Ngongang Ouankou Christian1, 2, 3, Tsambang Djeufack Wilfried Lionel4, Eyoungou Lucien Roger5, Azabji Kenfack Marcel2, Mbouh Samuel5, Wandji Ngamga Christiane Josée1, Kuate-Mfeukeu Liliane2, Mekoulou Jerson3, Bitchou Marie Philomène1, Tachim Ngatchouissi Kevin4, Essono Naah Annabelle Clotilde4, Chendjou Kapi Léana Oriane6, Nganou Chris Nadege1, Hamadou1, Jonte Mbianda Klod Paturelle1, Tikapa Joachim2, Tchuisseu Larissa2, Kenfack Monique1, Ndongo Amougou Sylvie2, Boombi Jérôme2, Kaze Folefack François Jérôme1, Ouankou Mérimée Débozard7, Kingue Samuel2, Ngu Blackett Kathleen2, Mandengue Honoré Samuel3
1Internal Medicine and Specialities, Yaounde University Hospital Center, Cameroon
2Faculty of Medicine and Biomedical Sciences, University of Yaounde I, Cameroon
3Douala University, Faculty of Sciences, Cameroon
4Higher Institute of Medical Technology Nkolondom Yaounde, Cameroon
5National Institute of Youth and Sport Yaounde, Cameroon
6Université Des Montagnes, Institut Supérieur des Sciences de la Santé (ISSS), Cameroon
7Centre de Cardiologie et Médical, Cameroon
Correspondence to: Ngongang Ouankou Christian, Internal Medicine and Specialities, Yaounde University Hospital Center, Cameroon.
| Email: |  |
Copyright © 2018 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Background: Sporting discipline is acknowledge to be an influential factor on the aspects of cardiac adaptation encountered in the athlete’s heart syndrome. Little focus is carried to determine its influence on athletes of black ethnicity. Taking in consideration their unspecified training pattern, our study aimed at bringing out its impact on Cameroonian athletes. Methods: Was conducted a prospective cross sectional study, enrolling athletes trained at the NIYS of Yaounde, with their ages from 20 to 35 years and having at least a year duration at high intense practice. The disciplines included were Basketball, Football, Handball, Martial arts and Volleyball. Were excluded from the study all pregnant, breast feeding women and subjects with cardiovascular diseases. Ethical clearance and administrative authorization were obtained. Data was collected after an individual signed informed consent. Data compilation was done using CSPro version 6.0 and analysis done with SPSS version 20 and Microsoft Excel 2010. The Chi square test for comparison of proportions, the ANOVA test (analysis of variance) and student test for comparison of means. Statistical significance was set at p = 0.05. Results: 151 athletes were enrolled, 43.05% female and 56.95% male athletes for a male to female gender ratio of 1.3:1 and a mean age was 25.87±3.33 years. Anthropometric parameters differences in women showed statistical significance for body weight 75,5 ± 8,6 (p=0.04), body surface area 1,80 ± 0,13 (p=0.01) and BMI 28,1 ± 2,7 (p=0.04) in the martial arts discipline. No statistical significance was demonstrated in men for anthropometric parameters. The slowest heart rated differences were not significant for both genders between the different sporting disciplines. Abnormal repolarization pattern was statistically significant in men among the sporting disciplines (p= 0.04). No statistical significance was noted in women echocardiographic patterns. We noted a random distribution of highest values. LVEDD/BS (28.7 ± 3.5), LVESD/BS (17.7±3.0), IVC exp/BS (14.2±0.1) and IVC insp/BS (11.9±0.6) were highest in Basketball; for IVSd/BS (5.21±0.8) and LVEF (72.9±8.2) in Handball; for LVWTd/BS (4.5±1.4) and E/A ratio (2.2±0.1) in Football; for LAD/BS (22.1±2.4), LA area (20.7±4.1) and RVEDD/BS (10.5 ± 2.3) in Martial arts and AoD/BS (14.1±2.5) and TAPSE (16.7 ± 2.3) in Volleyball. We noted a random distribution of highest values for echocardiographic parameters in men. Highest recorded values for LVEDD/BS (27.4±2.5), LVESD/BS (17.2 ± 3.1), LVWTd/BS (4.7±1.0), LAD/BS (16.1±1.7), LA area (20.8±4.7), RVEDD/BS (12.7 ± 2.6), IVC exp/BS (12.7 ± 2.3), IVC insp/BS (7.7 ± 2.3) and AoD/BS (16.1±1.7) were in Football; for IVSd/BS (6.0±1.4), TAPSE (16.3 ± 2.8) and E/A ratio (2.2 ± 0.6) in Volleyball and LVEF (71.5 ± 7.3) in Handball. The only statistically significant value was for AoD/BS (p=0.006) in Football. Conclusion: More precisions on the Athletes heart syndrome are obtained from this study. The influence of unspecific training regime applied in our study population was demonstrated. The striking ECG abnormalities demonstrated in black athletes was not attributed to any sporting discipline. We could not demonstrate any significant adaptation changes between athletes of the same gender from different sporting disciplines.
