-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Psychology and Behavioral Sciences
p-ISSN: 2163-1948 e-ISSN: 2163-1956
2016; 6(2): 47-52
doi:10.5923/j.ijpbs.20160602.02

Critical Appraisal of Fish's Clinical Psychopathology Signs and Symptoms in Psychiatry (Third Edition)
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRajnish Raj1, Ravinder Singh2, Rakesh Tilak Raj3
1Department of Psychiatry, Government Medical College and Rajindra Hospital, Patiala, India
2Department of Psychiatry, Post Graduate Institute of Medical Education & Research, Chandigarh, India
3Department of Dermatology and Venereology, Government Medical College and Rajindra Hospital, Patiala, India
Correspondence to: Rajnish Raj, Department of Psychiatry, overnment Medical College and Rajindra Hospital, Patiala, India.
| Email: | drrajnish_raj@yahoo.com |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of authors are to highlight the errors in the third edition of Fish's Clinical Psychopathology and inform its readers to use their discretion before accepting the edited version as the final word. Materials and Methods: Textual analysis of words quoted in third edition of Fish and review of their meaning with reference to various Psychiatric textbooks, Advance Oxford English dictionary, Taber's Cyclopedic Medical dictionary, Penguin dictionary of Psychology, The Penguin dictionary of Philosophy, web based search engines e.g., PubMed, SCOPUS, EMBASE, EBSCO, Index Copernicus, Ulrichs, Hinari, Google scholar etc., were used to extract the relevant data and decipher the intended truth conveyed therein. 39 records were initially identified. 30 studies were included from review of literature; seven records were excluded because of duplication in extended phase and two more studies were excluded as they reported effects of RLS on pathophysiology etc., which was not the intended purpose of the study. Results: There is discontinuity in copying and interpretation of the text with meaning either lost or distorted, possibly, due to inadvertent human error in the subsequent editions of Fish's Clinical Psychopathology. New operational definition of Hallucination is proposed, Delusional Perception redefined with reference to Fish's earlier edition, Delusional memory segregated from sudden delusional idea, subtleties between Aphasia and speech disorder enumerated for being ontological and epistemological distinct and delusional parasitosis reestablished as Ekbom syndrome. Conclusions: Both the deductive and inductive reasoning were applied to analyze the information. The inferences were drawn on facts rather than fiction or partial truth abou t Restless Leg Syndrome, Delusion Disorder of Infestation or parasitosis, Aphasia, Delusional Perception, and Hallucination. Thus, this study helps in restoring sanctity of the Fish's Clinical Psychopathology.
Keywords: Ekbom syndrome (ES), Restless leg-syndrome (RLS), Willis-Ekbom disease (WED), Wittmaack-Ekbom syndrome (WKS), Aphasia, Delusion Perception and Hallucination
Cite this paper: Rajnish Raj, Ravinder Singh, Rakesh Tilak Raj, Critical Appraisal of Fish's Clinical Psychopathology Signs and Symptoms in Psychiatry (Third Edition), International Journal of Psychology and Behavioral Sciences, Vol. 6 No. 2, 2016, pp. 47-52. doi: 10.5923/j.ijpbs.20160602.02.
Article Outline
1. Introduction
- "The fault, dear Brutus, is not in our stars,But in ourselves, that we are underlings" –Shakespeare.In 1967, Frank Fish produced a 128 page volume on psychopathology, it was revised and edited by Max Hamilton in 1974, reprinted second edition in 1985 [1].Revising Fish's Clinical Psychopathology has been humbling and exciting experience for the authors of third edition. They strived to retain the spirit of Fish's original work, took linguistic liberty to change its meaning, incorporate new materials relating to personality disorder, cognitive distortion, defense mechanisms, memory and unusual psychiatric syndromes. Notwithstanding these revisions, they trust that this text remains true to the spirit of Fish's original Clinical Psychopathology, if it does not, the fault lies with them [2].
2. Materials and Methods
2.1. Information Source
- A systemic review of literature and articles on psychiatry in English was conducted by searching in PubMed, SCOPUS, EMBASE, EBSCO, Index Copernicus, Medline, Ulrichs, Hinari, Google scholar and Cochrane Library. Additionally, grey literature (referring to documents produced in print and electronic formats protected by intellectual property rights was searched. Free text search terms were "Ekbom syndrome", "delusional parasitosis", "delusional disorder of infestation", "Restless leg-syndrome", "Willis-Ekbom disease", "Wittmaack-Ekbom syndrome", "Aphasia", "Delusion Perception", "delusional memory" and "Hallucination". The following terms were also included as MeSH terms combined with the Boolean term " All Fields AND negative [All Fields]; AND diagnosis [Subheading] OR diagnosis [All Fields] OR symptoms [All Field] OR diagnosis MeSH terms] OR symptoms [All Field] AND "Ekbom" etc., and others as stated above [Mesh Terms] to support firmer conclusion." Dates of publication were not included as limitation. This search was conducted in November 2015 using Cochrane Library.
