-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Psychology and Behavioral Sciences
p-ISSN: 2163-1948 e-ISSN: 2163-1956
2014; 4(1): 21-29
doi:10.5923/j.ijpbs.20140401.04
Development of a Scale for Assessing the Childcare Information Utilisation Skills of Childcare Professionals (SACIUS)
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLWatanabe T1, Tanaka E2, Tomisaki E2, Mochizuki Y2, Tokutake K2, Wu B2, Matsumoto M2, Shiori A2, Anme T2
1Ashikaga Junior College, Ashikaga, 326-0808, Japan
2University of Tsukuba, Tsukuba, 305-8575, Japan
Correspondence to: Watanabe T, Ashikaga Junior College, Ashikaga, 326-0808, Japan.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
[Aim] Childcare professionals who work at childcare centres require the skills to maintain and improve the overall health of the children for whom they care. The purpose of this study was to develop a scale for assessing the childcare information utilisation skills (i.e. skills for utilizing information towards the betterment of the child) of childcare professionals, as well as confirm its reliability and validity. Furthermore, we intended this scale to be used in the ‘plan-do-check-act’ cycle of childcare professionals to maximise each child’s ability. [Methods] Item development was conducted through focus group interviews. Validity and reliability were assessed with a sample of 178 childcare professionals throughout Japan. Then, using factor analysis, the predicted 2-factor structure was obtained; the factor pattern was similar to a simple structure, thereby confirming the factorial validity. [Results] The first factor (12 items) consisted of the childcare professionals’ skills for assessing information, putting this assessment into practice, evaluating the practice, and then incorporating their evaluation into further practice to increase their knowledge and improve their skills; thus, the factor was called ‘advanced information utilisation skills’. The second factor (14 items) consisted of childcare professionals’ skills for collecting and understanding basic information; thus, we called it 'basic information utilisation'. The Cronbach’s alpha values were consistently high (first factor: α = 0.93; second factor: α = 0.90; whole scale: α = 0.94), thus confirming the internal consistency reliability of the scale. The results of correlational analysis of age, work experience, and Early Childhood Environment Rating confirmed the criterion validity; another correlational analysis with a measure of communicative and critical health literacy confirmed the construct validity. [Conclusion] The final scale consisted of 2 factors and 26 items. With the confirmation of the validity and reliability, we expect that this scale will contribute to improvements in the quality of childcare, as well as lead childcare professionals to acquire improved materials to be used in childcare.
Keywords: Childcare, Childcare Information Utilisation, Childcare Professional, Health Record, Care Coordination
Cite this paper: Watanabe T, Tanaka E, Tomisaki E, Mochizuki Y, Tokutake K, Wu B, Matsumoto M, Shiori A, Anme T, Development of a Scale for Assessing the Childcare Information Utilisation Skills of Childcare Professionals (SACIUS), International Journal of Psychology and Behavioral Sciences, Vol. 4 No. 1, 2014, pp. 21-29. doi: 10.5923/j.ijpbs.20140401.04.
Article Outline
1. Introduction
- In Japan, the total fertility rate peaked in 1971, and subsequently started a slow decline, reaching 1.26 by 2005. Since then, it has remained persistently low. In order to find a solution to this declining birth rate, the Japanese government has been attempting to develop a system and new guidelines for childcare centres that will help parents maintain a balance between work and childcare. This has led childcare centres to begin making efforts to cope with parents’ various forms of employment, such as extending their work hours and offering midnight or holiday childcare services, as well as accommodating children who are on their waiting lists[1]. The new guidelines in Japan for childcare centres emphasise the importance of evidence-based support and constant self-evaluation of services and personnel, in order to increase the quality of childcare[2]. According to the guidelines, this increase in quality would be the result of the plan-do-check-act cycle (PDCA cycle), a process whereby childcare professionals assess the various characteristics of the children they care for, put the results of this assessment into practice, evaluate the results of the practice, and then incorporate their evaluation into their subsequent practice, thereby improving their skills over time. However, currently there is no tool for assessing childcare professionals’ ability to provide such evidence-based support or engage in self-evaluation; thus, many professionals are struggling to learn about each child, and how to assess this information, put it into practice, and then evaluate this practice.We developed a cloud computing-based support system for comprehensive childcare. The validity of this system for use in the PDCA cycle has been confirmed[3]. Thus, one of the only tasks remaining to complete this system of evidenced-based child support and self-evaluation of childcare centres is to develop a tool that childcare professionals can use to self-monitor their performance.The purpose of this study was to develop a scale for assessing the childcare information utilisation skills of childcare professionals that can be used to quantitatively measure the effectiveness of the PDCA cycle; the scale would be essential for helping childcare professionals maintain and improve children’s health and maximise each child’s ability. Furthermore, we determined the reliability and validity of this scale by administering a questionnaire survey to childcare professionals throughout Japan.
