-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Psychology and Behavioral Sciences
p-ISSN: 2163-1948 e-ISSN: 2163-1956
2013; 3(6): 151-156
doi:10.5923/j.ijpbs.20130306.02
Comparative Study of Illness Perception among Hypertensive Patients in India
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAarti Nagarkar, Swapnil Gadhave, Pooja Gund, Ishor Sharma, Ankita Choure
Interdisciplinary School of Health Sciences, University of Pune, Pune, 411016,India
Correspondence to: Aarti Nagarkar, Interdisciplinary School of Health Sciences, University of Pune, Pune, 411016,India.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
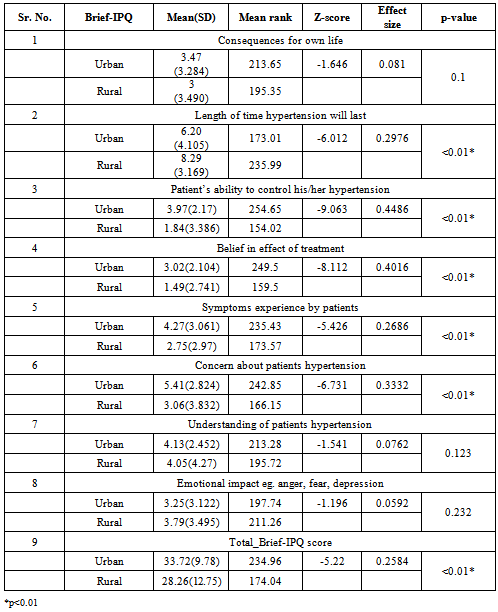
Hypertension is a chronic condition and a major risk factor for cardio vascular disease. Prevalence of hypertension is increasing exponentially in India. Knowledge about patient’s perception would provide better understanding of the factors influencing the patient’s acceptance of illness and coping behaviour. The aim of the study was to translate and validate brief illness perception questionnaire and to determine differences in illness perception among rural and urban hypertensive patients. Cross sectional study 408 hypertensive patients from urban and rural area who attended the clinics during study period were recruited to compare illness perception between rural and urban hypertensive patients. Translated and validated Brief-Illness Perception Questionnaire (Brief-IPQ) was used. Internal consistency of the Marathi version was moderate (Cronbach alpha 0.340). The item to total correlation coefficient ranged from -0.415 to 0.475. Comparative study between urban and rural respondents suggested higher threatening perception among urban than rural hypertensive patients (Mann –Whitney U test Z score = -5.220; p-value < 0.01). Urban hypertensive patients frequently experienced symptoms, more concerned, considered having personal control over their illness and thought their antihypertensive medication was more helpful in controlling their illness than rural hypertensive patients.
Keywords: Hypertension, Illness Perception, Brief-IPQ, India
Cite this paper: Aarti Nagarkar, Swapnil Gadhave, Pooja Gund, Ishor Sharma, Ankita Choure, Comparative Study of Illness Perception among Hypertensive Patients in India, International Journal of Psychology and Behavioral Sciences, Vol. 3 No. 6, 2013, pp. 151-156. doi: 10.5923/j.ijpbs.20130306.02.
Article Outline
1. Introduction
- Hypertension currently affects almost 1 billion people worldwide, this number is expected to grow to 1.6 billion by 2025[1,2]. Prevalence of hypertension is increasing exponentially in India, too[3]. Reported prevalence of hypertension is 164.18 per thousand in urban India.[4] Hypertension is a chronic condition and a major risk factor for cardio vascular disease. Control and treatment of this chronic condition can lead to prevent more than 300,000 of the 1.5 million annual deaths from cardiovascular diseases in India[3].Research dealing with chronic illnesses has reported that the patients’ perception of the illness influence different aspects of their experience including adherence to the advice, health seeking behaviour and ways to cope with the illness[5,6,7]. An insight into patients lay beliefs about their illness can be a major factor in combating chronic illnesses like hypertension, diabetes[8,7]. Knowledge about patient’s perception would provide better understanding of the factors influencing the patient’s acceptance of illness and coping behaviour[9]. Leventhal and colleagues (1997) have suggested a ‘Self-regulatory model’ which is helpful in understanding how patients organize their behaviour and emotional reactions to illness.[1]. Several validated instruments based on Leventhal’s theory are available to study illness perception [11,12,13] and have proved useful in improving health of patients and their recovery[14]. Health promotion interventions based on illness perception would prove beneficial for improving public health. This study was undertaken with following objectives: a] to translate and validate brief illness perception questionnaire b] to understand illness perception among hypertensive patients using brief illness perception questionnaire and c] to determine differences in illness perception among rural and urban hypertensive patients.
