-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Psychology and Behavioral Sciences
p-ISSN: 2163-1948 e-ISSN: 2163-1956
2014; 4(3): 87-91
doi:10.5923/j.ijpbs.20140403.01
The Reliability and Validity of the Adolescent Subjective Well-Being Scale in Japan
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLWatanabe T 1, Ito S 2, Okumura R 2, Tanaka E 3, Tomisaki E 3, Tokutake K 3, Wu B 3, Mochizuki Y 3, Arioka S 3, Anme T 2
1Japan University of Health Sciences, Satte, 340-0113, Japan
2Tobishima Health center, Tobishima, 490-1434, Japan
3University of Tsukuba, Tsukuba, 305-8575, Japan
Correspondence to: Watanabe T , Japan University of Health Sciences, Satte, 340-0113, Japan.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
[Aim] The Adolescent Subjective Well-Being Scale was developed to measure quantitatively adolescents’ subjective well-being; its reliability and validity were also examined. [Method] Drawing from the Philadelphia Geriatric Center Morale Scale developed by Lawton et al. in 1972, which is used widely in gerontology, 10 subjective well-being scale items were constructed. Being high in morale means that one is satisfied, has one’s own place, and has accepted inevitable truths. A self-administered questionnaire was completed by junior high school students (aged 13 to 15 years) residing in a rural village (T) near a large city in 2002, 2005, 2008, and 2011. The questionnaire was distributed by hand to each household and left there to be completed. The items were evaluated using a three-point scale. Factor analysis was undertaken to confirm the factor structure, and a reliability coefficient was determined for each sub-scale. The Spearman’s rank correlation coefficient was then calculated for the relationship between total scale score with sleep patterns, stress level, and satisfaction with life. [Results and discussion] A subjective well-being scale, comprised of 3 factors and 10 items, was developed. Data were obtained from 433 respondents (135 in 2002, 115 in 2005, 97 in 2008, and 86 in 2011). Of these, 387 (120 in 2002, 102 in 2005, 85 in 2008, and 80 in 2011; no missing data) were analyzed, along with the items that made up the scale. Factor contribution of the three-factor solutions was 1.86 for the first factor, 1.68 for the second factor, and 1.45 for the third factor. Based on the characteristics of the questionnaire items that constituted each factor, the first factor was named “affect,” the second “self-recognition,” and the third “adaptation to life.” The Cronbach’s alpha coefficient was .62 for the first factor, .57 for the second, .52 for the third, and .71 for the overall scale, which confirmed the scale’s internal consistency reliability. The correlation coefficient between total scale score and sleep patterns was r = .22 (p < .001), between total scale score and stress level was r = -.50 (p < .001), and between total scale score and satisfaction with life was r = .39 (p < .001). Thus, a significant positive correlation with sleep patterns and satisfaction with life, and a significant negative correlation with stress level were indicated. These results confirmed the scale’s criterion-related validity. Therefore, the scale, consisting of 3 factors and 10 items, could be used to examine young people’s subjective well-being.
Keywords: Subjective Well-Being, Adolescence, School Health, Mental Health
Cite this paper: Watanabe T , Ito S , Okumura R , Tanaka E , Tomisaki E , Tokutake K , Wu B , Mochizuki Y , Arioka S , Anme T , The Reliability and Validity of the Adolescent Subjective Well-Being Scale in Japan, International Journal of Psychology and Behavioral Sciences, Vol. 4 No. 3, 2014, pp. 87-91. doi: 10.5923/j.ijpbs.20140403.01.
Article Outline
1. Introduction
- The WHO defines health as “a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity” [1]. As such, many studies in the field of gerontology pertain to physical, mental, and social wellbeing. Owing to the benefits of social relations and social activities, social well-being is related to life expectancy [2, 3] and physical function [4]. Mental well-being, which is related to subjective well-being and subjective sense of health, is hypothesized as being associated with participation in social activities [5].In addition, poor social and mental well-being during adolescence have been examined as mental health issues, and the seriousness and intractability of these issues have been reported [6, 7]. However, the problem of “mental health issues” during adolescence cannot be solved overnight. To support adolescents with mental health problems, it is necessary to assess their social and mental well-being. Health promotion, which is central to recent health policies, is a progressive idea that focuses not only on physical capacities, but also social and personal resources; it goes beyond the simple promotion of a healthy lifestyle to the endorsement of holistic well-being [8] Thus, the development of a scale that assesses well-being is urgently needed.We therefore developed the Adolescent Subjective Well-Being Scale (ASWBS), which quantitatively measures adolescents’ subjective well-being, and examined the scale’s reliability and validity in the present study.
