-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Internal Medicine
p-ISSN: 2326-1064 e-ISSN: 2326-1072
2021; 10(3): 35-39
doi:10.5923/j.ijim.20211003.01
Received: Nov. 14, 2021; Accepted: Dec. 12, 2021; Published: Dec. 24, 2021

Clinicoepidemiological Features and Management of Nasal Polyps - A Developing Country Experience
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLWaheed Atilade Adegbiji 1, Dr. Shuaib Kayode Aremu 2, Kayode Rasaq Adewoye 3
1ENT Department, College of Medicine and Health Sciences, Ekiti State University Teaching Hospital, Ado-Ekiti, Nigeria
2ENT Department, College of Medicine and Health Sciences, Afe Babalola University, Ado-Ekiti, Ekiti State, Nigeria
3Department of Community Medicine Federal Teaching Hospital, Ido Ekiti / Afe Babalola University, Ado-Ekiti, Nigeria
Correspondence to: Dr. Shuaib Kayode Aremu , ENT Department, College of Medicine and Health Sciences, Afe Babalola University, Ado-Ekiti, Ekiti State, Nigeria.
| Email: |  |
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

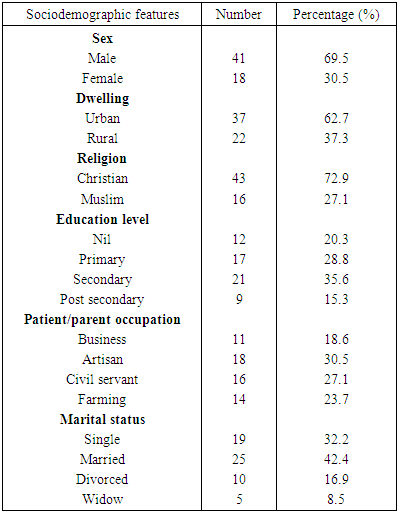
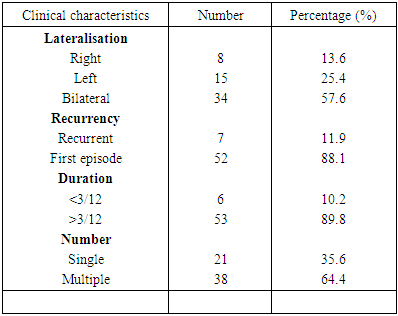
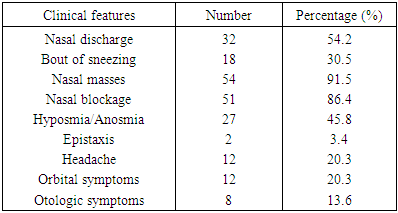
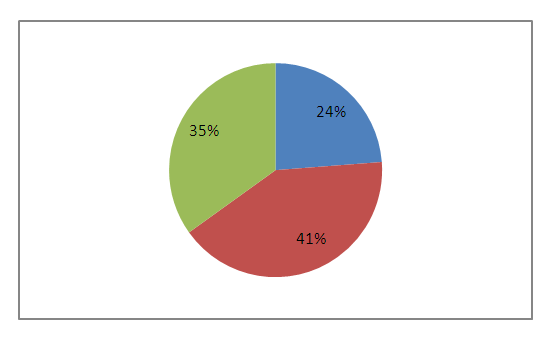
Background: Nasal polyps are common sinonasal diseases with scarce literature in developing countries. This study aimed at determining the prevalence, sociodemographic features, clinical characteristics, radiological investigation and management of nasal polyps in our center. Materials and Methods: This was a retrospective study of all the patients with nasal polyps who had surgery in ear, nose and throat department of Ekiti state university teaching hospital. The study was carried out from July 2009 to June 2019. Detailed data on the patients were retrieved from our out patients clinic register, emergency ward register, theatre register and hospital medical record and documented. All the data obtained were collated and analysed by using SPSS version 18.0. Results: Prevalence of nasal polyps was 1.2%. There was 69.5% male with male to female ratio of 2.3:1. Urban dwellers accounted for 62.7%. Nasal polyps were 57.6% bilateral, 25.4% left sided and 13.6% right sided. First episode occurred in 88.1% and recurrent cases in 11.9%. Chronic cases (>3|12) was commoner than acute cases (<3|12) in 89.8% and 10.2% respectively. There were multiple grapelike nasal polyps in 64.4% and single nasal polyps in 35.6%. There were ethmoid (simple) polyps in 81.4% followed by nasal cavity polyps in 15.3% and antrochoanal polyps in 3.4%. Main clinical features were nasal masses 91.5%, nasal blockage 86.4%, nasal discharge 54.2%, hyposmia/anosmia 45.8%, bout of sneezing 30.5% and headache 20.3%. Nasal polyps extension were 81.4% Intranasal/paranasal sinuses, 28.8% orbital extension, 6.8% pharyngeal extension and 5.1% intracranial. Associated comorbid illnesses were allergic rhinitis, infective rhinosinusitis and asthma in 44.1%, 37.3% and 25.4% respectively. All patients were managed by surgically as intranasal polypectomy 76.3%, Caldwell Luc procedures 13.6% and external frontoethmoidectomy 10.2%. Postoperative steroid therapy was offered to 66.1%. Conclusion: Nasal polyps are idiopathic common sinonasal chronic disorder. There is associated late presentation with longstanding progressive nasal obstructions. All patients had surgery and medical treatment.