2. Methods
2.1. Development of Scale Items
- Before we could implement the scale, we attempted to develop an item pool that would eventually constitute this scale for assessing the childcare information utilisation skills of childcare professionals. To create the item pool, we organised 4 focus group interviews consisting of 3 different groups of professionals: a group of childcare professionals, who are exposed daily to children at childcare centres; a group of public health nurses; and a group of developers who have experience in web-based utilisation systems, so that we could optimise childcare professionals’ ability to record and evaluate information about the children. Each group contained about 7 members, because this number is the maximum for ensuring effective group dynamics[4,5]. Data were obtained from 7 men and 19 women, totalling 26 people aged 25–60 years. Every interview lasted for about 1.5 h.We created 2 categories from the information extracted from the interviews: ‘basic information utilisation skills’ and ‘advanced information utilisation skills.’ This process of extraction and categorisation was conducted by 3 researchers and supervised by an expert of group interview methods, in order to ensure that important information was placed into the appropriate categories.In this study, we defined ‘information utilisation skills’ as skills that can be used in the PDCA cycle and are necessary for maintaining and improving each child’s overall well-being as well as maximising each child’s ability. As for the categories, ‘basic information utilisation skills’ are considered the skills used for collecting and understanding the basic information of childcare centre children that is required for further assessment. ‘Advanced information utilisation skills’, in contrast, are those skills used for assessing the basic information on childcare centre children, putting the results of this assessment into practice, evaluating the effects of the practice, and then incorporating the evaluation into subsequent, better practice. Thus, these skills correspond to the elements of the PDCA cycle.In developing a scale for assessing the information utilisation skills of childcare professionals, it would be necessary to have a suitable reference construct to ensure that the scale is suitably valid; thus, we employed the concept of ‘health literacy’. Health literacy is defined as ‘the cognitive and social skills which determine the motivation and ability of individuals to gain access to, understand and use information in ways which promote and maintain good health’[6] or ‘The wide range of skills and competencies that people develop over their lifetimes to seek out, comprehend, evaluate, and use health and information and concepts to make informed choices, reduce health risks, and increase quality of life’[7]. Although ‘health literacy’ and information utilisation skills differ in where the skills are directed, they are similar in how they both involve understanding the information required for maintaining or increasing health, as well as applying such information. We found that the skills of the ‘basic information utilisation skills’ category was similar to the concepts of ‘functional health literacy’ and ‘interactive health literacy,’ while ‘advanced information utilisation skills’ was similar to ‘critical health literacy’, according to Nutbeam’s use of the term ‘health literacy’[8,9]. Therefore, we consider that these 2 categories appropriately reflect information utilisation skills. Eighty items were categorised into ‘basic information utilisation skills’ and 36 items were categorised into ‘advanced information utilisation skills.’ Four researchers along with an epidemiologist, a professional in maternal and child health, and a childcare professional then conducted an item analysis, taking care so that the similar or exact phrases and words obtained in the focus group interviews were used. Furthermore, they closely examined the content of each item to ensure that there was no overlapping of meaning and that the wording was at the level of childcare professionals.The item analysis resulted in a total of 30 items, with 18 items categorised as ‘basic information utilisation skills’ and 12 items as ‘advanced information utilisation skills’.