2.2. Study Selection
- The aims of authors are to highlight the errors in the third edition of Fish's Clinical Psychopathology. For inclusion in the review of research, data was confined to Nosological classification and subsequent changes for defining psychic/mental life in descriptive psychopathology textbooks, abnormal psychology, and Journal of psychiatry. Psychiatric textbooks, Advance Oxford English dictionary, Taber's Cyclopedic Medical dictionary, Penguin dictionary of Psychology and Penguin dictionary of Philosophy were also screened.
2.3. Data Collection and Analysis
- Data were screened for eligibility and abstracted from each of the studies independently by all the three authors (RR, RS and RTR) and any disagreement was resolved by consensus and Cohen's kappa for interrater agreement between evaluators was 0.903.
2.4. Assessment of Bias
- Publication bias was taken into consideration with the possible overestimation or underestimation of the reported effect associated with the review of literature on the hypothesis that studies with the statistically significant results or otherwise may be more likely to be published compared to those with non-significant results.
2.5. Record Retrieval
- 32 records were identified through data base research and 7 additional records from other sources. Total 39 records were screened; out-off which 7 records were excluded because of duplication in extended phase. Then, 32 records were assessed for study eligibility from which 2 studies of RLS excluded as they were outcome effects on pathophysiology and pregnancy. Finally, 30 studies were included in the review of research [Figure 1]. The critical analysis of their textual content interpreted in view of the earlier versions of the Fish's Clinical textbooks and thus, highlighting their subsequent changes and inadvertent distortion of words, which conveys partial truth or a lie. The wisdom of readers is invoked in supporting the intended truth.
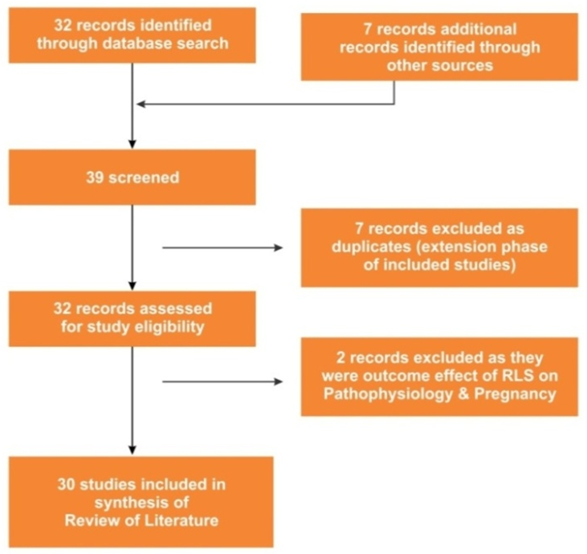 | Figure 1. Flow-Diagram Indicating Selection of Studies Included in Review of Literature |
3. Errata
3.1. Errata 1
- Ekbom syndrome: also known as restless leg syndrome, this is a common sensorimotor disorder with a prevalence of 1-5% [2].Restless leg syndrome (RLS) is known as (Wills-Ekbom syndrome or Wittmaack-Ekbom syndrome) whereas delusional parasitosis as (Ekbom syndrome).Historically, RLS was also described by Francois Boissier de Sauvages (1763), Magnus Huss (1849), Theodur Wittmaack (1861), George Miller Beard (1880), Georges Gilles de la Tourette (1898) [3, 4]. However, both are entirely two different conditions that were described by Karl-Axel Ekbom. The symptoms of RLS are an urge to move the limbs with or without sensations; improvement with activity; worsening at rest; at evening or night. Genetically, four genes i.e., MEIS1, BTBD9, MAP2K5 and PTPRD were found to be associated to RLS [5]. The possible association was of low iron levels and dopamine dysregulation in the substantia nigra. It is more common in individuals with iron deficiency, pregnancy, and end-stage kidney disease [6, 7].Delusion Parasitosis (Ekbom syndrome):Delusions of infestation have been described by Hopkinson (1970) and by Reilly (1988) [8, 9]. Historically, the conditioned is named after Ekbom, a Swedish neurologist (1937; 1938) but was probably first described in 1894 in France by Thiedierge, and again in 1896 by Perrin, both were dermatologists. In Ekbom's syndrome, (1938) the patient believes that he is infested with small but microscopic organisms. Patients also believed that they had a spider in their hair, worms and lice beneath the skin or infestation with various insects. It is also called zoophobia, parasitophobia, acarophobia (Myerson, 1921) and Dermatozoenwahn (skin-animal-delusion) (Skott 1978) [10, 11]. The psychodynamic factors for emergence of delusion of infestation are defense of guilt and projection. Its formation in female gender was influenced by her sexual role and activity e.g. who become pregnant, possibly unwillingly, or is ashamed at her loss of virginity, venereally affected by may feel that she has been contaminated or even infested. It is most common in older people and in females over the age of 40 years. They provide skin scrapings, bits of debris (in paper, small jars). In addition, they extensively elaborate pest, their life cycle, and behaviors. The mean duration of delusion was 3.0±4.6years (median, 1 year) and reject any possibility of psychological or other explanations “I'm not crazy,” or “I am not imagining this”.
