-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Psychology and Behavioral Sciences
p-ISSN: 2163-1948 e-ISSN: 2163-1956
2012; 2(4): 120-129
doi: 10.5923/j.ijpbs.20120204.07
Evidence of Incremental Validity between Pfister Test and Human Figure Drawing
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-Text HTML
Full-Text HTMLClaudio Garcia Capitão , Lucila Moraes Cardoso
Department of Psychology, São Francisco University, São Paulo, 01258-020, Brazil
Correspondence to: Claudio Garcia Capitão , Department of Psychology, São Francisco University, São Paulo, 01258-020, Brazil.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
The aim of this study was to seek incremental evidence of validity between the Color Pyramid Test (CPT) and the Human Figure Drawing (HFD). The incremental validity of information obtained from a given test can predict something unique, which other existing measures or constructs cannot predict. The sample consisted of 118 children from public schools in the state of Sao Paulo, Brazil, of which 59 (50%) were male, aged between 6 and 12 years (M = 9.22, SD = 1.75) and education ranging from pre-kindergarten to seventh grade. The tests were administered on each child without predetermined time for their implementation. The results showed significant correlations between the two tests, which contributed to the evidence of incremental validity between the two tests. It is suggested that further studies on the evidence of validity and accuracy, with controlled samples and other indicators,not explored in this study, will contribute to the projective techniques surveyed.
Keywords: Correlation, Psychological Assessment, Projective Methods, Pfister Test, Human Figure Drawing
Article Outline
1. Introduction
- The projective techniques, often called the projective hypothesis, are the most intriguing topics, both in psychological testing and overall psychology. They are among the most easily recognizable symbol of psychology in contemporary society. In projective techniques, the response is formuled in terms of desires, fantasies, inclinations and fears of the person. Therefore, it is believed to be an ideal way to know the personality traits of an unconscious person.The term “psychological evaluation” was defined as a set of assessment processes, administered by licensed psychologists, to form impressions and images of other people’s behavior, or mental health, while combating with the situation. The information thus obtained is helpful for making decisions and testing hypotheses to reveal the deviant personality characteristics[1]. The appropriate use of assessment techniques requires that psychologists should adhere to the numerous activities and psychological processes involved in them. This requires some diversification of techniques ([2],[3]), as well as care in the use of reliable instruments, which have good psychometric properties ([4],[5]).The resources analyzing the projective phenomenon, i.e., information about what is going on internally with a person from the externalized perception about a particular stimulus, are known as tools, measures or projective techniques[6]. Projective instruments such as the Human Figure Drawing (HFD) and the Pfister Color Pyramid Test (CPT), use instruments like personal interviews and self-report scales, to access information[7]. It is expected that through different projective techniques, the information about the subject is known by his/her behavior and spontaneous tendencies, egocentricity, driven by implicit needs and more likely to become manifested in specific contexts, than the self-report techniques where the implications of a reason or a special needs are clear to the subject[7].Moreover, it has been emphasized that no trace is meaningful in the evaluation process if considered in isolation.It is necessary to consider the application context, as well as the set of indicators to have an integrated view of the points and make appropriate use of the numerous variables to be analyzed ([8],[9],[10]). Thus, the low correlation of scores for different measures for evaluating the same construct does not necessarily mean a problem of incremental validity. This is because sometimes the lack of weak correlation or low magnitude is evidence to support the validity of projective techniques, demonstrating its clinical and empirical usefulness for certain constructs[11].The low correlations in projective techniques can be interpreted as the results of unique aspects of each person's livings. It is possible that the correlations can identify a common point on a particular aspect and that others have no relation to each other since they relate to the peculiar way on how each person perceives and deals with conflicts. Thus, the low correlations among projective techniques seems to be associated with evidence of incremental validity, which are obtained when the data generated by a particular instrument relate to something unique, that is, something that other measures or constructs already existing do not predict[12].This study will consider the correlations between two projective methods, the CPT and the HFD. Both the techniques are nonverbal, interesting, doesn’t need any major educational qualifications and can be implemented rapidly ([13-15],[10]). Both