-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Psychology and Behavioral Sciences
p-ISSN: 2163-1948 e-ISSN: 2163-1956
2013; 3(1): 34-39
doi:10.5923/j.ijpbs.20130301.05
Impact of Socio- demographic Factors on Child Mortality in Bangladesh: An Multivariate Approach
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRafiqul Islam 1, Moazzem Hossain 2, Mizanur Rahman 1, Mosharaf Hossain 3
1Department of Population Science and HRD University of Rajshahi, Rajshahi, 6205 Bangladesh
2Research fellow Dept. of Population Science and HRD University of Rajshahi Bangladesh
3Research Fellow Departments of Population Science & HRD University of Rajshahi Rajshahi, 6205, Bangladesh
Correspondence to: Rafiqul Islam , Department of Population Science and HRD University of Rajshahi, Rajshahi, 6205 Bangladesh.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Child is the asset of a country. Child mortality is a powerful indicator to determine overall health situation in a country. It is one of the most important issues in developing countries. In Bangladesh, it is related to various social, demographic and environmental factors. Moreover, child mortality is linked to fertility. The main purpose of this study is to determine the factors related to child mortality in Bangladesh. In this study, data is used from Bangladesh Demographic and Health Survey (BDHS) 2007. In this paper, percentage distribution and logistic regression model have been used to determine which factors affect child mortality. It is indicated that mother’s education, wealth index, breastfeeding status, birth order, preceding birth interval and watch TV have effect on child mortality. The logistic model reveals that the mortality risk is 0.681 times lower for preceding birth interval 24 months and above than the preceding birth interval below 24 months. The risk of child mortality is 1.43 times higher for birth order 2-3 and 1.633 times higher for birth order 4+ as compared with single birth order. The risk of child mortality is found 0.958 times and 0.941 times lower for the children whose father’s having secondary and higher education as compared to the children of father’s having primary education. As compared with illiterate mothers the risk of mortality is 0.584 times, 0.341 times and 0.165 times lower for mothers who have had primary, secondary and higher education respectively. The risk of child mortality is found 0.958 times and 0.941 times lower for the children whose father’s having secondary and higher education as compared to the children of father’s having primary education. The risk of mortality is 0.850 times less for the children whose mother watching TV regularly than the children whose mother does not watch TV. The risk child mortality was found 0.017 times lower for the children whose mother currently breastfeeding to their children as compared to the children whose mother’s were not currently breastfeeding their children. Breastfeeding plays an important role in the growth, development and survival status of infant and child. So, it is concluded that mother’s education, breastfeeding status, wealth index, watch TV and birth order should be increased for reducing child mortality in Bangladesh.
Keywords: Child Mortality, Socio-economic Characteristics, Percentage Distribution, Logistic Model, Bangladesh
Cite this paper: Rafiqul Islam , Moazzem Hossain , Mizanur Rahman , Mosharaf Hossain , Impact of Socio- demographic Factors on Child Mortality in Bangladesh: An Multivariate Approach, International Journal of Psychology and Behavioral Sciences, Vol. 3 No. 1, 2013, pp. 34-39. doi: 10.5923/j.ijpbs.20130301.05.
