-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Internal Medicine
p-ISSN: 2326-1064 e-ISSN: 2326-1072
2020; 9(1): 11-19
doi:10.5923/j.ijim.20200901.02

Cancer in Ife-Ijesha, Southwestern Nigeria: An Account of a 20- year Cancer Registration from Ife-Ijesha Cancer Registry
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAbidemi Omonisi1, Akinwumi Komolafe2, Olufemi Adefehinti3, Babatunde Olasode2, Oladejo Lawal4, Muheez Durosinmi5, Williams Odesanmi2
1Department of Anatomic Pathology, Ekiti State University, Ado-Ekiti, Ekiti State, Nigeria
2Department of Morbid Anatomic & Forensic Medicine, Obafemi Awolowo University, Ile-Ife, Osun State, Nigeria
3Department of Paediatrics & Child Health, Obafemi Awolowo University, Ile-Ife, Osun State, Nigeria
4Department of Surgery, Obafemi Awolowo University, Ile-Ife, Osun State, Nigeria
5Department of Haematology & Blood Transfusion, Obafemi Awolowo University, Ile-Ife, Osun State, Nigeria
Correspondence to: Abidemi Omonisi, Department of Anatomic Pathology, Ekiti State University, Ado-Ekiti, Ekiti State, Nigeria.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

BACKGROUND: The incidence of cancer is increasing worldwide and particularly in the sub-Saharan Africa as shown by cancer data published by World Health Organization. Nigeria like many countries in the West African region is experiencing an increase in cancer incidence, yet there is no centre exclusively devoted to cancer care and cancer research. It is said that environmental factors play a significant role in the causation of cancer, so it is important to know the pattern of cancer distribution in a specific geographical location.In Nigeria, there seems to be a changing pattern in the trends of some cancers during the last four decades. AIM & OBJECTIVE: The aim of the study is to describe the pattern of cancers seen in Ife-Ijesha zone, Southwestern Nigeria as recorded in the hospital-based Ife-Ijesha cancer registry between January 1991 to December 2010. The main objective of the study is to describe the pattern of cancer seen with reference to age, sex and site. MATERIALS AND METHODS: The study is a retrospective study of all cases of malignant tumour recorded in the Ife-Ijesha cancer registry which is located in the Department of Morbid Anatomy & Forensic Medicine of the Obafemi Awolowo University Teaching Hospitals Complex Ile-Ife, Nigeria between January 1991 and December 2010. RESULTS: The total number of cancers recorded in the 20 years period that met the inclusions criteria were 6405. Out of these, 3498 (54.6%) were seen in females while 2907 (45.4%) were seen in males. Total number of malignant tumours recorded in paediatric age group was 692 (10.8%). The common malignant tumours in males in order of decreasing frequency were prostate cancer, non-Hodgkin’s lymphoma, liver cancer and soft tissue sarcoma. In females, breast cancer was on top followed by cancer of the cervix, non-Hodgkin’s lymphoma, leukaemia and soft tissue tumours. There is an increasing trend in the incidence of breast cancer, prostate cancer and non-Hodgkin’s lymphoma. However, cervical cancer showed a decline. CONCLUSIONS: This study has shown a probable rising trend in the pattern of non-Hodgkin’s lymphoma recorded in Ife-Ijesha cancer registry. On the other hand, prostate cancer and cancer of the breast remained consistently the most frequent cancer in the males and females respectively. Lung cancer and Kaposi’s sarcoma that are commonly seen in the Northern and Eastern regions of Africa are rare in this study.
Keywords: Ife-Ijesha, Cancer Registry, Southwestern
Cite this paper: Abidemi Omonisi, Akinwumi Komolafe, Olufemi Adefehinti, Babatunde Olasode, Oladejo Lawal, Muheez Durosinmi, Williams Odesanmi, Cancer in Ife-Ijesha, Southwestern Nigeria: An Account of a 20- year Cancer Registration from Ife-Ijesha Cancer Registry, International Journal of Internal Medicine, Vol. 9 No. 1, 2020, pp. 11-19. doi: 10.5923/j.ijim.20200901.02.