methods allow the symbolic manifestations of the feelings, showing how the person perceives himself and those around him.CPT is introduced by Max Pfister, a Swiss psychologist to reveal deviant personality characteristics of the examinee.In this test, the examinee is asked to complete the pyramid schemes with colorful small squares. The affective and emotional dynamics, as well as the structural and cognitive functions of the examinee can be known by the way he approaches the task, the choice of color combinations and the unique way of composing the elaborate pyramid. This test also checks for any sort of abnormality, if it reacts to emotional stimuli with lower or greater control of cognitive functions[10].The research is conducted based on the databases obtained from Virtual Health Library (VHL). The survey in the database was based on the criterion: BVS - Psi Brazil, published between 2001 to 2011. This search led to the identification of 12 papers that used the CPT as the main instrument for psychological evaluation. Eight of the 12 papers (66.6%) used CPT for analyzing the psychometric qualities. Then six of the eight papers (75%, which is 50% of 12 papers) were looking for evidence of validity of the technique and two (25%, which is 16.6% of 12 papers) were regulation studies). The remaining 33.3% addressed the use of CPTin specific contexts of action in the psychic functioning in elderly women.Reference[16] considered Pfister validity as a reliable tool for diagnosis of obsessive compulsive disorder,[17] established indicators of alcoholism,and[18] identified symptoms of panic disorder through some indicators of the Pfister. Other references[19] and[20] identified patients with depression and schizophrenia, respectively. Pfister, which is associated with other diagnostic features, is emphasized in all the studies for added security. The sixth study found evidence of validity between Pfister and HFD[21].HFD is an evaluation technique, where the examinee is assessed in terms of intellectual functioning and qualitative measure of personality, by analyzing the human figure drawn by him[22]. The test is treated as a projective technique to measure mental maturity, and assuming that there is a set of signals found in this particular technique, which relates to the children's attitudes and concerns, known as emotional indicators. The emotional indicators reveal the child’s anxieties, concerns and attitudes irrespective of age and maturity. There are other indicators, known as Evolutionary Items, which are not often found in the younger children’s drawings but are relatively common with the increasing age of the child. There is also the set of indicators known as Expected Items, where the omission is considered. The omission of any parts of the body indicates excessive immaturity, delay or regression due to emotional problems.Fifteen articles on HFD were found in the database BVS-Psi Brazil within the period of 2001 to 2011. Seven of the 15 articles used the Koppitz scoring system, two sought for evidence of validity of the system through correlation with other scoring systems. One of the studies linked HFD with CPT and found validity evidence[23] and the other sought for concurrent validity between the HFD and Test R-2. It was concluded that the Drawing scoring systems, such as Koppitz (r = 0.575) or the Goodenough-Harris (r = 0.606), in correlation with R-2, are suitable for cognitive evaluation of children([24],[25],[26],[27]).The other five studies were applied research, in which the projective instrument was used to generate information about a specific context, namely, personality assessment of obese children([28],[29],[30],[31],[32]). It was used to verify the typical conflicting behaviors of females in their early adolescence[33]. It is further used, to seek evidence for HFD validity of deaf children[34], to analyse the personality of children with bruxism[35] and to verify the contributions of HFD for designing the psychological profile of a group of morbidly obese patients[36]. Other studies have either used other HFD scoring systems, or have not explained about their scoring systems.HFD and CPT enable the evaluation of various emotional indicators, thereby, justifying the relevance of studies dedicated to improve the psychometric qualities of the instruments ([17-20],[14],[15],[21],[22]). The present study sought evidence of incremental validity by the correlation between the CPT and the HFD.
2. Method
2.1. Participants
- Participants for this study were selected through non-random sampling as per their convenience,at different public institutions in the state of São Paulo, Brazil. The sample consisted of 118 children, among which 59 (50%) were male and the rest were females. Their age ranged between 6-12 years (M = 9.22, SD = 1.75).Their education level ranged from pre-kindergarten to seventh grade. This age group of childrensignified no history of low academic performance. Of the total number of children, 12 (10%) attended preschool, 18 (15%) attended the first-grade, 25 (21%) attended the second-grade, 18 (15%) attended the third grade, 24 (21%) attended the fourth grade, 12 (10%) attended the fifth grade, eight (7%) attended the sixth grade and only one child (1%) attended the seventh grade.