Article Outline
1. Introduction
- Bangladesh is poor country and its most of the peoples are still illiterate. Maternal and child health care facilities are not enough free cost till now. So, it has been facing many problems. Now-a-days, child mortality is one of the burning questions[1]. Child mortality is defined as the probability of dying between the first and the fifth birthday[2]. Child mortality is determined by enormous number of complex and interrelated factors[3]. Five factors can directly influence child mortality: maternal factors (e.g. age, parity), environmental contamination (e.g. food, water), nutrient deficiency (e.g. calories), injuries (accidental or intentional) and personal illness control (e.g. personal preventive measures)[4].Maternal education was observed strong predictor of child mortality in developing countries[5-11]. The education of mother’s is emerged as one of the strongest predictors of child mortality through other factors like women’s autonomy, income, working status of parents, standard of living, household size, place of residence, better condition of water supply and sanitation have influence upon it[12-14]. Mother’s education attributed to the children of enjoying better diets and better overall care than the children of non-educated mothers[15] and there were strong inverse relationship between mother’s education and child mortality[16-17]. Mother education had a strong influence on child survival in Bangladesh than that of father’s education[18]. The child mortality causes the cessation of breastfeeding, thus increasing the probability of return to ovulation, so also the conception of the next child, resulting in a short birth interval. The strength of this effect was found to be related to the intensity, frequency and duration of breastfeeding[19]. Birth interval played significant role on infant and child mortality[20-22] and if the length of birth interval is short then the probability of dying is very high. In developing countries, children are much more likely to die if they are born less than two years after the mother’s previous birth than their birth interval is longer[20]. The higher mortality rates in rural area compared to urban area of developing countries have attributed to the greater availability of health care services, higher income and educational level in urban areas. In rural area of Bangladesh, the under five mortality occurred for most significant causes such as diarrhea and dysentery, tetanus, fever, respiratory and dropsy[23]. The health care services including higher coverage with immunization, safe delivery of birth is more developed in urban area than rural area in Bangladesh[24-25]. So, the main aim of this study is to find the impact of different socio-economic and demographic factors on child mortality in Bangladesh.
2. Sources of Data
- The total sample used in the current study consisted of 10996 Bangladeshi female married populations in age group 10-49 years. The data is taken from Bangladesh Demographic and Health Survey (BDHS)-2007 collected from the various districts of Bangladesh using multistage cluster sampling technique.
3. Methodology
- Cox discovered the logistic regression model that can be used not only to identify risk factors but also to predict the probability of success[26]. Furthermore, Lee and Fox developed this model[27-28]. This model expresses a qualitative dependent variable as a function of several explanatory variables, both qualitative and quantitative. Logistic regression is a form of regression, which is used when the dependent is a dichotomy and the independents are categorical. In logistic analysis, child mortality is treated as dependent variable and it is classified in the following way:
 Mother age at birth, sex of child, breastfeeding status, birth order, preceding birth interval, mother’s and father’s education, wealth index and watch TV are considered as explanatory variables in this model.
Mother age at birth, sex of child, breastfeeding status, birth order, preceding birth interval, mother’s and father’s education, wealth index and watch TV are considered as explanatory variables in this model.4. Results
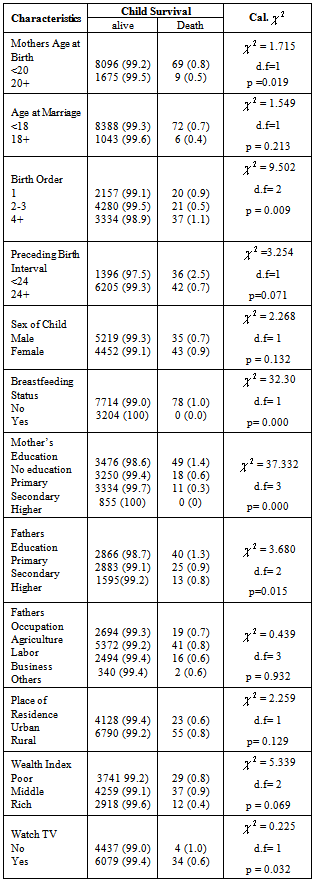
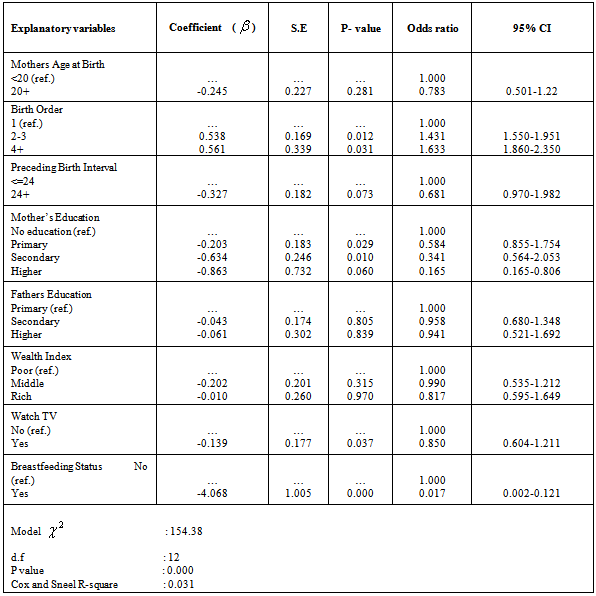