Keywords:
Sporting discipline, Athlete’s heart syndrome, Gender, Cameroon
Cite this paper: Ngongang Ouankou Christian, Tsambang Djeufack Wilfried Lionel, Eyoungou Lucien Roger, Azabji Kenfack Marcel, Mbouh Samuel, Wandji Ngamga Christiane Josée, Kuate-Mfeukeu Liliane, Mekoulou Jerson, Bitchou Marie Philomène, Tachim Ngatchouissi Kevin, Essono Naah Annabelle Clotilde, Chendjou Kapi Léana Oriane, Nganou Chris Nadege, Hamadou, Jonte Mbianda Klod Paturelle, Tikapa Joachim, Tchuisseu Larissa, Kenfack Monique, Ndongo Amougou Sylvie, Boombi Jérôme, Kaze Folefack François Jérôme, Ouankou Mérimée Débozard, Kingue Samuel, Ngu Blackett Kathleen, Mandengue Honoré Samuel, Athlete’s Heart Syndrome Variability with Respect to Sporting Disciplines in Elite Cameroonian Athletes, International Journal of Internal Medicine, Vol. 7 No. 1, 2018, pp. 8-15. doi: 10.5923/j.ijim.20180701.03.
1. Introduction
The influence of sporting disciplines on the aspects of cardiac adaptation have been demonstrated by numerous studies [1-4]. Other influential factors such as: age, gender and ethnicity also show substantial impact on the magnitude of cardiac adaptation [5-9]. A classification of sports is provided by the Mitchell’s classification, which relates two general component of exercise: dynamic and static demands [10-12]. Each sport is categorized with respect to their level of intensity (low, medium, high) of dynamic or static exercise generally required to perform that sport during competition. This sports matrix should not be regarded as a rigid classification, but rather a spectrum in which some athletes from same sporting discipline could possibly deserve placement in different categories. Furthermore, some sports involve heterogeneity with respect to static and dynamic cardiovascular demands in different athletic disciplines. Such as parallel bars and floor exercises in gymnastics or positions of lineman or running back in football, or goalkeeper and mid-fielder in soccer. These distinctions are not formulated in the classification, but should be taken into consideration. Striking electrocardiographic (ECG) abnormalities encountered in black athletes are considered as an ethnic variant of the athlete’s heart syndrome [13, 8, 9]. Thus, it was of importance to determine how these striking ECG abnormalities are distributed throughout the different sporting disciplines practiced. In this study we sought to demonstrate differences in cardiac adaption between athletes of similar genders from different sporting disciplines in black athletic population from the Cameroon.
