-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Psychology and Behavioral Sciences
p-ISSN: 2163-1948 e-ISSN: 2163-1956
2013; 3(1): 11-17
doi:10.5923/j.ijpbs.20130301.02
Positive Role of Maternal Education on Measles Vaccination Coverage in Bangladesh
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLS. M. Raysul Haque 1, Wasimul Bari 2
1Environment, Health & Safety unit of Banglalink, Telecom Company, Bangladesh
2Department of Statistics, Biostatistics & Informatics, University of Dhaka, Bangladesh
Correspondence to: Wasimul Bari , Department of Statistics, Biostatistics & Informatics, University of Dhaka, Bangladesh.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Despite increased funding in measles vaccination programs by national governments and international aid agencies, basic factors hinder achievement of childhood measles immunization to levels compatible with other EPI (extended program on immunization) vaccines. One of such factors is maternal education status. This study aims to demonstrate the eventual influence of maternal education status on measles vaccination coverage among children of age 9 to 59 months in Bangladesh. A nationally representative data Bangladesh Demographic and Health Survey (BDHS) 2007 was used for this purpose. Sample size for this study was 3916 children from the different part of the country born within last five years preceding the survey. Logistic regression analysis was applied to examine the influence of maternal education on uptake of measles vaccination as well as other relevant variables such as place of residence, media exposure, birth order, sex of the child etc. The results of the analysis show that mother’s education level is positively and statistically significantly associated with the likelihood of a child being vaccinated for measles after controlling for all other potential factors.
Keywords: Measles Vaccination, Maternal Education, BDHS, Logistic Regression Model
Cite this paper: S. M. Raysul Haque , Wasimul Bari , Positive Role of Maternal Education on Measles Vaccination Coverage in Bangladesh, International Journal of Psychology and Behavioral Sciences, Vol. 3 No. 1, 2013, pp. 11-17. doi: 10.5923/j.ijpbs.20130301.02.
Article Outline
1. Introduction
- Measles is a highly contagious but vaccine preventable, viral infection, with a case fatality rate of up to 10%. Globally, an estimated 10 million cases and 164,000 deaths from measles occurred in 2008[1]. Measles vaccination is a cost-effective intervention for preventing measles infection. Vaccination for measles has been part of the World Health Organization’s (WHO) recommended immunization series since the inception of Expanded Program on Immunization (EPI) in 1974. Routine measles vaccination coverage was selected as the third indicator of progress towards the Millennium Development Goal (MDG 4), of reducing under-five mortality rates by two-thirds by 2015, compared with 1990 baseline data. According to the WHO, by 2008, measles vaccination coverage was 83% globally among children aged 12–23 months old. Nearly 700 million children aged between 9 months to 14 years living in high-risk countries, were vaccinated against the disease within 2000 to 2008 and globally measles deaths declined by 78% during this period, indicating that the global measles vaccination campaign successfully prevented over 3.6 million deaths [2, 3, 4].The lowest rates were in the South-East Asian (75%) and African (73%) regions. In low-income countries, 76% of children aged 12–23 months had received measles vaccination[4]. However, measles continues to be a major public health problem among children in developing nations, with measles deaths predominantly occurring among children aged below five years. Children living in developing countries with low income and poor health infrastructure are at the highest risk of measles-related morbidity and mortality. Most of the world’s measles-related deaths occur in nations with the lowest measles vaccine uptake [5, 6].According to WHO (The World Health Report 2005) measles is the fifth leading cause of death among children under five years of age in Bangladesh. Annually, an estimated 20000 children die from measles in the country (The World Health Report 2005). So far, the routine measles vaccination coverage has reached only 83.1% (BDHS, 2007) and measles vaccine is 85% efficacious when given at 9 months of age. As a result, around 40% of children in each birth cohort remain susceptible to measles due to dropout, left out and failure to develop immunity. A study conducted by Chowdhury et al (2003) has illustrated the overall difference in BCG and measles coverage in Bhairab, Bangladesh. This study shows that nearly 90% of girls received BCG, while this dropped to 70% for measles[7]. As the BCG vaccination is given at birth, it is more likely to be completed, whereas the measles vaccination is given at a certain age and not in combination with other vaccines, the mother gets occupied in different issues, so the rate may fall for