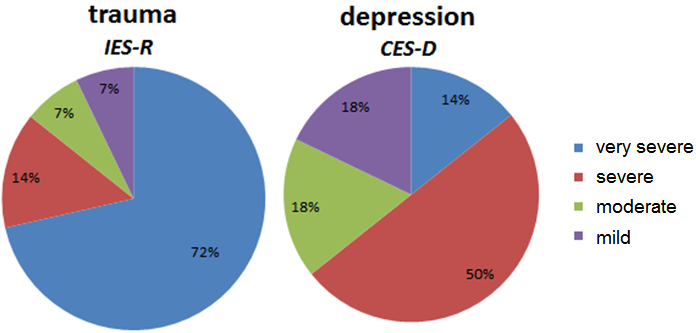 | Figure 1. Severity of trauma (IES-R) and depression (CES-D) |
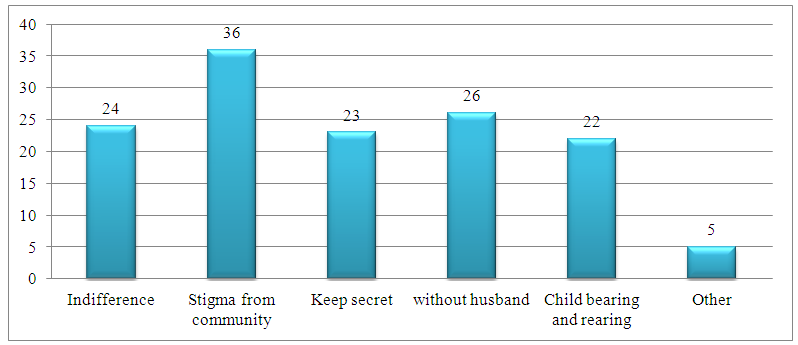 | Figure 2. Difficulties of Women living with HIV |
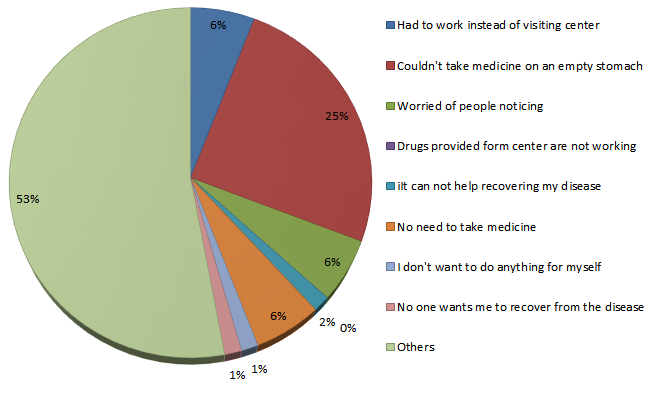 | Figure 3. Internalized stigma of PLWH |
|
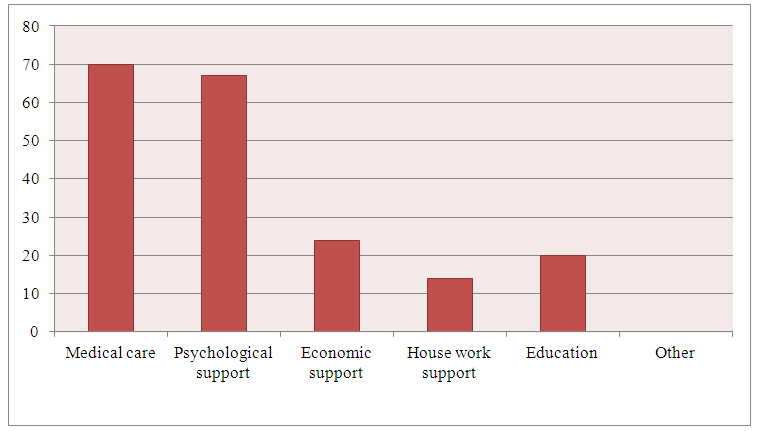 | Figure 4. Most helpful services for PLWH |
4. Conclusions
- The women living with HIV showed resilience with determination to live in spite of the tangible threats of a well-known chronic disease. Perceived or self-stigma added to the impact. Psychological and social support is necessary to address the impact of the disease. The government should include counseling as a pertinent component of therapy and provide the basic nutrition for these women. Support to establish small scale business is crucial in order to discourage vulnerable women from moving into commercial sex. Stigma has been defined as ‘an undesirable of discrediting attribute that an individual possess, thus reducing that individual’s status in the eyes of society (Brown et al., 2001; Goffman, 1963)’.