2. Methods
Subjects We carried out a prospective descriptive cross sectional study on athletes from the National Institute of Youth and Sport (NIYS) at Yaounde. Ethical clearance was obtained from the Douala University Institutional Ethic Committee. Were included athletes with ages from 20 years and below 35 years of both genders and practicing high intensity regular physical activity of at least a year duration at high level. Were excluded from the study those who did not sign an inform consent, those with past history of cardiovascular diseases and pregnant or breast feeding athletes. We conducted a non-exhaustive consecutive sampling in five sporting disciplines.Study procedure A questionnaire on socio-demographic data (age and sporting discipline) administered to everyone who concern to participate. Then, clinical and para-clinical data collected. It consisted in the measurement of weight; height; blood pressure [14, 15]; cardiac auscultation; electrocardiographic tracing [16-18] and Doppler echocardiographic assessment ratio [19, 13]. They were collected following standard procedures. Indexed data collected at ECG evaluation were rhythm (sinus bradycardia), first-degree atrio-ventricular block, incomplete right bundle branch block, isolated QRS voltage criteria for LVH, T-wave inversion, ST-segment depression, left atrial enlargement, left axis deviation/left anterior hemiblock, right axis deviation/left posterior hemiblock, Ventricular premature contractions, complete left or right bundle branch block. Indexed data for Doppler echocardiography were for morphologically: LVEDD/BS, LVESD/BS, IVSd/BS, LVWTd/BS, LAD/BS, AoD/BS, LA area, RVEDD/BS, RV area, IVC exp/BS, IVC insp/ BS and functionally: TAPSE/BS, LVEF and E/A.Statistical analysis The data entry sheet was developed with CSPro version 6.0 software. The data from the validated questionnaires was entered, cleaned and analysed using SPSS version 20 and Microsoft Excel 2010. Quantitative variables are expressed as mean ± standard deviation. Meanwhile, qualitative variables were expressed as effective and percentages. The Chi square test for comparison of proportions, the ANOVA test (analysis of variance) and student test for comparison of means. Statistical significance was set for P value less than 0.05.
3. Results
3.1. General Characterization of the Study Population
3.1.1. Demographic Characterization
We enrolled 151 athletes with 86 (56.95%) male and 65 (43.05%) female, for a male to female sex ratio of 1.3:1. The mean age was 25.87±3.33 years. The practiced sporting disciplines were Basketball, Football, Handball, Martial arts and Volleyball. The study population distribution in the different sporting disciplines is represented in figure 1 below. The most represented male participants were from the Football discipline and for women from the Handball discipline.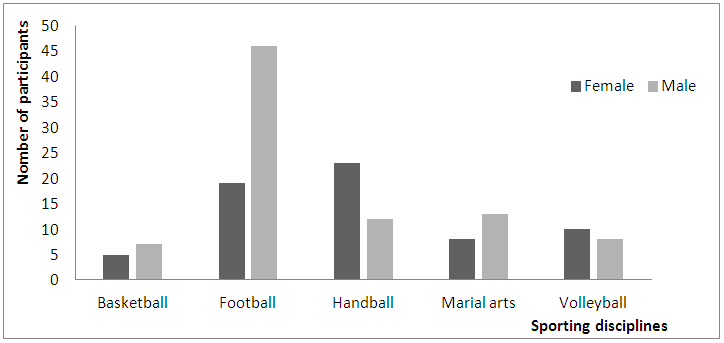 | Figure 1. Genders distribution in each sporting discipline |
3.1.2. Anthropometric Parameters between Genders from Different Sporting Disciplines
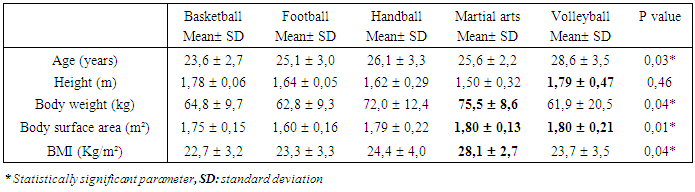
a) Anthropometric parameters between female genderTable 1. Female anthropometric parameters differences
 |
| |
|
Table 1 represent anthropometric parameters differences among women. Was noted from Volleyball the highest height (p=0.46); from Martial arts the highest body weight (p=0.04), body surface area (p=0.01) and BMI (p=0.04). b) Anthropometric parameters between male genderTable 2. Male anthropometric parameters differences
 |
| |
|
Table 2 represent anthropometric parameters differences among men. Was noted from Basketball the highest height and highest body weight; from Martial arts the highest body surface area and BMI. All were statistically not significant.