2.2. Instruments
2.2.1. Pfister Color Pyramid Test (CPT)
- The CPT consists of three beige colored cards with a pyramid scheme designed in each one of them and a set of 24 small squares of different shades and tones of red, green, blue, purple, yellow, orange, brown, black, white and grey[10]. The examinee was asked to choose any colored small squares of his liking, and to place them on the pyramid scheme. The examinee was requested to fill three pyramid schemes one at a time. After completing the test, the pyramid schemes were verified to reveal the different personality characteristics of the examinee[10]. In the present study, indicators such as formal aspect, percentage of colors and chromatic syndromes are considered. The chromatic syndromes refer to specific color combinations. Normality syndrome is one such chromatic syndrome, where a combination of Blue, Red and Green is evident. Similarly, in stimulation syndrome, a combination of Red, Yellow and Orange is evident in cold syndrome a combination of Blue, Green and Purple is evident, in Colorless syndrome, a combination of Black, White and Grey is evident and lastly, in dynamism syndrome, a combination of Green, Yellow and Brown is evident.A standardization study[30] presented normative tables to the state of Sao Paulo, for analyzing the frequency of colors and the formal aspect of the pyramids. Another study[31] conducted a comparative analysis between two regional groups (southeast and northeast) of Brazil. This study found out a marked difference between two regional groups. The frequency of the orange color is much more in the southeastern Brazilian group as compared to the northeastern group. Again, the northeastern Brazilian group showed a marked demotion in the formal aspect.
2.2.2. Human Figure Drawing (HFD)
- Reference[16] suggested for HFD administration, in which the examinee receives the direction “draw a whole person”. If the examinee hesitates to follow the direction, the examiner assures him/her by saying, "there is no beautiful or ugly drawing, right or wrong, the drawing I’m requesting is that, one you can accomplish." After the accomplishment of the above, the investigation was carried out. The survey questions corresponded to the questionnaire, to be used as a tool for the evaluation of the children’s mental and behavior[13]. For coding, tables were used for correction and classification of the manual of HFD evaluation with standardization for Argentina[16].
2.3. Procedures
- The project, which maintained the ethical standard of research, was approved by the Ethics Committee in Research of the University and submitted to the institutions. The agreement was made between the responsible authorities of the schools and the parents, with due respect for the children’s acceptance. For instruments administration, there was a concern regarding performing it in a pleasant and appropriate environment to establish good rapport. The tests were administered individually in a single session, without time limitation for performing the task. At first the CPT was applied and then the HFD.The choice of the order of the instruments came from some projective hypotheses. The first hypothesis refers to the fact, that the CPT has an indicator related to the mode of execution and application, which depicts the behavior ofthe person, while facing the new tasks, but HFD technique have no such indicators.Although these indicators have not been used in this research, the database was used for other researches that could take this indicator into consideration. The second supposition is that to fill the pyramids with colored boxes is a new task and which in general has no association with the school context, while drawing people is a relatively common task in the Brazilian school context. Although the children chosen had no history of low academic performance, it was decided to minimize the possibility of interference. Finally, it is believed that the influence of one technique over the other is minimum, since the tasks are very much different, reducing the possibility of the learning effect.