Keywords: Nasal polyps, Sinonasal surgery, Steroid, Developing countries, Nigeria
Cite this paper: Waheed Atilade Adegbiji , Dr. Shuaib Kayode Aremu , Kayode Rasaq Adewoye , Clinicoepidemiological Features and Management of Nasal Polyps - A Developing Country Experience, International Journal of Internal Medicine, Vol. 10 No. 3, 2021, pp. 35-39. doi: 10.5923/j.ijim.20211003.01.
Article Outline
1. Introduction
- Nasal polyps is sinonasal disorder with a pedunculated oedematous mucosa that arises from the mucosa of the nasal and paranasal sinuses [1,2]. Nasal polyps is a form of chronic rhinosinusitis of the sinonasal mucosa [3]. Nasal Polyps are common sinonasal disorder affecting 1-4% of adult population worldwide [2]. It is commoner in male and adult also very uncommon in children under 10 years. The aetiology of nasal polyps is multifactorial or unknown (idiopathic) [4,5]. They can be associated with other respiratory diseases like allergy, asthma or aspirin sensitivity [6]. Patients with Samnter’s Triad have polyposis, asthma, and aspirin hypersensitivity. Nasal polyps appear as smooth, round, semi-translucent, single or multiple grapelike masses that are most commonly found in the middle meatus and ethmoid sinuses. Nasal Polyps may be clinically silent [7]. It may present clinically with nasal obstruction, congestion, mouth breathing, hyposmia, rhinorrhea, postnasal drip, headaches, snoring and sleep apnoea. On sinonasal examination, nasal polyps more commonly appear bilaterally but may also present unilaterally. CT scan is essential if surgical treatment is required it will show the extent of nasal polyps and anatomical variations [8]. Plain X-rays are insensitive and MRI scan may aid in the diagnosis of neoplasia [9]. Histological examination is required for definite diagnosis and to rule out malignancy.The management of nasal polyps can be either medical or surgical or both depending on the nature. In failed medical therapy or large-sized nasal polyps, polypectomy is performed [10,11]. Topical corticosteroids are used to reduce the size of the polyps, improve nasal breathing and prevent recurrence. Despite treatment there has been high recurrence rate of nasal polyps also a challenges to otorhinolaryngologist.In developing countries there have been fewer studies in literature on clinicoepidemiological and surgical management of nasal polyps particularly in Nigeria. Due to paucity of information this study aimed at determining the prevalence, sociodemographic features, clinical characteristics, radiological investigation and management of nasal polyps in our center to control this disorder.