3.2. Differences between Sporting Disciplines for Same Gender
3.2.1. Electrocardiography Data Differences
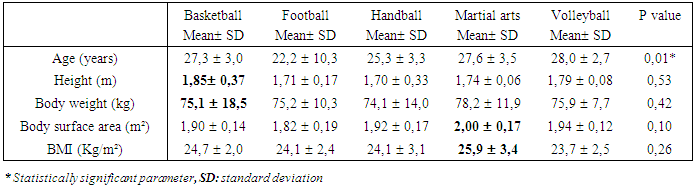
a) Heart rate variation in different sporting disciplines with respect to genderThe slowest heart rated in the female population was recorded in Football and the fastest heart rate recorded in Handball. The slowest heart rate in the male population was recorded in Volleyball and the fastest recorded in Handball. These results show no statistical significance as presented in table 3 below.Table 3. Heart rate pattern in the different sporting disciplines
 |
| |
|
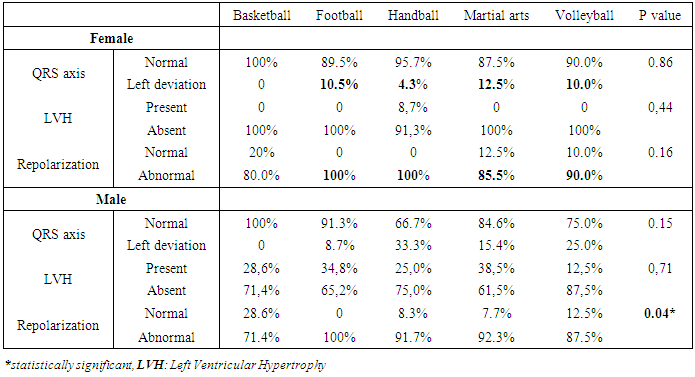
b) Differences in electrophysiological parameters in female athletes Bradycardia (HR ≤ 60 b/m) was recorded in 4 (17.4%) Handball players; 2 (20%) Volleyball players and 3 (15.8%) Football players. Premature contractions were recorded in Football players, 1 (4.3%) PJC and 1 (4.3%) PAC and in one (4.3%) Handball player with a PVC. Prolong P-R interval was recorded in one (20%) Basketball player and 1 (5.3%) Football player. No bundle branch block was noted in all the discipline. Posterior hemi-blocks were recorded in one (12.5%), 1 (10%), 1 (5.3%) and 1 (4.4%) athletes from Martial arts, Volleyball, Football and Handball respectively. Atri-ventricular block was noted in one (5.3%) Football player and from no other discipline. c) Differences in electrophysiological parameters in male athletes Bradycardia with HR ≤ 60 b/m was recorded in 6 (46.2%) Martial arts; 19 (41.3%) Football; 4 (33.3%) Handball; 2 (28.6%) Basketball and 2 (25%) Volleyball athletes. Premature contractions were recorded in Volleyball players, 1 (12.5%) PVC, 1 (2.2%) PAC and in a Football player 1 (2.2%) PVC. Prolong P-R interval was recorded in 2 (28.6%) Basketball; 1 (12.5%) Volleyball; 4 (8.7%) Football and 1 (8.3%) Handball players. Negative P wave was recorded in one (8.3%) Handball athlete. Left atrial hypertrophy (high amplitude P wave>3mm) were recorded in one (12.5%) Volleyball player (statistically significant with p=0.04). P wave without QRS was recorded in one (12.5%) Volleyball player (statistically significant with p=0.04). Right bundle branch block was recorded in 2 (16.7%) Handball; 1 (12.5%) Volleyball; 1 (7.7%) Martial arts and 1 (2.2%) Football player. Posterior hemi-blocks were recorded in 4 (33.3%) Handball and anterior hemi-block recorded in 2 (25%), 1 (7.7%) and 3 (6.5%) athletes from Volleyball, Martial arts and Football respectively. Atri-ventricular block was recorded in 1 (2.2%) Football player and in no other discipline. 3.2.1.1. Morphological Electrocardiographic Pattern for Same Gender in Different Sporting DisciplinesTable 4. Female and male morphologic and functional differences in sporting disciplines
 |
| |
|
From the female gender all the Football and Handball athletes had abnormal repolarization and LVH was noted only in 2 (8.7%) Handball athletes. QRS axis deviation was the least represented alteration in all the disciplines. No statistical significance was noted. Form the male gender abnormal patterns were mostly recorded in Football players, followed by Martial arts, Handball, Volleyball and Basketball athletes respectively. No statistical significance was noted, except for repolarization pattern which was statistically significant (p=0.04).