Article Outline
1. Introduction
- Cancer is now the leading cause of death globally and the new global cancer data suggests that the global cancer burden has risen to 18.1 million cases and 9.6 million cancer deaths according to GLOBOCAN 2018 estimates [1-2]. Despite the commitment by the leaders in the developed countries in combating the scourge of cancer, most African leaders have not shown serious commitment in reducing the risk factors and disabilities attributable with the disease in the continent. Many Africa countries are struggling with cancer disease burden assessment with lack of adequate reliable data from cancer registries as well as mortality data from vital registration or verbal autopsies. It might seem that cancer should not be regarded as a priority in Africa because the continent continues to face challenges arising from sustained epidemics of infectious diseases [3]. Almost all the investment put into the continent’s health systems has been focused toward communicable diseases such as malaria, cholera, tuberculosis and HIV/AIDS [3].Unfortunately, cancer has already reached an alarming rate in most nations in Sub- Saharan Africa and mortality from the disease is now a major concern to the health practitioners in the region [4-5]. Coincidently, this region also has one of the highest incidence for HIV/AIDS and HIV/AIDS associated cancers [6-7], weak health systems [8], grossly deficit infrastructures[9], high out- of- pocket healthcare costs [10],critical shortage of healthcare workers [11] and lack of national cancer control programmes in many countries in the continent [12]. For close to four decades, the pattern of cancers recorded at Ibadan cancer registry at different periods were used to project for the distribution of cancers in Nigeria [13-16]. However, remarkable differences can be found in the distribution of cancers from one geographical location to another because environmental factors also greatly influenced the expression of cancers in a geographical environment even within same country [17-18]. The study of the geographical distribution of cancer has long been recognised to be one way of obtaining clues to its causation [19]. The Ife-Ijesha Cancer Registry (IICR) was established in 1989 and domiciled in the Department of Morbid Anatomy and Forensic Medicine of Obafemi Awolowo University Teaching Hospital, Ile-Ife, Osun State, Southwestern. Although, IICR has contributed data to few special publications, this is the first major publication from the registry since inception till date. This study analyses the profile of cancers and also an account of the first two decades of cancer registration in Ife-Ijesha, south-western Nigeria. This report will serve as the baseline for further publications that will emanate from the registry and also serves as basis for comparism with other data from other cancer registries.
2. Materials and Methods
- Study location: This study was carried out at the Ife-Ijesha cancer registry, located in the Department of Morbid Anatomic and Forensic Medicine Obafemi Awolowo University Teaching Hospitals Complex, Ile-Ife, Osun State, Nigeria from January 1991 and December 2010.Study Area: The registry is located and essentially covered the Ife-Ijesha senatorial zones that comprises of ten Local Government Areas with a heavy annual rainfall [20]. The 2006 last census conducted in the country puts the population of Ife-Ijesha at 1,265’491 [21] comprising 643,121 males and 622,370 females. This zone has the largest deposit of gold in Nigeria [22]. This population is in the Yoruba speaking area of South Western Nigeria. The dominant occupation and economic activities of the people centres around farming, agro-allied production, trading, artisanship, school administration, teaching and cottage industries. In additions, there are large academic community consisting of highly educated lecturers and non- academic staff in the Universities, Polytechnic and Colleges of Education. There are civil servants in the services of local, state and federal governments with numerous other corporate and private businesses. There are also, a Teaching Hospital and Missionary Hospitals, in the zone. The zone also enjoys the presence of commercial, development and community banks. The Ooni of Ife and the Owa Obokun of Ijeshaland are the notable paramount rulers in the zone. The zone is home to the famous and beautiful Erin Ijesha (Olumirin) waterfalls: a lavish acrobatic display of nature and a proud tourist attraction centre [22]. Study population: Six thousand four hundred and five (6405) of cancer cases recorded in Ife-Ijesha Cancer Registry was analyzed for this study.Study type: This is a retrospective study.Inclusion and exclusion criteria: All cancers that were confirmed morphologically and recorded in the Ife-Ijesha. Cases with incomplete biodata, all post-mortem diagnoses with prior ante-mortem diagnosis were excluded to prevent double data entrying and cases that are not confirmed morphologically in the cancer registry. Insitu carcinoma and all borderline tumours were excluded from this study. All cancers that satisfy the inclusion criteria were classified by topography based on organ and site according to International Classification for Diseases Oncology [23]. Data collection and Abstraction: The registry uses active method of case finding. Data sources within the hospital are visited weekly while data sources outside the hospital at the onset were visited monthly. The registry cytology and histology reports as well as death certificates as a basis of diagnosis. Methods: biodata of the patients such as age, tribe, religion, occupation, gender were noted and documented on the registry abstraction form. The abstraction form captures all the key variables, including the clinical history, tumour type and the incidence date. Each of the cancer was coded using the ICD-O coding system.Ethical clearance: Ethical approval for the study was obtained from the Hospital Research and Ethical Committee of Obafemi Awolowo University Teaching Hospital, Ile-Ife, Osun State, Nigeria.Statistical analysis: SPSS version 15.0 (SPSS, Inc.,Chicago, Illinois,USA) was deployed for the statistical analysis.