2. Materials and Methods
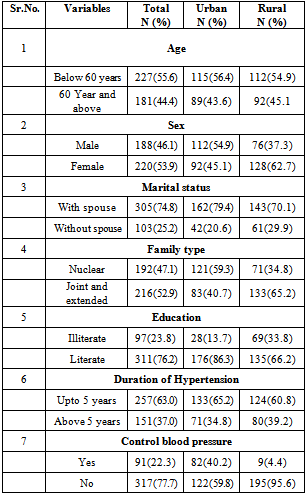
- Study was carried out at two places. Urban sample was collected by recruiting patients attending outpatient department of a Municipal cooperation’s tertiary hospital in the city of Pune. Pune is located in the western part of the state of Maharashtra, India. Rural patients were recruited from the field practice area named Khadkala primary health centre and all private clinics in the area. This primary health centre caters to the population of 47,000 and is located 55 kilometers from the city of Pune. Time space sampling method was used in the recruitment of the patients in the study. Patients already diagnosed with hypertension and visiting the clinics for routine check up for hypertension or for collection of medicine from the drug store located in the hospital were recruited during six days a week in the morning and afternoon session of the outpatient department of District hospital in city and Primary health center in rural area. Total 408 hypertensive patients; 204 from urban and 204 from rural hypertensive patients who attended the clinics during study period (Nov 2011 to March 2012) were included in the final analysis of the main study. Tools/Measures: Pretested semi-structured interview schedule was administered which includes questions on social and economic characteristic, illness history and Marathi version of Brief Illness Perception Questionnaire (Brief-IPQ) developed by Broadbent and colleagues[12]. illness representations like (i) Identity- How much do you experience symptoms from your illness?(ii) Consequences- How much does your illness affect your life? (iii) Concern- How concerned are you about your illness?(iv) Timeline- How long do you think your illness will continue?(v) Coherence- How well do you feel you understand your illness? (In the text used as understanding)(vi) personal control-How much control do you feel you have over your illness? (vii) Treatment control- How much do you think your treatment can help your illness? (viii) Emotional response- How much does your illness affect you emotionally? (e.g. does it make you angry, scared, upset or depressed?). The total scaling is based on 8 items. The ninth question is open ended question about perceived cause of illness. Responses are recorded on 11 point Likert scale, separately for each item, participants are asked to choose one number which describes their answer on the scale of 0 to 10. To compute total Brief-IPQ scores for item Personal (Q3) control, Treatment control(Q4) and coherence(Q7) were reversed and added. Higher score for total Brief-IPQ reflects more threatening perception about illness. Translated version of Marathi Brief-IPQ was semantically and conceptually close to the original questionnaire. Translation was done by two independent translators; both were native speaker of Marathi and also spoke English language. They reviewed the first and second forward translation and prepared reconciled forward translation. The third person who was also a native Marathi speaker reviewed reconciled version and translated back in English. Thus translated version was compared with original and accepted after minor changes. Study is approved by Pune University’s ethics committee.Data Analysis: Validation of Marathi Brief-IPQ was undertaken using methods used by Broadbent and colleagues (2006) for validation of the original Brief-IPQ[12]. 1) The Pearson’s correlation coefficient between the scores used for test-retest reliability analysis. Forty hypertensive patients were contacted again for test-retest reliability exercise. 2) Discriminant validity analysis was carried out using ANOVA test with least significant difference (LSD) post hoc test. For the discriminant validation of scale an additional sample of 70 already diagnosed diabetes patients and 50 acute respiratory tract infections patients attending the same clinics were interviewed using the same questionnaire. Descriptive statistics and non parametric tests were used for the analysis because they did not qualify for the parametric tests as all major variables showed non normal distribution. Mann Whitney-U test was conducted to check the difference between the total score and individual score for different dimensions of the Brief-IPQ. Data analysis was carried out using SPSS version 19.
3. Results
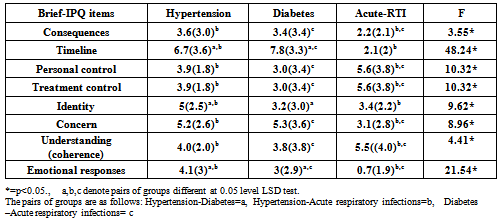
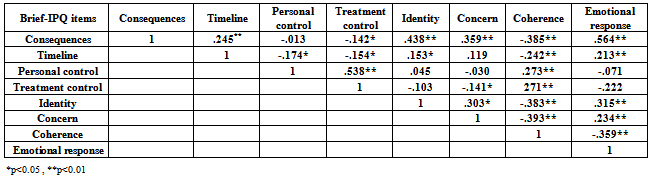
- Results of objective one are described initially. The Brief-IPQ was translated in Marathi using rigorous protocol as described above. Internal consistency of the Marathi version was moderate (Cronbach alpha 0.340). The Cronbach alpha value increased to 0.668 when timeline, treatment control items were deleted. The item to total correlation coefficient ranged from -0.415 to 0.475. Pearson correlation demonstrated that the Brief-IPQ items except timeline (Pearson’s correlation coefficient (r) (r = 0.014) and treatment control (r =0.072) have modest test-retest reliability. Pearson’s correlation coefficient ranged from 0.328 to 0.574 for remaining items on the scale.To establish discriminant validity of the scale (Table-1), difference between total Brief-IPQ mean scores for hypertension, diabetes and acute respiratory infections, were computed using series of one-way ANOVA with LSD post hoc test.The scores differ significantly from each other at p<0.05 level. The mean difference between hypertension and diabetes (4.27, P< 0.05) as well as acute respiratory infection (9.36, P < 0.01) was significant. Difference between acute respiratory infection and diabetes was 5.09, P < 0.01.