this reason. In 2004 about 9743 measles cases were detected in Bangladesh which was near about triple in 2005 that is 25935 [8]. After that in September 2005, government of Bangladesh in collaboration with Government of Japan, Centers for Disease Control (CDC), WHO and UNICEF launched one of the largest mass measles campaigns ever implemented in the world. This Measles Catch-up Campaign, which is called the Haam Protirodhe Tikadan Campaign 2005-2006, was an opportunity to cover all dropout, left out and failure to develop immunity cases. During this campaign (phase-1, September 2005), approximately 35 million children of the age of 9 months to <10 years was targeted to be vaccinated against measles. Phase-2, (February to March 16th 2006) would cover 33.5 million children. After this initiative in 2006 we found 6,192 and in 2007, 2,924 measles cases. But we are still at risk of this disease. According to BDHS 2007 the measles vaccination coverage is 83.1% but other vaccine coverage is high like BCG- 96.8%, 1st dose of DPT-96.8%, 1st dose of polio-97.7%. So in comparison to these vaccines measles vaccination coverage is still not satisfactory and as an indicator of MDG-4 our target is to reach 100% by 2015.The importance of mothers’ education for child survival was brought into focus by Caldwell’s seminal paper on Nigeria. This paper argued that education of women played an important role in determining child survival even after control for a number of other factors, including such socioeconomic characteristics of the husband, as his educational level and occupation [9]. During 1980s, the realistic knowledge concerning the associations between maternal education and child survival at the micro-level expanded considerably as a result of the World Fertility Survey (WFS) program[10] and from a United Nations study which used both survey and census data[11] . Both of these major studies showed that increased levels of mother’s education were associated with improved chances of child survival in a wide range of developing countries. Both studies suggested that the associations between mother’s education and child survival were stronger in Asia than in sub-Saharan Africa. Therefore, the relationship between maternal education and children's health is no longer an issue to be debated. There still exists a lack of research information on vaccination coverage and the role of maternal education. Others socio-economic factors like income, occupation, and social class are often mentioned as important factors in influencing vaccination coverage. A few of the possible ways that have been focused so far are pointed out below for education as a potential determinant for increasing vaccination coverage specially measles vaccination uptake: (i) Education gives the basic ideas about the path of wellbeing and also equips and encourages increasing mother’s knowledge on healthy living; (ii) Education equips mothers with the knowledge of proper health behavior and illness behavior for preventive and curative measures[12]; (iii) Education makes the mothers more willing to use health care services when necessary and preparing them for overcoming the barriers in doing so[13,14]; (iv) Education allows greater exposure to the mass media, which can keep mothers better informed about the health issues[15]; (v) Education empowers mothers to make and implement proper and timely decisions regarding their children's health[16].An empowered woman can look after the health issues of her offspring better than an un-empowered or underpowered woman. Thus, we find maternal education as a gate way toward improving immunization specially increasing measles vaccination coverage as it is still low in comparison to other vaccine coverage. According to BDHS 2007, the measles vaccination coverage is 83.1% but the target to reach MDG is 100% by 2015. According to John Hobcraft, education differentials in extent of measles vaccination were usually in the 10-to-20 percentage points range after controlling all other socio-demographic variables [17].This paper analyses the probability of a child being vaccinated against measles, specifically focusing on the influence of maternal education status at different levels. We have also considered other important factors that are mentioned in literatures. In this paper, we have used published BDHS 2007 data due to maintain the validity and reliability as this is the only nationally accepted reliable data set in Bangladesh.
2. Research Hypothesis
- The hypothesis considered in this paper is stated as “Maternal education can increase the measles vaccination coverage in Bangladesh”. In Bangladesh, in spite of all efforts, the vaccination coverage for measles is not much high like the other EPI vaccines. Therefore, if it can be proved that there exists a significant positive association between maternal education and measles vaccination coverage, in future by giving proper attention to maternal education the measles vaccination coverage can be increased remarkably in Bangladesh.