2. Method
2.1. Construction of Scale Items
- To develop a scale that measures well-being, we first focused on the Philadelphia Geriatric Center Morale Scale (PGCMS) [9], which was developed through research on successful aging. Lawton theorizes that “high in morale” has three meanings: to be satisfied with oneself, a feeling of one’s own place/space in the environment, and the acceptance of truths that cannot be altered. The “positive-negative feelings continuum” that is measured by the morale scale is termed “subjective well-being” [9, 10]. This concept is applied to the adolescent as well as older persons from the perspective of life-span developmental psychology [11].We therefore created two categories: “positive emotion” and “negative emotion.” We then created ten items using examples from the PGCMS [10] in these frames. This process was conducted by three researchers and supervised by a psychology expert to ensure that the information was placed into the appropriate categories. Furthermore, we closely examined the content of each item to ensure that there was no overlapping of meaning.
2.2. Subjects, Method, and Survey Items
- This research was a complete survey conducted in a rural village (T) near a large city in Japan. A self-administered questionnaire was completed by junior high school students (aged 13 to 15 years) residing in T in 2002, 2005, 2008, and 2011. The questionnaire was distributed by hand to each household and left there to be completed. In addition to the subjective well-being scale items, the questionnaire contained items about basic attribution (gender, age), sleep patterns, stress levels, and subjective satisfaction with life. The 10 items of the subjective well-being scale were evaluated using a 3-point scale ranging from 1 (rarely) to 3 (always) (the point scale was reversed for negative questions). Sleep patterns were assessed through the question “do you sleep enough?” and subjects responded via the same 3-point scale format as described above. Stress was evaluated by the question, “have you experienced any stress in the past month?” which contained a 4-point response scale ranging from 1 (hardly) to 4 (a lot). Lastly, subjective satisfaction with life was assessed with the question, “are you currently satisfied with life?” which was in answered in a yes (2 points) or no (1 point) format.
2.3. Data Analysis
- First, descriptive statistics were obtained, and the distribution pattern of each variable was confirmed. Then, exploratory factor analysis was performed to create a scale that could appropriately measure adolescents’ subjective well-being. Having confirmed the factor structure, the reliability coefficient of each sub-scale was calculated. The Spearman’s rank correlation coefficient was also calculated to determine the relationship between total scale score and sleep patterns, stress level, and satisfaction with life.
2.4. Ethical Considerations
- Subjects were informed orally and in writing of the aim of the survey, use of the data, and sole use of the results for the study’s purpose. They were also told that there were no disadvantages associated with participating in the survey, that they were free to decide whether to fill in the questionnaire, and that there would be no consequences of refusing. Returning the completed questionnaire was considered as consent to participate. To ensure that questionnaire responses would not be revealed to a third party, an individual, sealable envelope was provided to subjects for return of the questionnaire. The study was carried out after obtaining approval from the Ethics Committee of the Faculty of Medicine at Tsukuba University.
3. Results
3.1. Subjects’ Attribution
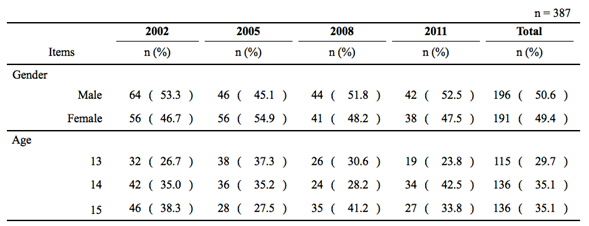
- Questionnaires were distributed to 433 subjects (135 in 2002, 115 in 2005, 97 in 2008, and 86 in 2011). Of these, 387 (120 in 2002, 102 in 2005, 85 in 2008, and 80 in 2011) were completed correctly, having no incomplete answers or omissions, and thus were used in the analyses (Table 1).The respondents were 196 boys (50.6%) and 191 girls (49.4%). One hundred and fifteen were 13 years old (29.75), 136 were 14 years old (35.1%), and 136 were 15 years old (35.1%).
3.2. Factor Analysis Results
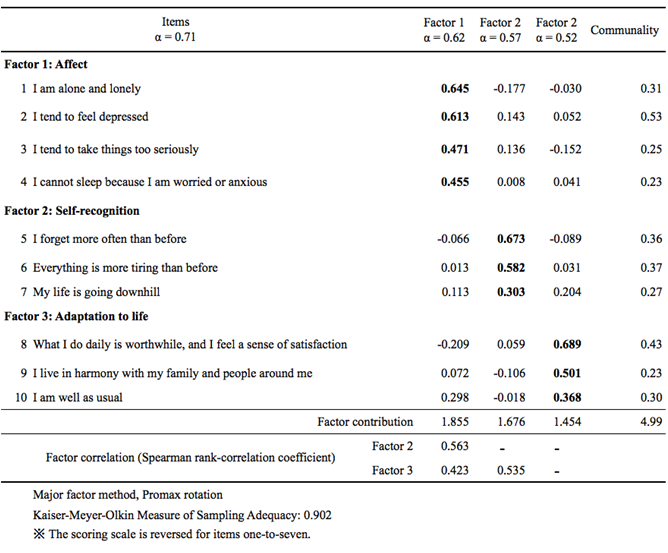
- The distribution of each of the 10 items that comprised the subjective well-being scale showed no multivariate normality, and correlation between factors and no-factor independence was confirmed. Therefore, principal factor analysis was performed with an oblique rotation (promax rotation). Three-factor solutions were adopted for the factors after considering the screen plot and eigenvalue. For each factor, items with factor loadings above 0.30 were selected. A subjective well-being scale, consisting of 3 factors and 10 items, was then developed (Table 2).The factor contribution of the three-factor solutions was 1.86 for the first factor, 1.68 for the second factor, and 1.45 for the third factor. Based on the characteristics of the questionnaire items that constituted each factor, the first factor was named “affect”; the second, “self-recognition”; and the third, “adaptation to life.” The Cronbach’s alpha coefficient was .62 for the first factor, .57 for the second, .52 for the third, and .71 for the overall scale.