3. Results
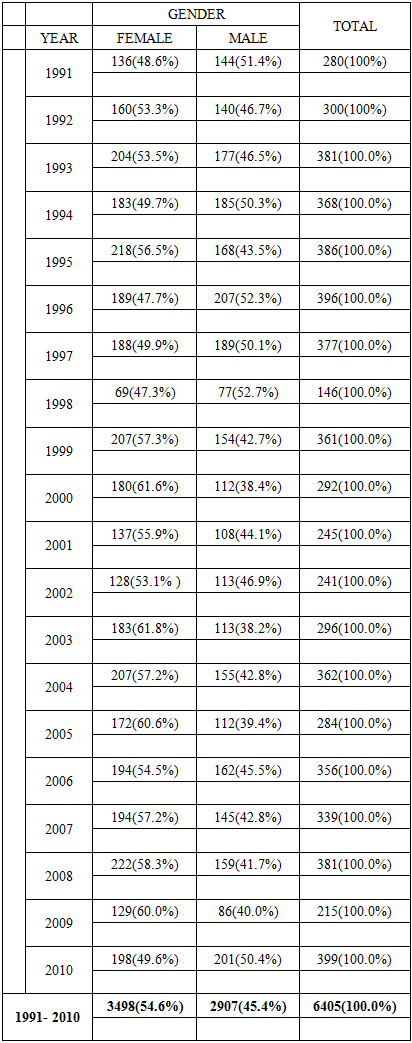
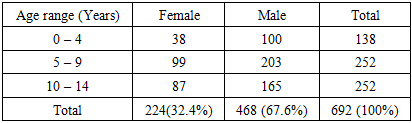
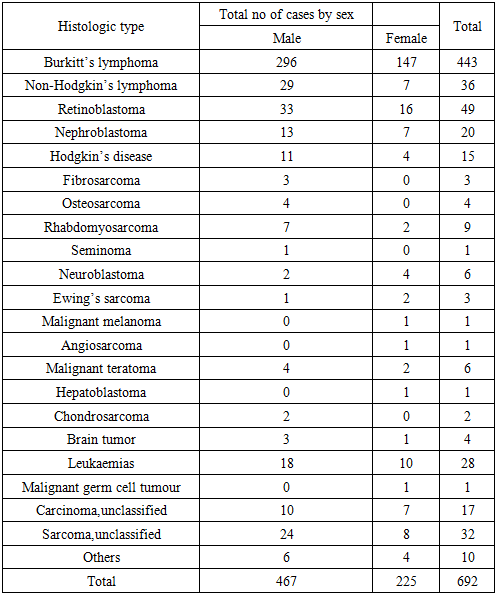
- A total of 6895 cancer cases were documented in the Ife-Ijesha cancer registry during the period under review. This gives an annual average of 345 cases. Of these, only 6405 cases met the inclusion criteria for this study.Of the 6405 patients, there were 3498 females and 2907 males as shown in Table 1.