3. Data and Method
- This study uses data from the Bangladesh Demographic and Health Survey (BDHS) 2007. The BDHS 2007 survey was performed under the authority of the National Institute for Population Research and Training (NIPORT) of the Ministry of Health and Family Welfare. DHS-Bangladesh - 2007 covered a nationally representative sample of 11,440 ever married women of age 10– 49 years and their children born 0–59 months prior to the survey date. BDHS 2007 is a stratified, multistage cluster sample with 227 rural PSU’s (primary sampling units ) and 134 urban PSU’s. An average of 30 household was selected from per PSU. The unit of analysis is the child. In order to reduce the recall bias in the BDHS survey, information regarding Antenatal care (ANC), Post natal care (PNC), immunization, diseases etc. was asked only for the children of age less than 60 months. Therefore, a file was created for the sample of children of age 0–59 months including all variables of household and mother. In absence of income or consumption data, BDHS 2007 used household assets to construct a wealth index using principal components analysis The sample size used in the analysis is 3916 children. Note that all the children are of age between 9 and 59 months and they are the last child of respective respondents prior the survey. Here we have considered eleven variables out of which one is dependent variable and ten is independent variables. Measles vaccination among 9 to 59 month children is dependent variable, outcome either vaccinated or not. Independent variables are: Level of education: four levels of education, no education, primary education, secondary education and higher education group; Place of residence: two groups that are urban and rural; Media exposure: Exposed and non-exposed to the media; Wealth index: Within the wealth index we have considered three groups. Poor, middle class and rich; Place of delivery: two groups that are hospital or institutional delivery and non-hospital delivery; Age of mother at first birth: two age groups, age up to 18 and age above 18; Birth order: three groups, 1st birth, 2nd-4th birth and 5th or more; Sex of the index child: male and female; Religion: two groups, Muslims and non-Muslims; and Mothers working status: Two groups, working and not working.The analysis was done into three steps. Firstly, univariate analyses were done for both dependent and independent variables. Then, bivariate analysis was done to examine the association between the dependent variable and all other independent variable separately. Finally, multivariate analysis was done by fitting the logistic regression model for measles vaccination to examine the impact of maternal education after controlling the other factors. This was done by following a step-by-step procedure and we included the factors in the logistic regression model those are found to be statistically significant in the bivariate analysis. In first step, we consider measles vaccination and level of education that means primary, secondary and higher in reference with no education. In second step along with education we include wealth index that means poor and rich with the reference of middle income group and place of residence as rural with the reference of urban area. In third step, along with education, wealth index and place of residence we include mother’s age at first birth as age above 18years with the reference of age below 18years, place of delivery as hospital with the reference of non-hospital and birth order as the first birth and the 5thand above birth with the reference of the 2nd to 4th birth. In last step, along with the above variables here we include media exposure as exposed with the reference of non-exposed.
4. Results
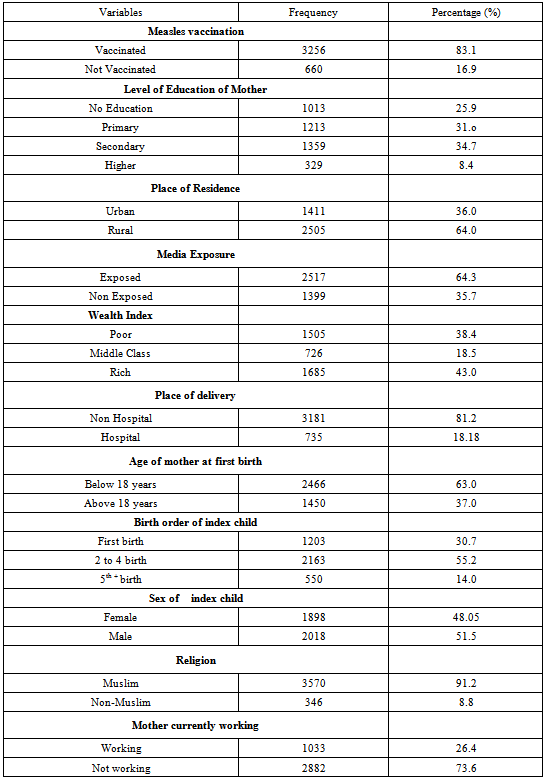
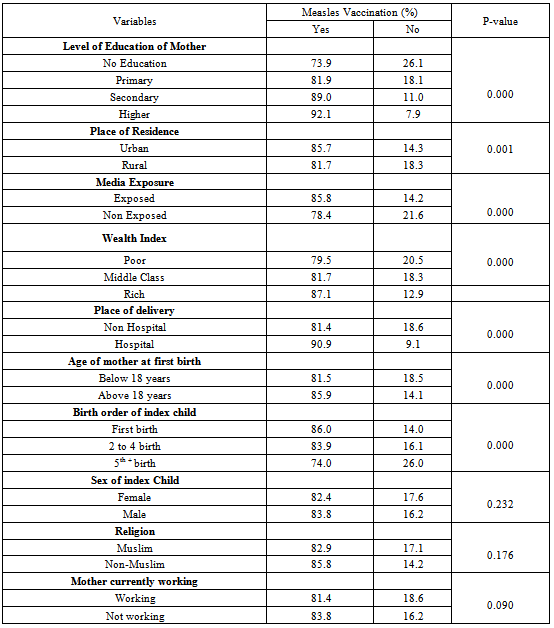
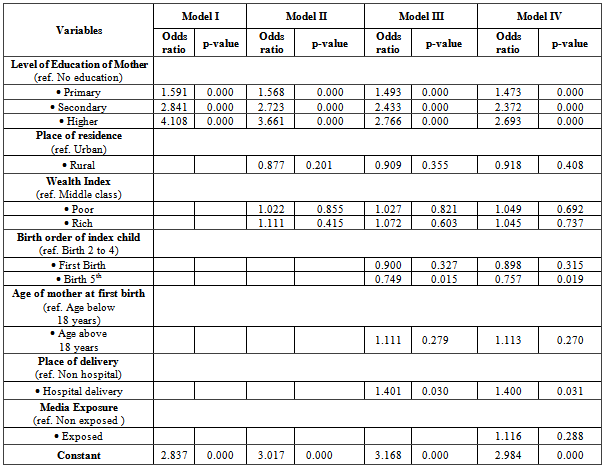