3.2. Errata-2
- Aphasia or dysphasia is a disorder of speech resulting from interference with the functioning of certain areas of the brain [2].Aphasia is a disorder or loss of language. It contains both verbal and non-verbal (gestural) expression and dysphasia as unintelligent speech, impairment of, or difficulty with language. It is divided into two types sensory (receptive) and motor (expressive) [12].The dissociation between poorly articulated speech and intact language indicates that these are two different functions.Speech is an aspect of language that corresponds to the mechanical and articulatory functions to vocalize [13]. Thus, for language to become speech the vocal cords, palate, lips and tongue needs to perform a complex and synchronized intricate steps. Dysarthria is a disorder of articulation and caused by lesions of the brainstem such as bulbar and pseudo-bulbar palsy. Aphonia is the loss of ability to vocalize. Dysphonia denotes impairment with hoarseness but without complete loss of function [12, 13].Language is a complex system based on number of elements including phonemes, syntactic structure, semantics, prosody and pragmatics. The purpose is to aid communication, express thoughts, and encode facts to memory.
3.3. Errata-3
- Hallucination 'a perception without an object' (Esquirol, 1817) [1, 2].Jasper, 1962 defined hallucination as a 'false perception which is not sensory distortion or a misrepresentation, but which occurs at the same time as real perception' [1, 2].The word "Perception" was not defined anywhere in Fish's Clinical psychopathology. However, it was used to define hallucination. It creates ambiguity in the minds of readers, and does not help in understanding meaning of hallucination.Awareness of an object as described by Jasper, 1962.Object is that to which we confront, look at, apprehend, think about or recognize with our inner eye or sense organs. It exists for us in the form of perception or Ideas. As perceptions, the objects stand bodily before us tangible, felt, and apperceived or with a quality of subjectivity. It has three elements: qualitative aspect of perception, spatial and temporal arrangement, and purposeful act of perception [14].Sensation is first stage in receiving information from outside the self. The sensory system includes visual, gustatory, auditory, tactile, and olfactory [13]. Mental image is an inner representation of external world and recognized to be arising in mind's eye of the person.Hornby in 1990 defined perception as the ability to see, hear or understand; quality of understanding; insight and; way of seeing or understanding [15].Thomas et al., 1990 stated that perception in Latin is percepitio, which means to perceive. 1. Process of being aware of objects; consciousness. 2. Process of receiving sensory impression. 3. The elaboration of a sensory impression; ideational association modifying, defining, and usually completing the primary impression or stimulus [16].Elliot et al., 2001 defined Perception as appreciation, apprehension, awareness, cognition, comprehension, consciousness, discernment, insight, instinct, intuition, knowledge, observation, realization, recognition, sensation, sense, understanding, view [17].Sadock et al., 2015 defined perception as conscious awareness of elements in the environment by mental processing of sensory stimuli; or mental process by which all kinds of data, intellectual, emotional, and sensory, are meaningfully organized. Whereas, Apperception was defined as awareness of meaning and significance of a particular stimulus as modified by one's own experiences, knowledge, thoughts, and emotions [18].The above definitions for perception are vague or overinclusive and refuted as they fail to convey the intended meaning.Perception is of two staged steps i.e., a) receiving sensation from the exteroceptive or interoceptive environment; b) encoding, transforming, and transmitting information into cortical levels and decoding into understandable meanings i.e., appraising. They are classified into two types: sensory distortion and sensory deception [30].Recognition [Conscious awareness] of felt [emotional apperception] sensations [external or internal environment] or inference of sensation is Perception by Authors. The recognition of stimuli was processed by two competing models i.e., bottom-up and top-down. Bottom-up model consists of primary process that transforms sensation into recognition of an object having form, shape, colour, motion and location in space. Top-down process involves influence of learned experience to sensory information by template-matching, feature-matching, recognition-by -component and configural-model [30].Jasper, 1962 defined Hallucination as "false perceptions that are not in any way distortions of real perceptions but spring up on their own as something quite new and occur simultaneously with and alongside real perception" [14].Smythies, 1956 defined hallucination as exteroceptive or interoceptive percept that does not correspond to an actual object [19].Slade, 1976 defined three-operation definition of hallucination (a) percept-like experience in absence of an external stimulus; (b) percept-like