|
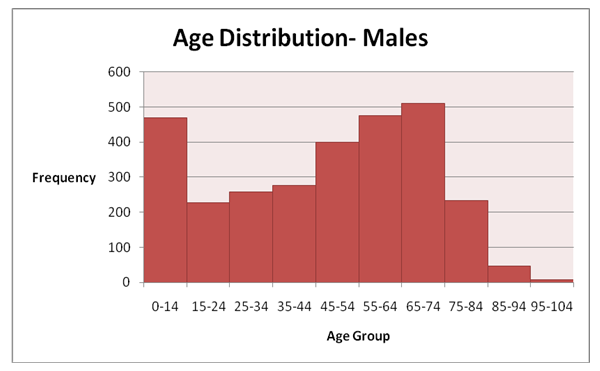 | Figure 1a. The incidence and age group distribution of male cases, 1991-2010 |
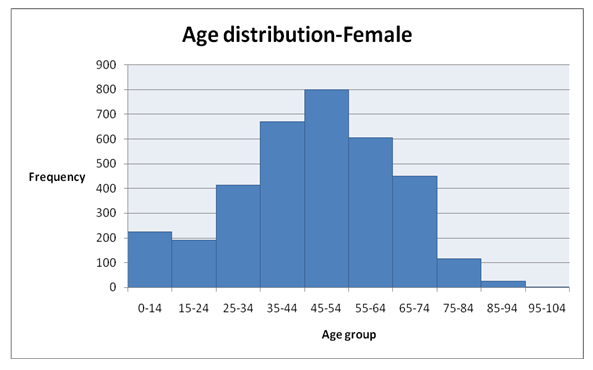 | Figure 1b. The incidence and age group distribution of female cases, 1991-2010 |
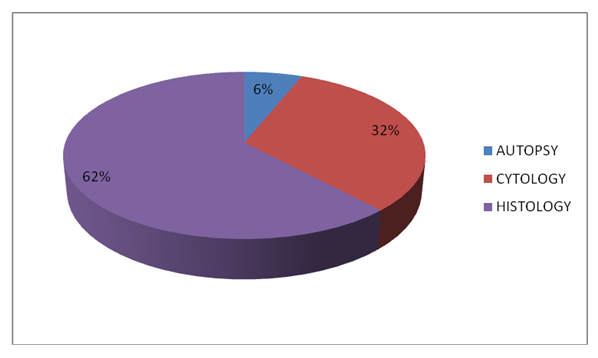 | Figure 2. A Pie Chart Showing the Basis of Diagnosis, IICR 1991-2012 |
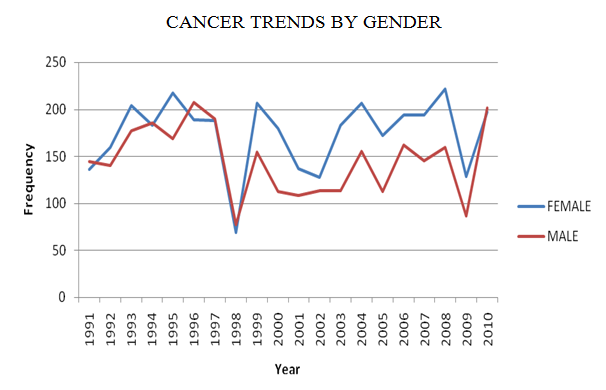 | Figure 3. Cancer Trends by Gender in Ife-Ijesa Cancer Registry (IICR), 1991-2010 |
|
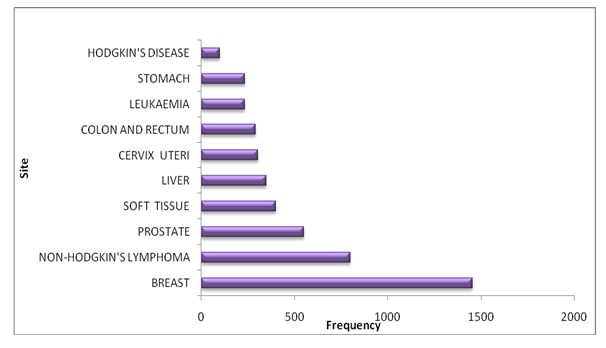 | Figure 4. The Bar Graph Showing Top Ten cancers in IICR: 1991-2010, ALL PERSONS |
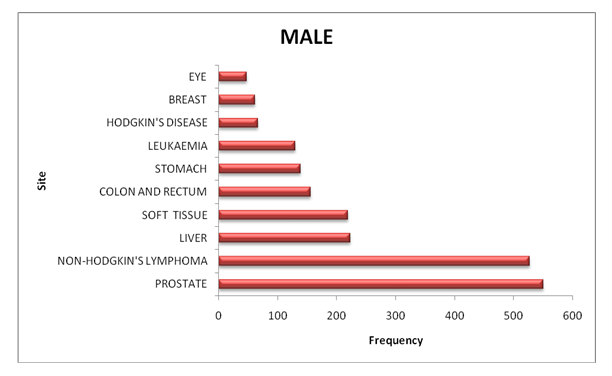 | Figure 5. The Bar Graph showing Top Ten cancer site in Male 1991-2010 |
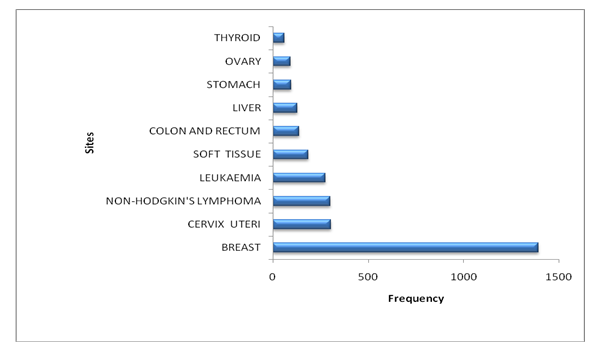 | Figure 6. The Bar Graph showing Top Ten cancers site in Female 1991-2010 |
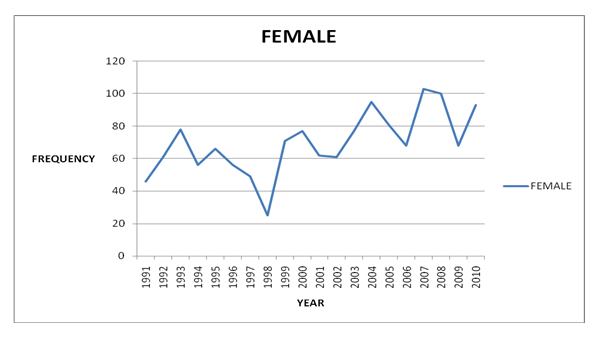 | Figure 7. Showing Trend of Breast Cancer in the Females, IICR, 1991-2010 |
|
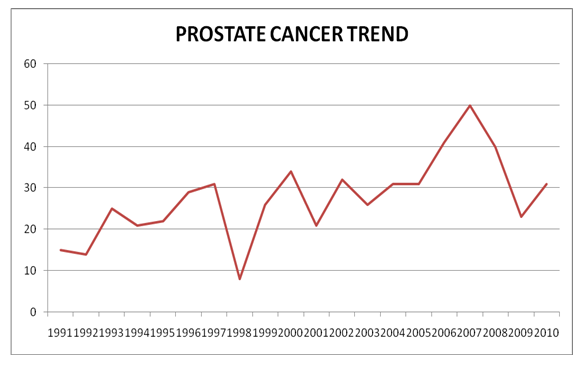 | Figure 8. Showing Trend of Prostate Cancer IICR, 1991-2010 |
|
4. Discussion
- Today, it is recognized that cancer is common in Africa, and it would be impossible to review briefly the extensive literature on cancer from this continent and the rest of the world. The incidence of all cancers is increasing all over the world and the increase is occurring more rapidly in regions that had hitherto enjoyed low incidence [24].In this study, the female to male ratio of the overall cancer incidence is 1.2:1. This shows a female preponderance. Most studies in Nigeria have shown a female preponderance. Edington and Maclean in their first publication on cancer rate survey in Nigeria reported a female preponderance [13]. Ogunbiyi et al 45 years after also reported a female preponderance from same cancer registry [25]. Earlier report by Ojo from the Ife-Ijesha cancer registry where this study was carried out showed a female preponderance over a three year period 1993-1995 with a female to male ratio as 1.13: 1 [26]. However, this contrasts with the finding of an earlier study by Mulligan in Ilesha Southwestern Nigeria. He reported a male preponderance with female to male ratio as 1:1.1 [27]. When Mulligan carried out his study in the late 60s, women in Nigeria were not as emancipated even in the southern part of Nigeria as they are now. This was probably why he reported a male preponderance. In the traditional African societies, the males are more visible than the females. This was even more so before the period of women emancipation in Nigeria although, in different parts of the country, cultural, religious and even tribal norms dictate different levels of emancipation for women, as well as whether they have a liberal or conservative social and political orientation. Overall, most studies in Nigeria have reported female predominance, this is because females are likely to seek medical care more easily than the males who are the breadwinners of their families and are more highly mobile, most of them will only present in the hospitals if their health conditions have severely deteriorated. In additions, the