- Table 1 describes the profile of both dependent and independent variables. In case of measles vaccination, out of 3916 cases 83.1% was vaccinated while 16.9% were not vaccinated. Among the independent variables, our main point of interest is level of education .Within level of education, 25.9% are in no education group, 31.0% are in primary education group, 34.7% are in secondary education group, while higher education group consists of 8.4%. Among the respondents, 64.0% people reside in rural area while 36% reside in urban area. Respondents in exposure with media are 64.3% while 35.7% are not in exposure with media. In case of wealth index, 43.0% are rich, 38.4% are poor and 18.5% are in middle class group. Hospital delivery is very few (18.18%) in compression with non-hospital delivery (81.2%). Out of 3916 mother, 63.0% experienced with their first child within 18 years of age. Majority that is 73.6% mothers are not working while 26.4% mothers are working. In case of religion, we find that 91.2% are Muslims. Within Birth order, the 1stbirth group consists of 30.7%, the 2ndto 4th birth group consists of 55.2% while 14% are in the 5th and more birth groups.Table 2 represents the results obtained from the bivariate analysis for measles vaccination with all independent variables. Out of all independent variables three appears insignificant as p-value is greater than 0.05. These three variables are sex of the child, religion and working status of mother. Note the p-values for these three variables are 0.232, 0.176, and 0.090, respectively. Out of remaining seven significant variables, under the level of education, higher education group has highest measles vaccination coverage that is 92.1% and the secondary and primary group have 89.0% and 81.9% measles vaccination coverage respectively. No education group has lowest measles vaccination coverage which is 73.9%.Measles vaccination coverage is slightly higher in urban area (85.7%) in comparison to rural area. Those who are in exposure with media have higher coverage (85.7%) in comparison to those who are not in exposure (78.4%) with media. Within wealth index, measles vaccination coverage is lowest among poor peoples, which is (79.5%) and highest among rich people, which is 87.1%. Coverage among middle class group is 81.7%. In case of place of delivery, measles vaccination coverage is higher for those who were delivered in hospital (90.9%) and lower in non- hospital delivered children which is 81.4%. Mother who experienced their first child above 18 years, vaccination coverage is relatively higher for their children (85.9%), in comparison to those who experienced their first child below 18 years (81.5%). Considering the birth order measles vaccination coverage in highest in first birth group which is 86.0% and lowest among the 5thand more birth group which is 74%. Coverage among the 2nd to 4th birth group is 83.9%.In Table 3, Model I presents the first logistic model for measles vaccination along with level of education represented by primary, secondary and higher education group. It is found that all the education levels have a significant (p-value=0.000) positive impact on the vaccination coverage. With the reference of no education group, higher education group has 4.108 times higher vaccination coverage while secondary and primary group has 2.841 and 1.59 times higher coverage respectively.Model II presents the second logistic model for measles vaccination where we include place of residence and wealth index along with level of education. After including these two variables along with education, education still remains highly significant for measles vaccination coverage. The p-value is still 0.000 for higher, secondary and primary group. Here, higher secondary and primary group has 3.661, 2.723 and 1.568 times higher coverage than no education group. In this model, place of residence and wealth index are not found to have significant effect on measles vaccination coverage.