experience that has full force and impact of a real perception; and (c) percept-like experience that is unwilled, occurs spontaneously and not controlled by the percipient [20].Spitzer, 1994 concluded that patient could distinguish between real and hallucinatory experiences [21].Cutting, 1997 defined perception without an object or appearance of an individual thing in the world without any corresponding material event. Hallucination takes place at the same time as normal stimulus [22].Aggernaes, 1972 who elaborated on Rasmussen description and pointed out six qualities of reality in hallucination. It has 1) sensation; 2) relevance of its need or action; 3) quality of objectivity; 4) certainty of its objective existence; 5) involuntary and 6) independence [23].DSM-5, 2013Hallucinations are perception-like experiences that occur without external stimulus. They are vivid and clear, with the full force and impact of normal perception, and not involuntary control. They are perceived to be distinct from the individual's own normal thought [24].New operational definition proposed by the authors regarding formation of Hallucination contains the following parameters viz. form, stream, possession, and content.Form of hallucinationHallucination is defined as "false perceptions of [interoceptive Smythies, 1956 or exteroceptive Jasper, 1962 percept] that [does not correspond to an actual object Esquirol, 1817; Cutting, 1997] are not in any way distortions of real perceptions [i.e., neither sensory distortion Fish, 1967; 1974 in intensity, quality and location of shape or size in space nor misrepresentation, Fish, 1985 i.e., illusion of completion, affect and fantastic] but spring upon their own [unwilled, Slade, 1976 or involuntary i.e., not in control DSM-5, 2013; Kaplan and Sadock, 2015 of the preceptor] as something quite new [distinct DSM-5, 2013] with [conviction of its reality Aggernaes, 1972] or [having insight, Spitzer, 1994 of its after images that persistently cause interference in attention] though person is aware and his consciousness is clear [DSM-5, 2013; Kaplan and Sadock, 2015] and occurs simultaneously [in space and time by Authors] alongside real perception [other external object, Sims, 2015]; kept as secret i.e., not publicized [Sims, 2015] and deliberately revealed after [establishing intended empathetic relationship of trust and intimate commune between the observer and observed] by Authors."Content of hallucinationThey are assessed on the following parameters: quality of noises or voices or any other sense modality, age, sex, location and direction in space and time, frequency, duration, continuity, verbatim of content in patients language with reference to its address to others as first, second and third person, commenting or discussion, attitude and reaction of patient towards his hallucination.Further, research is required to validate the clinical utility and applicability of the operational definition for its internal consistency and reliability.
3.4. Errata-4
- Delusional perceptIn delusional perception, the new meaning cannot be understood as arising from the patient's affective or previous attitude [26]. Schneider emphasized the importance of this symptom's 'two memberedness', as there is perceived object to the subject's perception of this object, and a second link to the new significance of this perception. Schneider divided delusional memory into delusion percept and sudden delusion ideas [26]. "A new meaning usually in the sense of self-reference, to a normally perceived object. Schneider suggested that the delusional experience can be reduced to three, viz. delusional mood, delusional perception and sudden delusional idea [1].For example,"They are of royal descent because they remember that the spoon they used as a child had a crown on it, this is usually a delusion percept" [26].On the other hand,"They are of royal descent because when they were taken to a military parade as a small child the king saluted them, this is sudden delusion idea because the delusion is contained within the memory and there is no 'two memberedness' [26].The above edited version of the text is fraught with errors and inconsistencies.The succinct definition of delusion percept is 'new meaning which is of delusional significance to the normally perceived event'.Original transcript for delusion percept with changes [26]."They [He is] are of royal descent [Delusional meaning] because they [He] remember [Memory] that the spoon they [He] used [Past event] as a child had a crown [Signifies royalty] on it, this is usually a delusion percept."It explains neither the timing of delusion nor the arrival of secondary link to the perceived event.Delusion is a false, firm, fixed belief, not amenable to correction, in-spite of the evidence contrary to it; having full conviction of its reality and keeping out of patient's social and cultural background [26, 27]. As earlier defined by the authors perception is [recognized felt sensations or inference of sensation] that arises from either exteroceptive or interoceptive environment.Delusion perception incorporates two interwoven concepts in one [False belief and perception of sensations