3. Results and Discussion
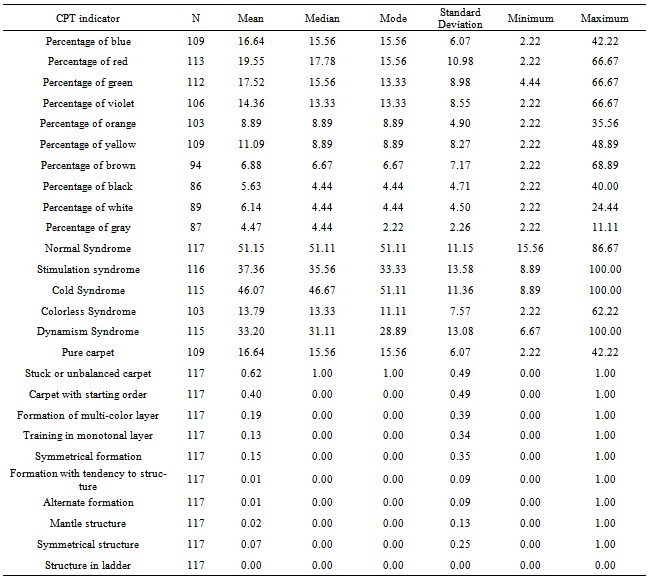
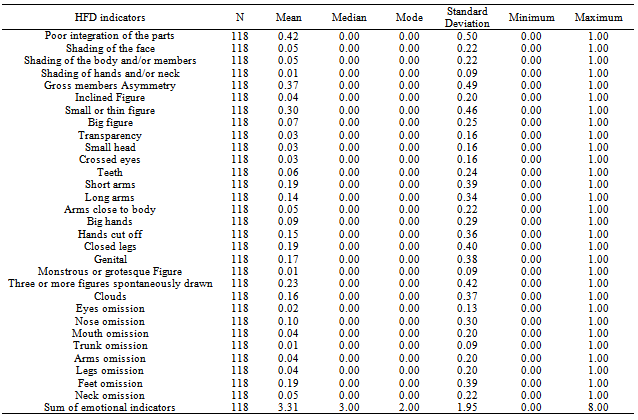
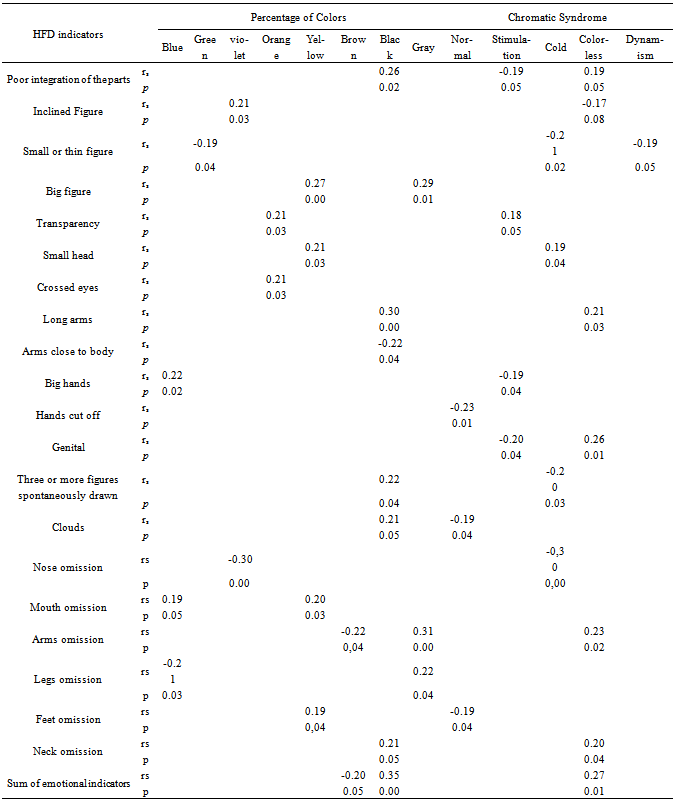
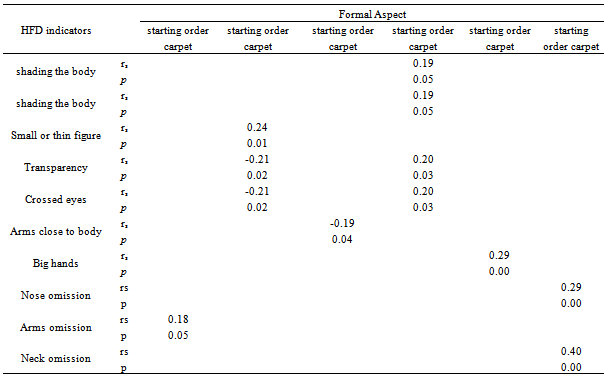
- Initially, the descriptive statistics of the CPT and HFD indicators were analyzed according to tables 1 and 2 respectively. The CPT indicators were analyzed, based on the Colors Percentage, Chromatic Syndrome and Formal Aspect, according to the criteria established in[10]. At HFD, there were 30 indicators, established by[16].The indicators (Table 1) that consider the Colors Percentage and Chromatic Syndrome, have not considered the protocol of one of the participants, as he failed to use some of the colors, and as a result the total participants came down to 117. With regard to the Formal Aspect, it was considered the presence (1) or absence (0) of each of the different types.In Brazil, there are no Pfister standards for children, therefore any comparison using normative tables[10] should be considered with some care. Still, it is noted that all percentages of colours and chromatic syndromes are in the range considered median when compared with the standards of[10].Table 2 shows the presence (1) or absence (0) of HFD emotional indicators of 118 children participating in the sample. Most of the children showed absence (0) of such indicators. While considering the sum of all the indicators, it is noted that the most frequent value was having two emotional indicators and the median was 3 (M = 3.31, SD =1.95). Reference[16] shows that the presence of more than three indicators represents emotional problems. In this case, considering the median, it is observed that approximately half of the children in the sample did not have emotional difficulties. However, there were participants, who presented sum of emotional indicator equal to 8, suggesting the presence of severe emotional difficulties. After the descriptive statistics, correlations of the CPT indicators with HFD were performed. We opted for the Spearman correlation for being a variable with nominal level of measurement. Results indicate significant correlations at p< 0.05, including some at p< 0.01. Significant data were analyzed according to the meaning of each indicator obtained in the manuals of HFD[16] and CPT[10]. The magnitude criterion of[36] was adopted to classify the magnitude of correlations. According to this criterion, correlation between 0.60 and 0.99 means strong correlation; between 0.30 and 0.59 means moderate correlation; and between 0.10 and 0.29 means weak correlation.Whenever the correlations were interpreted as negative, it was considered that the HFD indicators increase while the Pfister indicators decrease. However, in case of positive correlations, HFD increase is related to Pfister increase, and HFD decrease is also related to Pfister decrease. In literature, the ‘big figure’ relates to immaturity, expansiveness and lack of control and the increased gray color indicates timidity and caution with regard to emotional exchanges, i.e., indicates a defensive withdrawal and opposition tendency.The ‘mouth omission’ is associated with feelings of anxiety, insecurity, withdrawal, attitude of passive resistance and inability to communicate with others.Also it seems to be linked with fear, anxiety and perfectionism. The yellow suggests exaggeration of affective manifestations, less spontaneous, more stylized and superficial, in addition to immaturity, unsound structure, low frustration tolerance, instability, selfishness and irritability; whereas the blue may be associated with a feeling of inferiority, failure, dissatisfaction and ambivalence. Thus, this combination is related to insecurity and feelings of inadequacy that can lead to withdrawal and difficulty of expressing feelings.