2. Materials and Methods
- This was a retrospective study of all the patients with nasal polyps who had surgery in ear, nose and throat department of Ekiti state university teaching hospital. The study was carried out over a period of ten years (from July 2009 to June 2019). Data were retrieved from our out patients clinic register, emergency ward register, theatre register and hospital medical record. Data on sociodemographic features such as age, sex, religion, marital status, education and occupation were retrieved. Detailed information on presenting complaint, duration of symptoms, associated condition on symptoms of nasal polyps (bilateral or unilateral) which includes nasal obstruction, rhinorrhea, facial pain, headache, epistaxis, snoring, mouth breathing, voice changes, ear problems, eye problems and facial deformity due to polyposis were retrieved. Social and family history such as asthma, allergy, allergic rhinitis, cystic fibrosis and previous medical or surgical treatments were further obtained. Findings from otolaryngological physical examination were obtained. Investigations including CT Scan findings and diagnosis were also retrieved. Informed consent was obtained from each patient enrolled in the study.The procedures performed on nasal polyps included simple Intranasal polypectomy and functional endoscopic sinus surgery (FESS) while extranasal approach were Caldwell-Luc procedure and external frontoethmoidectomy. All histological diagnoses of the nasal polyps were retrieved and documented.All the data obtained were collated and analysed by using SPSS version 18.0 computer software. Descriptive statistics analysis by frequency table, percentage with pie and bar charts figures were used to express our findings.
3. Results
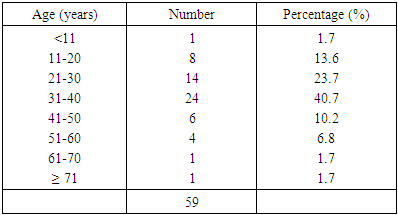
- A total of 5,078 patients were managed over the studied period out of which 59 had nasal polyps with prevalence of 1.2%. Nasal polyps occurred in all the studied age groups and the peak prevalence of 24 (40.7%) at age group (31-40) years as showed in Table 1.
|
|
|
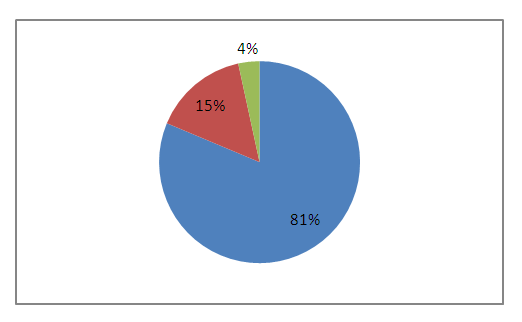 | Figure 1. Anatomical location among patients |
|
|
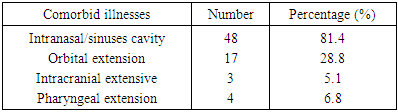
 | Figure 2. Associated co-morbid illnesses among patients |
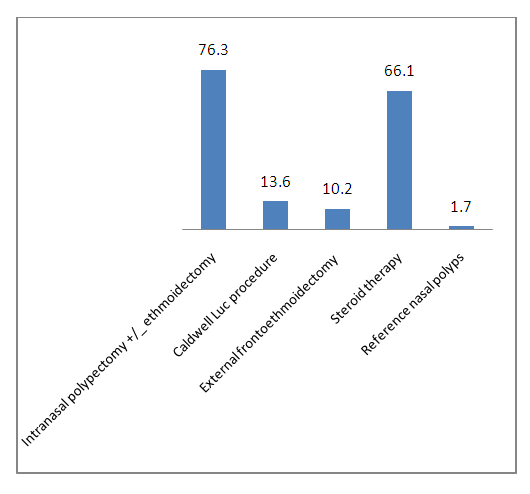 | Figure 3. Management of nasal polyps among patients |
4. Discussion
- In this study, prevalence of nasal polyps was 1.2%. This prevalence is low and this may be due to late presentation of our patients with sighted of protruding nasal masses and severe progressive nasal obstructions. In this part of the flu and stuffy nose are believed to be mild conditions and can be treated with home remedy or over the counter medication. Nasal polyps presentation affected all the studied age groups but peaked at middle-aged [12-14]. This may be due to chronic nature of this disorder with possible early pathology and late manifestation as observed in this study [15]. There was male dominance over female in this study as reported in other studies [16-18]. Female dominance was reported in other study [19]. Most of the patients were urban dwellers which may be due to industrial waste exposure, accessibility and affordability of health facilities. Nasal polyps are common among artisans, civil servants, farmers and businessmen due to their exposure in the course of daily activities [15]. This has profound effects on their work with associated