- Distribution of Child MortalityThe distributions of child mortality by demographic and socio-economic variables are shown in Table 1. From Table 1 it is noticed that mother’s age at birth, birth order, preceding birth interval, mother’s and father’s education, wealth index and watch TV has strong association with child mortality. Mother’s age at birth at the time of delivery is an important factor for child survival. Table 1 indicates that the proportion of child mortality is 0.8% for the children whose mother’s age at birth is below 20 years and 0.5% for the children whose mother’s age at birth is 20 years and above.Age at marriage shows insignificant relationship with child mortality. Highest proportion of child death (0.7%) is occurs whose mother’s age at marriage bellow 18 years but for marriage group 18 years and above this proportion is (0.4%). Birth order plays a vital role on child mortality. A significant proportion of child mortality is 0.9% and 0.5% occurs whose mothers had given single birth and 2-3 children, followed by 1.1% child death whose mothers had given birth more than 4 children. Hence it can be said that multiple birth is many time higher child mortality than single birth. Babies of multiple births usually become physically weak when their born. A strong significant relationship was found between child mortality and preceding birth interval. The child mortality is found to be high (2.5%) for the mothers having interval between last and previous child below 24 months, while it is lower (0.7%) for the mothers having interval between last and previous child 24 months and above. Breastfeeding status was associated significantly with child mortality. The proportion of children death whose mother never practiced breastfeeding is 1.0% and no percentage is found whose mother ever breastfeed their children. Among socio-economic variables maternal education has a strong relationship with child mortality and child survival. The child mortality is highest 1.4% for the children of illiterate mothers, 0.6% for primary educated mothers, 0.3% for secondary educated mothers and no parentage is found for the children whose mothers are higher educated. Thus it is clear that the child mortality decreases with increase of mother’s education. Like mother’s education & father’s education also plays significant role on child mortality. Father’s level of education has been regarded as a valid proxy income and wealth status of the household in Bangladesh. Highest number of children deaths (1.3%) is observed for the father having primary level education and the lowest number death (0.8%) is observed for the fathers who have had higher education. Child mortality is sharply decreases as the father’s educational level increases. In rural area child mortality is higher (0.8%) than urban areas (0.6%). Because of the people urban areas are more conscious about their child health and they get better medical facilities than rural areas. Lack of such facilities in the rural areas more causes higher child mortality.Wealth index is another important differentials factor of child mortality. The highest mortality is observed (0.9%) for the children whose mothers belonging to middle class families and the lowest proportion is (0.4%) child mortality is found among the children whose mother belonging to rich families. It is clear that the relation between wealth index and child mortality is negative. Watch TV also carry significant association with child mortality. The highest (1.0%) child mortality is observed whose mother does not watch TV and about 0.6% child death is observed whose mother watching TV regularly.Determinants of Child MortalityThe results of logistic regression analysis are shown in Table 2 in which it is observed that all the explanatory variables have significant effect on child mortality excepting mother’s age at birth, father’s education and wealth index. Mother’s age at birth plays an important role in child mortality though it does not show significant effect on child mortality. The study shows that the relative risk of child mortality is 0.783 times lower for younger age group (<20 years) mother as compared with the age group 20 years and above. Birth order shows strong relationship with child mortality risk. The risk of child mortality is 1.43 times higher for birth order 2-3 and 1.633 times higher for birth order 4+ as compared with single birth order. Preceding birth interval has significant association with child mortality. The model revealed that the mortality risk is 0.681 times lower for preceding birth interval 24 months and above than the preceding birth interval below 24 months. In this study, it has significant association with child mortality. As compared with illiterate mothers the risk of mortality is 0.584 times, 0.341 times and 1.65 times lower for mothers who have had primary, secondary and higher education respectively. Father’s education is the most important factor affecting child mortality but in this study father’s education is found insignificant on child mortality. The risk of child mortality is found 0.958 times and 0.941 times lower for the children whose father’s having secondary and higher education as compared to the children of father’s having primary education. These result clearly indicated that the risk of child mortality is decreasing with increasing father’s education. Wealth index of respondent is another important differential factor of child mortality