2.2. Subjects and Research Period
- Subjects were 180 childcare professionals and kindergarten teachers working at approved childcare centres and kindergartens in various local communities across Japan. Each community had an average population composition. The research period was between August 1 and 31, 2012.
2.3. Procedure
- The research was performed via a self-administered questionnaire. Researchers visited childcare centres and kindergartens with written requests for participation and explanations of the present study; in addition, we verbally explained the purpose and method of this study, how the results and data would be used, and that refusing to participate would put them at no disadvantage. We also provided a means to contact us in the case of further inquiry. Questionnaire collection was entrusted to the persons in charge of the respective childcare centres and kindergartens, who then returned them to us. We made sure that each person who collected the questionnaires understood what was asked of them, to ensure that they understood how to treat the questionnaires.
2.4. Questionnaire Items
- The questionnaire consisted of questions on demographic information (age, sex, profession, work experience, title), the information utilisation scale items collected and constructed prior to beginning the study, and 2 additional scales to confirm the criterion and construct validities of the information utilisation scale: the Early Childhood Environment Rating Scale[10] and the Communicative and Critical Health Literacy Scale[11]. As mentioned previously, the information utilisation scale items consisted of 2 subscales and 30 items. Participants rated each item on a 5-point scale, ranging from 1 (‘I disagree completely’) to 5 (‘I agree completely’).The Early Childhood Environment Rating Scale was developed to help improve the professional skills of people employed in childcare. It includes a variety of elements that professionals must have to meet the various needs of children and parents, and ensure that they have the best interests of the child in mind. This scale was found to benefit children’s healthy growth in a previous study. This scale consists of 9 items that reflect understanding the child, 8 items for understanding the family, and 12 items for understanding the child’s association with related agencies, giving a total of 29 items. Answers are rated on a 5-point scale, ranging from 1 (‘This is not at all true for me’) to 5 (‘This is completely true for me’), with the total scale score being the sum of the scores of all subscales[10].The Communicative and Critical Health Literacy Scale was developed by referring to the WHO’s definition of ‘health literacy’, and it includes 3 items for assessing individual communicative health literacy and 3 items for measuring critical literacy, totalling 5 items. These items were rated on a 5-point scale, ranging from 1 (‘I disagree completely’) to 5 (‘I agree completely’)[11].
2.5. Statistical Analyses
- First, we made sure that we understood each variable and its distribution. Next, we confirmed that the information utilisation scale had 2 factors—‘basic information utilisation skills’ and ‘advanced information utilisation skills’— through a factor analysis, while considering the distribution of these scale items. When the 2-factor structure was confirmed, we determined Cronbach’s alpha coefficient to assess the internal consistency of the factor structure. Then, we verified the criterion-related validity (concurrent validity) by assessing the correlations of the scale items and age, work experience, and the scores on the Early Childhood Environment Rating Scale. Finally, construct validity was verified through correlation analysis with subjects’ scores from the Communicative and Critical Health Literacy Scale.
2.6. Ethical Considerations
- The submission of the questionnaire was taken as each subject’s consent to participate. In addition, a sealable envelope was prepared for each subject to ensure his or her privacy. Research was conducted only after the approval of the ethics committee of the Faculty of Medicine at Tsukuba University.
3. Results
3.1. Subject Characteristics
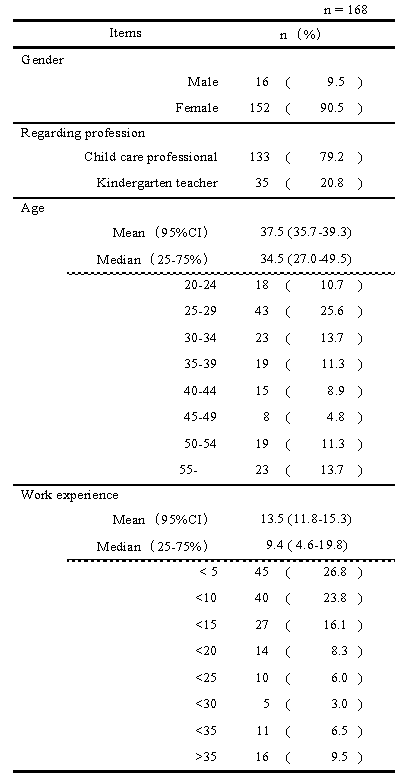
- Questionnaires were distributed to 180 subjects, of which 178 answered (return rate: 98.9%). Of these 178 answers, 168 were completed correctly, having no incomplete answers or omissions, and thus were used in the analyses (Table 1).