inconvenience, absenteeism and discomfort [15]. Bilateral and unilateral nasal polyps with left nasal polyps commoner than right nasal polyps. Most of nasal polyps arises from ethmoid sinuses with similar report by other studies [20]. First episode is commonest than recurrent cases due to chronic nature of the disorder and recurrence resulted from inability to address the main aetiology which is idiopathic [15,16]. Wrong assumptions by the patients that the feeling were due recalcitrant flu which does not respond to common drugs made most of the patients to present after 3 months up to 10 years in our findings [15]. Only complicated rhinosinusitis including allergic rhinitis were referred to otorhinolaryngologist in our practice. There is need for prompt referral of longstanding flu to the specialist for expert review and management [21]. Multiple grapelike polyps arises from multiple ethmoid air cell while solitary antrochoanal polyps was single tantrum [16]. Ethmoid (simple) polyps were commoner than antrochoanal and nasal cavity polyps in this study and concomitant with findings from previous study [20].Patients with nasal polyps usually presents with associated comorbid illnesses in our findings which were chronic rhinosinusitis, allergic rhinitis and asthma [21,22]. This is the commonest reasons for late presentation of nasal polyps because it was wrongly regarded as common or normal catarrh even in out patients' complaints. Commonest complaint of our patients with nasal polyps in this study was fleshy growth in the nose others were nasal obstruction, Nasal discharge (rhinorrhea), hyposmia / anosmia, bout of sneezing and headache [23,24]. Due to late presentation there were associated destruction of the surrounding bones with polyps extension into the contiguous organ such as orbit, intracranial structures and postnasal space (choanal).Our treatment plans was to relieve nasal blockage, restore nasal function/olfaction, improve sinus drainage and improve patients quality of life. Our treatment of nasal polyps was a combination of medical and surgical interventions [25,26]. All our patients had obstructing nasal polyps at presentation and surgical treatment were offered. Surgical approaches were simple polypectomies with or without ethmoidectomies and external frontoethmoidectomies for Intranasal polyps. Caldwell Luc surgery was done for the antrochoanal polyps. Medical treatment for nasal polyps by intranasal corticosteroids was offered to some of the patients postoperatively to induce remission and prevent recurrence [27]. Patients were monitored over two years. There was a case of recurrence in a patient with intranasal adhesion.
5. Conclusions
- Nasal polyps are idiopathic common sinonasal chronic disorder. There is associated late presentation with longstanding progressive nasal obstructions. Longstanding progressive nasal obstructions should necessitate referral to otorhinolaryngologist. Follow up patients post treatment is advised for early detection of recurrence.
ACKNOWLEDGEMENTS
- The authors are most grateful to Ekiti state university teaching hospital, the staff and all the patients who participated in this study.
Funding
- There was no financial support. It is a self sponsored research study.
Competing Interests
- All the authors declare that there was no competing interests.
Ethical Consideration
- Ethical approval was obtained from the ethics and research committee of our institution.