3.2.2. Transthoracic Echocardiographic Differences between Sporting Disciplines
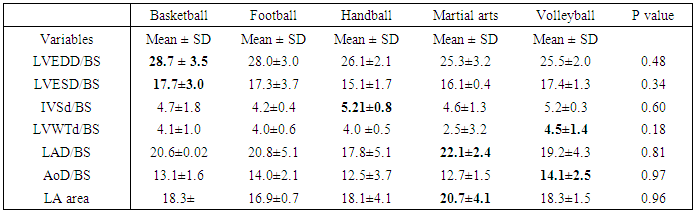
3.2.2.1. Left Cavities Morphological Differencesa) Difference in the female gender Table 5. Female left cavities morphological differences
 |
| |
|
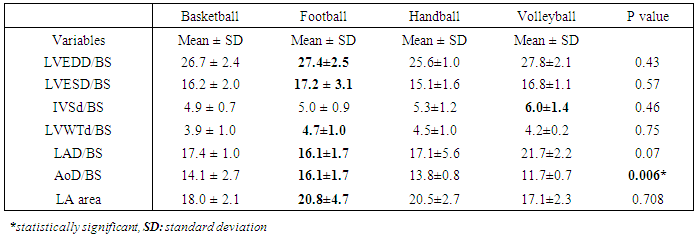
In Table 5 above, the greatest LVEDD/BS and LVESD/BS were recorded in Basketball; IVSd/BS recorded in Handball; LVWTd/BS and AoD/BS were recorded in Volleyball and LAD/BS and LV area were in Martial arts. All were statistically not significant.b) Differences in male gender Table 6. Male left cavities morphological differences
 |
| |
|
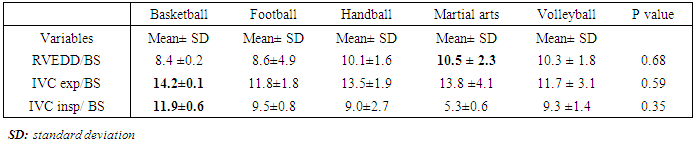
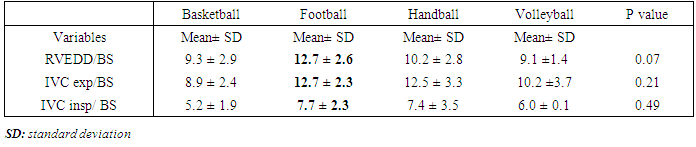
The greatest dimension were recorded in Football. Exception for IVSd/BS which was greater in Volleyball. The only statistical significant difference was recorded for AoD/BS as shown in table 6 above.3.2.2.2. Right Cavities Morphological Differences Table 7 and 8 respectively represent female and male right cavity morphological difference between the sporting disciplines.Table 7. Female right cavities morphological differences
 |
| |
|
Female athletes’ greatest dimensions were recorded for RVEDD/BS in Martial arts, IVC exp/BS and IVC insp/ BS in basketball. All being statistically not significant.Table 8. Male right cavities morphological differences
 |
| |
|
The highest dimensions for male athletes were recorded in Football. All were statistically not significant.3.2.2.3. Cardiac Functional DifferencesNo clear tendency is demonstrated. This is shown in table 9 and 10 respectivelyTable 9. Female functional cardiac differences
 |
| |
|
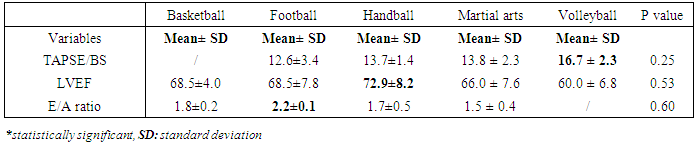
Functional cardiac parameters for female athletes were highest for LVEF values in Handball and E/A ratio in Football. All were not statistically significant.Table 10. Male functional cardiac differences
 |
| |
|
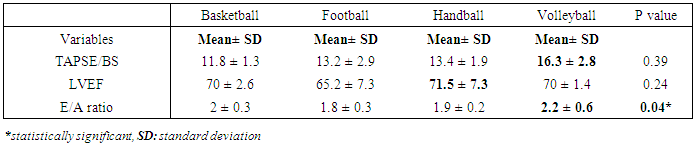
TAPSE/BS dimensions were highest for male Volleyball athletes; LVEF in Football athletes (statistically not significant) and E/A ratio highest for male Basketball athletes, which was statistically significant.
4. Discussion
In this study were included 151 athletes from both genders and sporting disciplines. The male athletes represented 56.95% and female athletes 43.05% of the study population. The mean age was 25.87±3.33 years. There was a morphological variation in the study population, for Basketball and Volleyball we noted thin; tall athletes of large body surface area and small BMI. For Football and Handball we noted short and thin athletes of small body surface area and BMI and for Martial arts we noted tall; fat athletes, of large body surface area and obese (mean BMI 28.1 kg/m2) for female athletes, while in overweight (BMI 25.9 kg/m2) for male athletes. All these parameters were statistically significant in the female population but none were significant in the male population. This results are similar to those from Baylos I et al who conducted a study on Greek female athletes from Basketball, Volleyball