|
3.2. Results of Factor Analyses
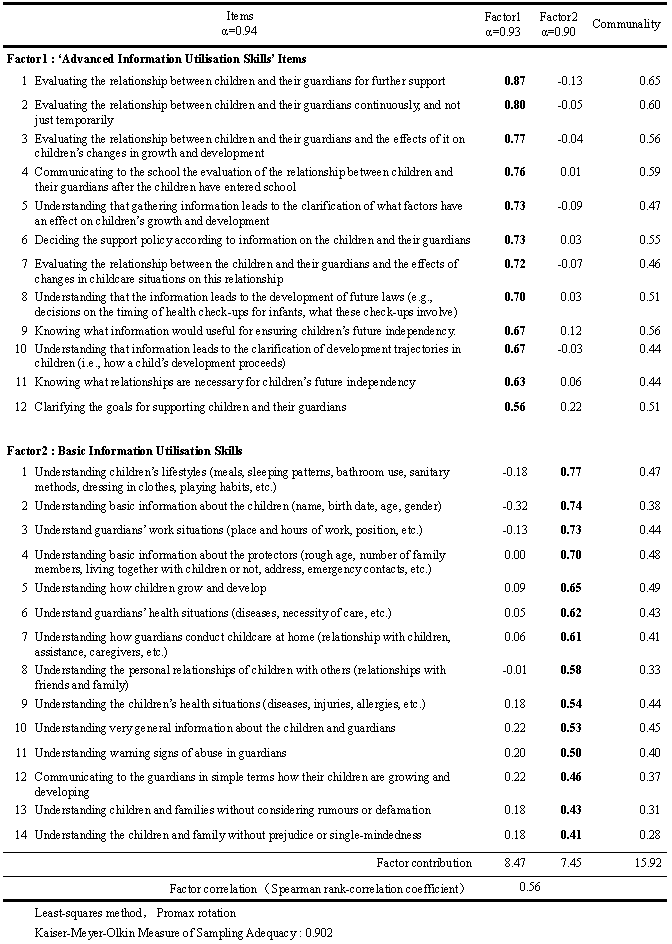
- For the 30 items of scale for assessing the childcare information utilisation skills, we confirmed the distribution for each item; however, a multivariate normal distribution was not obtained. There was a correlation between the factors, but they were not found to be independent. Therefore, we conducted a factor analysis by the least-squares method with an oblique (Promax) rotation. As for the factor number, in addition to the initial hypothesis, we considered a scree plot and eigenvalues, and 2 factors were revealed. For each factor, items with factor loadings of 0.4 and greater were adopted, and items showing overlapping factor loadings for both factors were excluded. Thus, 2 factors and 26 items were adopted (Table 2).
|
3.3. Coefficient of Reliability
- The Cronbach’s α coefficients were as follows: 0.94 for the whole scale, 0.93 for the first factor, and 0.90 for the second factor. Thus, the scale showed high internal consistency.
3.4. Correlations with Age and Work Experience
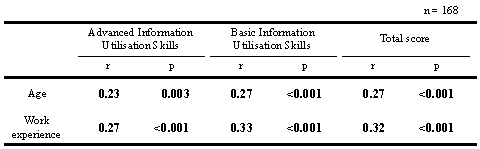
- Spearman’s rank correlation coefficients were calculated between age, work experience, and each item score on the scale for assessing information utilisation skills (Table 3). The correlations with age ranged from r = 0.23–0.27 (p < .001) and the correlations with work experience ranged from r = 0.27–0.33 (p < .001).