though it does not show significant impact on child mortality. The relative mortality risk of children is 0.990 times and 0.817 times lower for the children those are belonging to middle and rich class families as compared to the children belonging to poor families. This may be due to fact that children of middle and rich families are provided better advantage (food, nutrition and health care facilities) whereas the child of poor families does not get proper nutrition and health care facilities. Watching television has constituent role in building health consciousness and in reduction of child mortality but it has no significant effect on child mortality. The risk of mortality is 0.850 times less for the children whose mother watching TV regularly than the children whose mother does not watch TV. Breastfeeding status of children has strong significant influence on child mortality. The risk child mortality was found 0.017 times lower for the children whose mother currently breastfeeding to their children as compared to the children whose mother’s were not currently breastfeeding their children. Breastfeeding plays an important role in the growth, development and survival status of infant and child.
|
|
5. Discussion and Conclusions
- By running logistic analysis, it is investigated that mother’s education, wealth index, breastfeeding status, birth order, preceding birth interval and watch TV have significant on child mortality. The study confirmed that child death is higher among the poor children as compared to rich children. The children of poorest families suffered more in diseases than the children of rich families. Income inequality is significantly visible in both leading causes of child mortality[29]. Poor quality of care, misperceptions regarding need for care, and other social barriers underlie the low level of care-seeking for illnesses of the newborns and children in Bangladesh. There is, however, evidence that, with appropriate training and sustained support, the quality of care from the government first-level facilities can be substantially improved[30]. Multiple births are associated with higher child mortality rate owing to higher risk of pregnancy and delivery complications, greater probability of birth defects and complication, higher risk of infection and lack of access to both basic and adequate health care. Results of this study show that child mortality remains unacceptably high in Bangladesh and that child born multiple births are at a much greater risk of dying in infancy than children born singletons. Children born multiple births are more than two times as likely to die during the first year of life as children born singletons, birth interval, pregnancy care and delivery care, maternal education and nutritional status, household access to clean water and sanitation, and other factors[31].The logistic model reveals that the mortality risk is 0.681 times lower for preceding birth interval 24 months and above than the preceding birth interval below 24 months. The risk of child mortality is 1.43 times higher for birth order 2-3 and 1.633 times higher for birth order 4+ as compared with single birth order. The risk of child mortality is found 0.958 times and 0.941 times lower for the children whose father’s having secondary and higher education as compared to the children of father’s having primary education. As compared with illiterate mothers the risk of mortality is 0.584 times, 0.341 times and 0.165 times lower for mothers who have had primary, secondary and higher education respectively. The risk of child mortality is found 0.958 times and 0.941 times lower for the children whose father’s having secondary and higher education as compared to the children of father’s having primary education. The risk of mortality is 0.850 times less for the children whose mother watching TV regularly than the children whose mother does not watch TV. The risk child mortality was found 0.017 times lower for the children whose mother currently breastfeeding to their children as compared to the children whose mother’s were not currently breastfeeding their children. Breastfeeding plays an important role in the growth, development and survival status of infant and child. Therefore, from the findings we can draw the following recommendations which will be helpful for Government and Non-Government Organizations as well as policy makers:i. To enhance educational facilities for women, age at marriage, length of birth interval and breastfeeding practices in order to reduce child mortality. ii. The government should strengthen its maternal and child health care activities especially community based health care centre for lessening child mortality.Furthermore, factor analysis, component analysis and discriminant analysis would be employed for identifying the effecting factors on child mortality in future.