and Handball. He reported that, anthropometric variables varied among sporting disciplines [20]. This variation in anthropometric parameters can be as a results of the differences encountered in the body segments involved for the practiced each sporting discipline. The morphological adaptation to physiologic demands by the muscles engaged in the discipline lead to the recorded differences. Also, it can be due to selection criteria use in recruiting athletes in the sporting disciplines. People are selected in sporting disciplines according to their specific morphology. The sporting discipline in which was recorded the highest frequency of electrocardiographic alterations was Football (II C), both for female and male athletes. This can be explain from the fact it had the highest number of participants for both genders. The discipline with the least alterations was Volleyball (I B) this can be explained by its low level in static and moderate level in dynamic activity. Repolarization pattern was abnormal for all the Football and Handball (III A) female athletes and the least alteration were noted in Basketball (III A), meanwhile it shares the same class to Handball in the Mitchell classification. It can be due to the fact few basketball players participated to the study. For male athletes, in Football (II B), Handball (II C) and Martial arts (III A) was noted the greatest percentages of abnormal repolarization patterns. Martial arts athletes presented with more LVH than the other, which correlate to its level of static training. Our results are different from those obtained in previous studies, like that from Maaike G et al, who studied on 641 Caucasian athletes from 22 different sporting disciplines. Their results showed there were marked cardiac adaptation differences between athletes from different sporting disciplines [21, 22]. There were no marked differentiations in echocardiographic values for cardiac morphology and functions. For each echocardiographic parameter from the different sporting disciplines we had a random distribution of highest values. These results do not correlate to previous studies. Spirito P et al who studied on a sample of 947 athletes from 27 different sporting disciplines and reported that, sports differs greatly with regard to their impact on cardiac dimensions and that, dynamic activities are associated to greater dimensions [1]. The results obtained were not explained from the fact that in our study population of athletes from the NIYS training individualized (precise to any sporting discipline). Athletes follow similar training courses with no relation to their specific sporting discipline. Hence, the actual static and dynamic component of each discipline were not respected. An example was training regimens with heavy resistance weight (high static and low dynamic demand) to increase strength and power for sporting disciplines that do not involve such heavy static demands. This can explain why the resultant cardiovascular adaptation pattern does not show clear distinctions among the sporting disciplines.