from within or without environment]. The timing, arrival, and location in space of its occurrence and having 'two memberedness' its hallmark. Textual meaning"He is of royal descent [New meaning of delusional significance] because he remembers [Memory] that the spoon [He is using in a 'now moment' has a crown, which he perceived as stimulus from exteroceptive environment] and he used as a child [Past event stored in memory] had a crown [signifies his link with royalty] on it, this is usually a delusion percept."Matussek's in 1952, through Gestalten theory explained Psychotic breakdown as a continuum of schizophrenic shifts, having three phases [25].a) Trema (loss of freedom for person, as if, surrounded by barriers),b) apophanous (statement of assertion or proposition) phase has three properties:-i) structure, straight, round, angular etc., ii) total qualities rough, smooth silky etc., iii) essential properties and its connection with animate, inanimate, and, or, both, either-or, neither-nor, partly full and empty, empty, full etc.c) apocalyptic phase is a fragmentation of psychic life.Conrad, 1958 accepted Matussek's theory and recognized three stages in delusional perception. 1) Pure apophany, believes that object is but cannot say what it is? The state of no-thingness.2) The prefabricated stage, thing-is.3) Essential properties become prominent to the patient, and know its meaning.Delusional perception is an example of external apophany [25].Original transcript for delusion memory with changes [26]."They [He is] are of royal descent [new meaning of delusional significance] because when they [He was] were taken to a military parade as a small child the king saluted them [Him], this is sudden delusion idea [Delusional memory] because the delusion is contained within the memory and there is no 'two memberedness'."
4. Discussion
- Ekbom syndrome was described as restless leg syndrome, which is a medical disorder whereas it is Delusional parasitosis, a disorder of mind. Aphasia was described as a disorder of speech instead of disorder/loss of Language. Hallucination was defined as "perception without an object" but the meaning of perception was not defined that itself needs further clarification and understanding as perception contains both the disorders of sensory distortion and deception. Delusion perception, delusional memory and sudden delusion idea are three distinct entities rather than subsuming sudden delusional idea into delusional memory.Casey and Kelly, 2007 in third edition of Fish Clinical Psychopathology inadvertently changed 'He' to 'they', which signifies more than one-person manifesting psychopathology as folie-e-deux, etc. and inadvertently described delusion memory as sudden delusion idea, which is erroneous that was not the intended purpose of Frank Fish in explaining phenomenology [26].Idea is a basic unit of thought; a psychic representation of sign and symbols of universe, consensually validated and universally accepted as truth to convey and share experiences (innate or experiential) with others, whereas memory is a stored information. Ideas for Plato, are forms or universals; Descartes a concept that is perceived directly in the mind; Locke's ideas are mental events, a brain state underlies it, and it is derived in some fashion from experiences. Hume stated ideas as 'mental reconstructions of perception'. Kantian idea is a 'concept of reason' that is transcendent and Hegelian an 'absolute-truth' [28, 29].Sudden delusion idea is autochthonous, sudden onset, fully formed, immediate, out of blue and un-understandable (Jasper, 1962) [14]. It is delusional inspiration, an internal apophanous stage; a mode of understanding or knowing characterized as direct and immediate and occurring without conscious thought or judgement. However, in delusional memory, there is a break in the inner representational aspect of psychic life i.e., images, ideas, thoughts etc., that are stored and come into prominence on psychotic breakdown [25].
5. Conclusions
- The above mentioned errata require early corrections to restore sanctity of the Fish's classic text on Clinical Psychopathology that enables professionals to build essential foundation in descriptive psychopathology, helps to communicate with patient, their families, and other professionals for psychiatric health care, and envisions future research in mental health with precision.
6. Implication/Salient Features of Study
- It is a comparative textual analysis of various definitions proposed by Frank Fish to delineate psychic phenomenon and forms the foundational course in descriptive psychopathology in Fish's Clinical psychopathology. The inadvertently changes in subsequent editions distorted the meaning vis-a-vis other Psychiatric Text Books and relevant journals.
7. Future Directions
- The relevant proposed changes in the text bring the sanctity of Fish's Clinical Psychopathology and act as a template for incorporating new phenomena e.g., inception, conception, apperception, insight, inspiration, intuition etc., and achieve consistency in understanding and analysis of patient's psychic life and thus, helps in communicating across other health care professionals.