females usually attend the hospitals when they are pregnant for antenatal care and during the postnatal period. During these periods, they are screened and educated on health issues. The females are usually responsible for taking the children to the hospitals. All these make the females more hospital friendly and more likely to seek medical care than the males.Increasing trends in the annual reported cases of cancer have been documented in various studies [28-31]. When the annual average of cancer cases recorded in this study is compared with the earlier study by Mulligan in this environment, it can be suggested that there is about a ten times increase in the annual average of cancer in Ife-Ijesha Zone. When Mulligan carried out his study, Wesley Guide Hospital Ilesha was the only major hospital in the zone. Presently, there are more hospitals in the zone with improvement in the diagnostic facilities in the major hospitals; these hospitals are the Ife and Ilesha Hospital Units of the Obafemi Awolowo University Teaching Hospitals Complex and the Seventh Day Adventist Hospital Ile-Ife (a missionary hospital).It was also observed that the zone is increasingly being urbanized and the numbers of industries, banks, tertiary institutions of learning and fast food centres have increased remarkably over the decades with concomitants change in the lifestyles of the people. Forbes in 1997 documented in the English Literature that the gradual increase in the incidence of cancer globally from public health perspective, may be traceable to the increasing cancer awareness campaigns, changing lifestyles including diets, urbanization, improvement in diagnostic facilities, availability of specialist medical care and many as yet unknown factors [32]. Paediatric cancersWith respect to paediatric cancers, the pattern seen in this study compared favourably well with reports from other centres in Nigeria and other nations in Africa. The findings in this study are consistent with the findings in Ibadan [33], Lagos [34], Ghana [35] and Western Kenya [36]. The peak incidences of paediatric cancers were in the age-groups 5-9 and 10-14. In Ibadan, the majority of cases were seen between the ages 5 and 10 years [33]. This is similar to the finding in Lagos [34].This study showed that Burkitt’s lymphoma remained the commonest paediatric cancer in Ife-Ijesha zone of Osun state. This finding agrees with the those of other studies reported in other parts of Nigeria [33-34,37] which have shown an increasing trend in the incidence of Burkitt’s lymphoma except in Ibadan where the relative frequency has dropped over time [38]. It might appear as if the current control mechanisms in the prevention and control of Burkitt’s lymphoma are not effective. This trend is most likely to continue in West and East Africa, unless effective control measures are instituted to reduce the high prevalence of Epstein-Barr virus and malaria endemicity in these sub-regions [39]. Epstein-Barr virus (EBV) is widely accepted as a major contributor to the high incidence of endemic Burkitt’s lymphoma in Africa and is detected in about 95% of endemic