|
|
|
|
4. Discussion
- The Brief-IPQ was translated in Marathi for quick and easy assessment of illness perception of the hypertensive patients in Maharashtra. The Cronbach alpha value for Marathi translation was low. There are three possible explanations; Cronbach alpha decreases with reduced length of scale, merely eight item used for scaling[15]. Secondly, being multi dimensional scale; each item in the scale characterizes a single component of illness representations. Hence usually Cronbach alpha value is lower than expected cut off[16]. Thirdly, could be limited sample size, high sample size yields high Cronbach value[17]. Test retest reliability scores were comparable with other studies describing properties of the translated versions of Brief-IPQ [11,12]. The ninth item was an open ended question to which around 25% of respondents were unable to respond as it asked for causes of the illness. This is suggestive of gaps in the patient’s understanding of illness and awareness about the illness[17]. Discriminant validity analysis of the scale showed significant differences among the mean scores of Marathi Brief-IPQ. This indicates ability of the scale to distinguish between chronic illnesses as well as between chronic and acute illness. The results are in line with Broadbent and colleagues[12] work. Timeline and concern scores were elevated for hypertension and diabetes signifying their chronic nature and severe outcomes as compared to acute respiratory infections. Treatment control and personal control scores were high in the acute respiratory infection patients compared to diabetes and hypertension as they believed their illness to be short term and curable with treatment. We have used Brief-IPQ to show differences in the perceptions of two different groups and have used this in an outpatient set up. A study on musculoskeletal diseases has used this scale successfully to show difference in two groups[18]. Brief-IPQ has been used among outpatient set up in general hospital in China[19] as well as in, Bangalore, India[20], effectively.Illness perception, as assessed with the Brief IPQ questionnaire, was the ability of patients to see their illness i.e. hypertension as a chronic disease that can be well-controlled under appropriate treatment. Neither urban nor rural patients understood the nature of their condition. Total score reflects poor understanding of the condition. We did not come across any study among Indian hypertensive patients using Brief-IPQ but we compared our results with studies using the same scale for other illnesses. Our total and items scores are very less as compared to scores shown in a study on type 2 diabetes patients [8, 21] but one similarity with urban patient’s findings where they found that greater concern about the disease was associated with increased number of symptoms. Brief-IPQ scores of urban hypertensive patients suggest that they experienced more number of symptoms, thought they have greater ability to control their hypertension, and also believed in the effect of treatment. Symptoms recognition was more among urban patients perhaps because of higher literacy in urban (86%) than rural (66%). Erkoc and colleagues (2012) [22] found significant relationship between patient’s education level and knowledge about hypertension. As opposed to this rural patients experienced less symptoms, were less concerned about hypertension as a disease. They perceived they have less personal and treatment control. Ross and colleagues (2004)[23] suggest that emotional response to illness and belief in personal ability to control illness have indirect impact on medication adherence. Lack of personal control among rural patients may have serious implications on treatment adherence and control of hypertension. A recent review paper suggests that the awareness of hypertension in India is very low with suboptimal control rates[24]. We have not used the results of blood pressure measurements in this paper. However, it is worth mentioning here that the blood pressure control was found much high (40%) among urban than rural (4.4%) participants. Strengths and limitations of the study: The major strength of this study is that our findings are based on patients from urban and rural areas from outpatient setting rather than researchers identifying them as hypertensive. Patients were diagnosed with hypertension in general practice and participants were recruited by their own treating physician. It therefore seems likely that the patterns found in this study are generally representative for primary care patients with hypertension. Additional strengths derive from the use of a validated questionnaire and an acceptable reliability of the questionnaire when adapted in local language. One of the limitations of the study is possible selection bias due to selection of sample from outpatient departments. However we tried to avoid bias by selecting patients on all working days and at different timings. One more limitation of the study may be the relatively small number of participants, resulting in a statistical power that may not have been sufficient to detect very small differences in illness perception scores among patient groups. Nevertheless, we were able to detect significant differences in urban and rural patients understanding of the disease.
5. Conclusions
- The simplicity of scale makes it easy to understand and administer effectively in crowded settings however cultural adaptation and contextual changes may be considered when translated in any other language. It is useful in comparative studies. Studies which aim to change illness behaviour will benefit by use of illness perception questionnaire.
ACKNOWLEDGEMENTS
- We thank Dr Elizabeth Broadbent for granting permission to use the Brief illness perception questionnaire and translate it in Marathi. We are thankful to the Indian Council of Medical Research, New Delhi for supporting this research.