|
|
|
|
4. Conclusions
- There were significant statistical correlations between the Pfister test and Human Figure Drawing from the statistical point of view. However the correlations were either considered weak or moderate, because the tools identify only one aspect in common.The Pfister technique allows us to understand different aspects of affective and emotional functioning, as well as some structural and cognitive functions of the examinee, while the HFD is considered a qualitative measure of personality and intellectual functioning. Inspite of the fact that they both have unique characteristics, they are used to analyze a common factor, which is associated with the dynamics of personality and cognitive functioning of the subject.Each of these techniques should be combinedly used with other instruments to contribute to the evidence of incremental validity. There were significant statistical correlations between the Pfister test and Human Figure Drawing from the statistical point of view. However the correlations were either considered weak or moderate, because the tools identify only one aspect in common.When analyzing the data, it was possible to verify theoretical association between the indicators that had significant correlations. These results provide evidences that the instruments are complementary and make it feasible a broader clinical view on the emotional functioning of children; besides this, they strengthen the importance that each one of these techniques should always be used in conjunction with other instruments.The importance of this research, besides the purpose of seeking evidence of incremental validity between the instruments, is in the fact that in Brazil there are few instruments with evidence of validity for use with children. This way, this present study contributes with evidences of validity for two other instruments that could be used for evaluation of emotional and qualitative aspects of the personality in children.One issue which is to be considered refers to the instruments having been administered in the same order, for all participants, making it difficult the observation of the influence that the instrument exerts on the other, especially in relation to the answers. This bias could have been controlled in case the researchers had inverted the order of administration of the techniques, dividing the group in two halves. Still, it is emphasized that the reliability among judges was not conducted, which would verify the accuracy of the instruments. Studies of reliability have been quite relevant and allow us to affirm the reliability of the instrument, being very important for research on projective techniques.The instruments surveyed have other indicators that could have been explored, but were not in the scope of this study. However, new researchers will contribute to evidence of validity and reliability, as well as studies on Pfister and HFD, especially in Brazil.