Burkitt’s lymphoma cases [40].Commentary on The Leading Cancers in this study in Males and FemalesBreast cancer belongs to the group of cancers that are potentially curable if diagnosed early, unfortunately in Nigeria, most cases presented during the late stage of the diseases [41]. Overall, the dominant malignancy in this present study is cancer of the female breast. The trends for breast cancer varied markedly between 1991 and 2010. However, we observed steady rise in the incidence of breast cancer in this study with occasional declines which coincide with the period of national and local industrial unrest when public health facilities were closed. This finding is consistent with the finding of Afolayan et al from Ilorin who reported a steady rise in the incidence of breast cancer in their series [42]. This indicates that the existing control measures to stem the incidence of breast cancer in Nigeria are not effective. Thus there is need to review these control measures for better results. Some reports from the developed countries have shown that the large part of increase in the incidence of breast cancer parallels the increase in the use of screening mammography which detects breast cancer at an earlier stage [43-44]. However, this explanation might not account for the increasing trend recorded in this study because mammography machine was only introduced in this centre in 2010. The increase observed in this study may be postulated to be due to increased awareness and presentation for screening, and also the presence of the established risk factors for breast cancer. The established risk factors for breast cancer in Nigeria documented in the English Literature are, age at first full term pregnancy, parity, breastfeeding,age at menarche, adoption of western lifestyle and age at menopause[45]. The results of this study show an alarming high percentage (about 35%) of young women aged less than 44 with breast cancer. Some of these cases were in their twenties. The increasing prevalence of breast cancer among the young population could be due to the use of oral contraceptives, and increasing exposure to several reproductive risk factors such as age at menarche, parity and age at first full term pregnancy [46].In this study, 62 cases of male breast cancer were seen representing 4.3% of all the breast cancer cases seen in both sexes. This is higher than the 1% recorded from other parts of the world [47-48]. In a cancer survey conducted by Mulligan in Ilesha, Southwestern Nigeria in 1970; no case of male breast cancer was recorded in his study. Ezeome et al from Enugu Eastern Nigeria, Kidmas et al from Jos North Central and Oguntola et al from Osogbo South Western and Aghadiuno also from South Western Nigeria reported that male breast cancer constitute 2%, 8.6%, 8.86% and 3.4% of all breast cancers in their series [49- 53]. The higher figures in these studies may be due to small sample size, since this data is from hospital based survey. Cancer of the prostate is the most common cancer among men in Nigeria [54].. In this study, the trends for prostate cancer indicated a steady rise since the