|
|
- Model III in Table 3 represents the third logistic model for measles vaccination where we include birth order, mother’s age at first birth and place of delivery along with variables considered in Model II. After considering all these variables, education still remains highly significant for measles vaccination coverage where higher, secondary and primary education group has 2.766; 2.433 and 1.493 times higher coverage than no education group. The 5thand more birth groups has 0.749 times less measles vaccination coverage than the 2-4th birth groups. It is found statistically significant since p-value is 0.015. Measles vaccination coverage in hospital delivery group is 1.401 times higher than non-hospital delivery group. It is also found statistically significant with p-value 0.030.Model IV represents the last logistic model for measles vaccination where we include the media exposure variable along with all variables considered in Model III. After considering all seven variables in model IV, educations still remains highly significant for measles vaccination coverage. Still higher, secondary and primary group has 2.693; 2.672 and 1.474 times higher coverage than no education group. The 5th and more birth groups has 0.757 times less measles vaccination coverage than the 2-4th birth groups. It is found statistically significant since p-value is 0.019. Place of delivery is significant for measles vaccination coverage where hospital delivery group has 1.4 times higher vaccination coverage than non- hospital delivery group and p-value is 0.031. Media exposure is not significant for measles vaccination coverage in this model.
|
5. Discussion
- In this study, we explored the role of maternal education in determining the possibility that children receive measles vaccination. The possibility that a child received measles vaccination increased with increasing levels of maternal education. This result was shown to be independent of other possible important variables. The results of the current study comply with previous studies investigating factors associated with measles vaccination coverage in developing countries. It was found in a study that children whose mothers had attended secondary school or higher, had nearly 40% higher immunization coverage rates than those whose mothers had not attended school [18, 19]. Marks et al, investigated vaccination in the United States, finding that maternal education was a significant predictor of childhood vaccination coverage[20].The relative increases in female education are account, in part, for the considerable improvements in measles immunization coverage. So, maternal education is likely to play a critical role in efforts to improve childhood immunization. A greater investment in creating educational opportunities for mother in our country is urgently required. Adequate health communication strategies on the benefits of vaccination should be designed to appeal to both fathers and mothers. Community and religious leaders should be encouraged to advocate in favor of maternal education. It is acknowledged that removing the hindrances on maternal education in nations could be an effective strategy for a significant progress in measles vaccination uptake. Education is essential to adopts things those effects are not visible immediately and vaccination is one of them. Coverage of other EPI vaccines are relatively high in comparisons to measles as their schedule usually completed with few days to 14 weeks whereas schedule for measles vaccine is as soon as possible after 9 months, relatively longer duration than other vaccines. Mothers especially the illiterate one get reluctant about the measles vaccine as it is far away from the birth date. Education plays a vital role in understanding the delayed uptake schedule of measles vaccine and this understanding helps mother to complete their child immunization schedule within 1 year by getting measles vaccines for their children.Though there have been no significant measles outbreaks in Bangladesh recently, measles is still a highly infectious and produces fever and catarrhal symptoms of upper respiratory tract followed by a typical rash among the sufferers, who are most likely to be young children. Measles is still a leading killer among vaccine-preventable diseases of childhood in Bangladesh, taking its toll mainly among malnourished children. If one child gets infected with measles, the probability, for the rest of the children in locality, of getting infected with this disease is very high as transmission occurs directly from person to person mainly by droplet infection from 4 days before the onset of rash until 5 days thereafter. Moreover, there is no specific treatment for measles except managing the complication; so prevention through the good immunization coverage is the best way to reduce the child mortality and morbidity rates considerably. Results obtained from this study revealed the fact that there is a positive association between maternal education and measles vaccine coverage, which supports the research hypothesis considered in this paper. Policymakers and practitioners need to work together to increase the measles vaccine coverage in the country through education campaign for women. Therefore, it is necessary to have policy level decisions and social movements to address this issue for attaining MDG 4 (reducing under-five mortality rate by two thirds). As BDHS 2007 data that was used in the paper did not fully cover the diversity and complexity of social dynamics of Bangladesh, extensive empirical study is required to derive conclusive results. We did not consider the variable age at which the child was vaccinated since it is not available in the data set. One can consider this variable as an outcome variable and explore more information by applying techniques of survival analysis.
ACKNOWLEDGEMENTS
- We would like to thank National Institute of Population Research and Training (NIPORT), Bangladesh for allowing us to use BDHS 2007 data for our analysis.