|
3.5. Correlations with the Early Childhood Environment Rating Scale
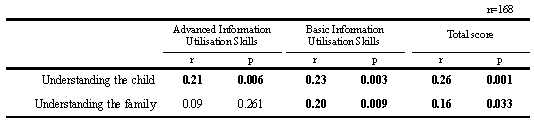
- Spearman’s rank correlation coefficients were calculated for each factor score of the scale and the subscales of the Early Childhood Environment Rating Scale (Table 4). The correlation of the subscale, ‘understanding the child’ with ‘advanced information utilisation skills’ was r = 0.21 (p = .006), that with ‘basic information utilisation skills’ was r = 0.23 (p = .003), and that with the total score of the information utilisation scale was r = 0.26 (p = .001). The correlations between the subscale, ‘understanding the family’ and ‘advanced information utilisation skills’, ‘basic information utilisation skills’, and the total score were r = 0.09 (p = .261), r = 0.20 (p = .009), and r = 0.16 (p = .033), respectively.
|
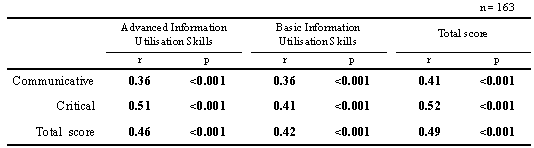
3.6. Correlations with the Communicative and Critical Health Literacy Scale
- Spearman’s rank correlation coefficients were calculated for each subscale score on the Communicative and Critical Health Literacy Scale and both factor scores and the total score of the information utilisation scale (Table 5). The correlations between communicative health literacy and ‘advanced information utilisation skills’, ‘basic information utilisations skills’, and the total score were r = 0.36 (p < .001), r = 0.36 (p < .001), and r = 0.41 (p < .001), respectively. The correlations between critical health literacy and ‘advanced information utilisation skills’, ‘basic information utilisation skills’, and the total score were r = 0.51 (p < .001), r = 0.41 (p < .001), and r = 0.52 (p < .001), respectively. Finally, the correlations between the total score on Communicative and Critical Health Literacy Scale and the ‘advanced information utilisation skills’, ‘basic information utilisation skills’, and total score of the information utilisation scale were r = 0.46 (p < .001), r = 0.42 (p < .001) and r = 0.49 (p < .001), respectively.
|
4. Discussion
4.1. Factor Structure of the Scale
- In this study, we aimed to construct a scale for appropriately assessing the information utilisation skills of childcare professionals. In our assessment of the validity and reliability of the scale, we also sought to confirm its hypothesised 2-factor structure—‘basic information skills’ and ‘advanced information utilisation skills’—by conducting a pilot study on childcare professionals and kindergarten teachers. The factor analysis revealed the predicted 2-factor structure, with a factor pattern near to a simple structure, giving it high factorial validity. Furthermore, the Cronbach’s alpha coefficients for the factors and whole scale were nearly 1, thus confirming its good internal consistency. As predicted, the 12 items in the ‘advanced information utilisation skills’ factor consisted of skills for assessing the information of childcare centre children, putting the results of that assessment into practice, evaluating the results of the practice, and then incorporating the evaluation into subsequent, thereby improved, practice. Furthermore, the 14 items of the ‘basic information utilisation skills’ factor corresponded to the skills used for collecting and understanding information of childcare centre children.
4.2. Scale Validity
- We found significant positive correlations between age, work experience, and the subscales of the Early Childhood Environment Rating Scale and the factors of the information utilisation scale. Because age, work experience, and the Early Childhood Environment Rating Scale are considered to help improve professionals’ skills in childcare, the criterion validity (concurrent validity) was confirmed. High quality childcare is considered to consist of ample knowledge and appropriate methods, also called ‘experience-based skills’ and ‘scientific skills’[10]. Experience-based skills are learned with both increasing age and work experience. Therefore, work experience should be considered as one of the elements that help improve expertise. Furthermore, the Early Childhood Environment Rating Scale was originally developed to aid professionals in improving their professional skills by striving to identify and meet the needs of each child; furthermore, there is already evidence that this scale has a beneficial effect on children’s healthy growth. Thus, the high correlations between its subscales and the factors of scale for assessing the childcare information utilisation skills suggests that our newly developed scale will allow for appropriate assessment of childcare professionals’ skills and how they improve.Furthermore, the construct validity was confirmed, as shown by the results of the correlational analysis with the Communicative and Critical Health Literacy Scale: significant positive correlations were found between the factors and total score of the information utilisation scale and all subscales of the health literacy scale. The communicative subscale of the health literacy scale showed a higher correlation with the ‘basic information utilisation skills’ factor, while the critical subscale showed a higher correlation with the ‘advanced information utilisations skills’ factor. Because both the criterion and concurrent validity were confirmed, we determined that the scale could be used to appropriately measure childcare professionals’ information utilisation skills.