early 90s. This finding is consistent with the reports based on GLOBOCAN 2018, which also reported cancer of the prostate as the most frequent cancer in the males in Europe, America, Southern Africa and some nations in West Africa [2]. According to the Globocan 2018 which is the latest global cancer estimates of incidence and mortality, lung cancer still topped the list as the most common cancer in the world in both sexes combined 2. However, in this study, only 10 cases of lung cancers were recorded over the 20 years period of this study. The few cases recorded may be due to absence of specialist pulmonary surgeon in the centre mostly during the study period but pulmonary surgeons are now available in the centre. It is hoped that more cases will be picked up in the near future. However, this finding is in contrast to the reports from the Northern Africa where lung cancer tops the list of the most frequent cancers in the males [2,55]. Cigarette smoking has been shown as a major cause of lung cancer in the Northern Africans [56].
5. Limitations of This Study
- There are many difficulties in the accurate enumeration of cancer cases from a defined population in the developing countries such as Nigeria. The data used in this study are mostly hospital-based and retrospective study with propensity for bias. Unavoidable bias as a result of facilities available, special interests or referral trends may occur. Some types of cancer may be overrepresented and others underrepresented.
6. Conclusions
- This study has confirmed that cancers are not rare in Africa and that it is important to monitor cancer trends in any population all over the world. Geographical cancer surveys have become a recognized method for elucidating the factors involved in the genesis of neoplasms. Such surveys are particularly valuable in describing the incidence and pattern of cancers in a geographical location.Although the data presented in this study are derived from a hospital based cancer registry, it is obvious that cases of cancer recorded are increasing and some of the common cancers are preventable or potentially curable if detected early. This study also reveals that breast and prostate cancers still top the list of most common cancer in the females and males respectively while others such as lung and Kaposi’s sarcoma enjoy low incidence in the study area. Establishing and running a cancer registry is tedious and challenging. The Ife-Ijesha cancer registry was designed as a population-based registry, but due to shortage of staff and financial constraints, it is currently operating as a hospital-based registry. There is need for the Governments at all levels and institutions to support the existing cancer registries in the country to ensure timely reporting of cancer data.
ACKNOWLEDGEMENTS
- We thank Mr. Bamigbetan Olajide, the Registrar of Ife-Ijesha Cancer Registry for his commitment to cancer registration in Ife-Ijesha population and Mrs Olorunlana Mosunmola, the computer and data manager of Ife-Ijesha Cancer Registry for her efforts in entering the data of these cancer patients into the computer over these years.