3.3. The Relationship between the Scale, Sleep, Stress, and Satisfaction with Life
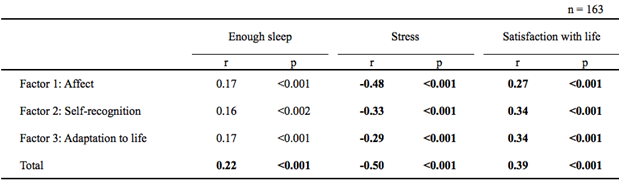
- The correlation coefficient between total scale score and sleep patterns was r = .17 (p = .001) for the first factor, r = .16 (p = .002) for the second, r = .17 (p = .001) for the third, and r = .22 (p <.001) for the overall scale. The correlation coefficient between total scale score and stress level was r = -.48 (p < .001) for the first factor, r = -.33 (p < .001) for the second, r = -.29 (p < .001) for the third, and r = -.50 (p < .001) for the overall scale. Lastly, the correlation coefficient between the total scale score and satisfaction with life was r = .27 (p < .001) for the first factor, r = .34 (p < .001) for the second, r = -.34 (p < .001) for the third, and r = .39 (p < .001) for the overall scale (Table 3).
|
|
|
4. Discussion
4.1. The Factor Structure of the Scale
- The adolescent subjective well-being scale consisted of three factors: affect, self-recognition, and adaptation to life.Subjective well-being has been studied according to three dimensions: objective personal conditions, cognition, and emotion [12]. The combination of emotional happiness and cognitive satisfaction is termed “subjective well-being” [13]. Emotion and cognition are therefore major factors that constitute subjective well-being. This study comprises a three-factor structure of affect, self-recognition, and adaptation to life. “Adaptation to life” includes the concept of cognition. The three-factor structure developed in this study can thus be considered valid and constitutive of subjective well-being. In addition, the reliability coefficient of the overall scale was .71, and .62 for the first factor, .57 for the second, and .52 for the third, which confirmed the scale’s internal consistency reliability.
4.2. Validity of the Scale
- The Spearman’s rank correlation coefficient was calculated for the relationship between total scale score and sleep patterns, stress level, and satisfaction with life. A significant positive correlation was found between sleep patterns and total scale score. A significant negative correlation was observed between stress level, total scale score, and sub-scale score. In addition, there was a significant positive correlation between satisfaction with life, total scale score, and interpretation score. This confirmed the criterion-related validity of the scale.
4.3. Study Limitations and Possibilities
- This study examined the scale’s criterion-related validity by performing a correlation analysis between subjects’ scale scores and sleep patterns, stress levels, and satisfaction with life. Major factors for change in subjective well-being include logical and flexible cognition, problem-solving behavior, social interaction, self-realization objectives, and acceptance of oneself [14]. These factors are reportedly related to social interaction [15]. A relationship with social skills has also been reported [16]. In addition, it is necessary to determine the concurrent validity of the present scale by comparing scores with those of another well-accepted scale, such as the Brief Multidimensional Students’ Life Satisfaction Scale (BMSLSS) [17]. Further confirmatory results will lend credence to the scale’s validity.
5. Conclusions
- The adolescent subjective well-being scale is composed of three factors, including emotion and cognition, which have been repeatedly implicated in previous studies as major factors constituting subjective well-being. The scale’s reliability and validity have also been confirmed. Thus, the adolescent subjective well-being scale is a useful tool for measuring subjective well-being in young people.
ACKNOWLEDGEMENTS
- I would like to thank those who have helped with this study, including Professor Tadao Takayama from the International University of Kagoshima and the Head of Research Group on the Healthiest and Longest-Living Village in Japan, Mayor Tokio Kuno, and Deputy Mayor Takamiki Hattori. The study has been partly funded by the Grants-in-Aid for Scientific Research of the Ministry of Education, Culture, Sports, Science and Technology (Grant number: 23330174, 24653134).