4.3. Contribution of the Scale to Improving the Quality of Childcare
- Many studies have been conducted on the effects of childcare outside of the home on the development and adaptive functioning of children. Bradley and Vandell[12], in a review of 106 studies on the effects of childcare (including age of entrance, the number of hours of care, and the methods and quality of childcare) on the development of children (social, physical, and cognitive), reported, ‘Childcare is a multidimensional phenomenon. Guidance on when to place a child in non-parental care and what kind of care to use is complicated … and research indicates that the quality of childcare matters’. ‘The most important are the quality of childcare and the human interaction full of responsiveness and sensitiveness, in personal relationship’. Afterwards, a cohort study reported, ‘Results showed that children who experienced higher quality childcare consistently showed somewhat better cognitive function and language development... Higher quality childcare also predicted greater school readiness...’[13].In addition, it has been reported that the quality of childcare in infancy has an effect on children’s later emotional stability, and problems in early childcare may result in the development of problematic behaviours and somatic symptoms in adolescence[14]. However, high quality childcare, even when the child comes from a bad home environment (including abusive homes), can make children develop more secure attachments[15].Thus, although many studies have indicated the importance of high-quality childcare, they have varied in how they evaluate this quality. Furthermore, although it has been said that quality childcare has at its core highly aware and skilled childcare professionals[16], before this study, there has been no such tool to quantitatively measure the skills of childcare professionals. Therefore, the scale developed herein can be utilised to help childcare professionals self-monitor, reflect on their knowledge and skills, and find points for improvement, eventually leading to their comprehension of all aspects of quality care. We hope that this scale will further improve the quality of childcare and help childcare professionals develop high-quality methods of care.
4.4. Limitations
- Although both the criterion and construct validity were confirmed, to obtain stronger validity, we require further verification in terms of the relationships of the skills that the scale reflects and the cognitive and language development and readiness of children for school, which have causal relationships with the quality of childcare[13].
5. Conclusions
- In the present study, we developed a scale for assessing the information utilisation skills of childcare professionals, consisting of 2 factors and 26 items. The scale was developed to properly measure the information utilisation skills used in the PDCA cycle, which childcare professionals require to maintain and improve children’s health and maximise each child’s ability. A factor analysis revealed factorial patterns near to a simple structure, thus confirming the factorial validity; furthermore, the internal consistency of the scale was high. The scale was found to be highly valid: the result of correlational analyses with age, work experience, and the Early Childhood Environment Rating Scale confirmed the criterion validity, while the correlational analysis with the Communicative and Critical Health Literacy confirmed the construct validity. We expect the scale to be useful in improving the quality of childcare, as well as the skills of those professionals working in this field.
ACKNOWLEDGEMENTS
- We are deeply grateful to Mr Kaoru Amahisa and Mr Shinichiro Edamoto, the president and the vice president, respectively, of the Japan Night Childcare Association, and the members of the Society of Childcare Improvement Studies, as well as all of the other people who have cooperated with us.This study was a part of the results of the ‘Implementation of a Web-based General Support System for Kindergarten Children’ (an implementation-support program of the Research Institute of Science and Technology at the Japan Science and Technology Agency) and the ‘Development and Research of a Program for Early Support of Children of Concern based on Mass Cohort Research (Work Number 2330174)’ (supported by a Grant-in-Aid for Scientific Research by the Ministry of Education, Culture, Sports, Science and Technology).