5. Conclusions
Our study on highly trained Cameroonian athletes of both genders and from different sporting disciplines showed no mark cardiac adaptation differences. The influence of unspecific training regime applied in our study population was demonstrated. In this study the striking ECG abnormalities demonstrated in black athletes could not be attributed to any sporting discipline. However, except for the abnormal repolarization pattern on electrocardiographic tracing which were present in all Football athletes (both male and female), we could not demonstrate any significant adaptation changes between athletes of the same gender from different sporting disciplines. In this study the striking ECG abnormalities demonstrated in black athletes could not be attributed to any sporting discipline.
ACKNOWLEDGMENTS
We are thankful to the athletes who participated to this study and all the supportive staff of the National Institute of Youth and Sports. N.O.C, T.D.W.L, E.L.R, N.B.K and M.H.S designed the study. N.O.C, T.D.W.L T.N.K and E.A collected data. N.O.C, T.D.W.L and W.N.C.J carried out the statistical analysis. N.O.C and T.D.W.L drafted the article and interpreted the analysed data. All authors read and approved the final version.
References
| [1] | Spirito P, Pelliccia A, Proschan M, Granata M, Spataro A, Bellone P, Caselli G, Biffi A, Vecchio C, Maron B, “Morphology of the 'Athlete's heart' assessed by echocardiofraphy in 947 elite athletes representing 27 sports,” Am. J. Cardiol, vol. 74, no. 8, pp. 802-808, 1994. |
| [2] | D'Andrea A, Riegler L, Golia E et al, “Range of right heart measurements in top-level athletes: the training impact,” Int. J. Cardiol, 2011. |
| [3] | Luijkx T, Cramer M, Prakken N et al, “Sport category is an important determinant of cardiac adaptation: an MRI study,” Br. J. Sports. Med., 2012. |
| [4] | Dudzié A, Menanga A, Hamadou B, Kengne P, Atchou G, Kingue S, “Ultrasoonographic study of the left ventricle function at rest in a group of highly trained black African handball players,” Eur J Echocardiography, vol. 8, 2007. |
| [5] | Makan J, Sharma S, Firoozi S, Whyte G, Jackson P, Mckenna W, “Physiological upper limits of ventricular cavity size in highly trained adolescent athletes,” Heart, no. 91, 2005. |
| [6] | Sharma S, Maron B, Whyte G, Firoozi S, Elliott P, Mckenna W, “Physiologic limits of left ventricular hypertrophy in elite junior athletes: relevance to differential diagnosis of athlete's heart from hypertrophic cardiomyopathy,” J. Am. Coll. Cardiol, no. 40, 2002. |
| [7] | Pelliccia A, Maron BJ, Culasso F, Di Paolo F, Spataro A, Biffi A, Caselli G, Piovano, “Clinical significance of abnormal electrocardiographic patterns in trained athletes,” Circulation, vol. 102, no. 3, p. 278–84, 18 july 2000. |
| [8] | Basavarajaiah S, Boraita A, Whyte G et al, “Ehtnic diffeerences in left ventricular remodeling in highly-trained athletes: relevance to diffferetiating physiologic left ventricular hypertrophy from hypertrophic cardiomyopathy”, J. Am. Coll. Cardiol, no. 51, 2008. |
| [9] | Rawlins J, Carre F, Kervio G et al, Ethnic differences in physiological cardiac adaptation to intense physical exercise in hghly trained female athletes, Circulation, no. 121, 2010. |
| [10] | Gallagher K, Raven P, Mitchell J, “Classification of sports and the athlete's heart,” In: Williams R, 1999. |
| [11] | Asmussen E, “Similarities and dissimilarities between static and dynamic exercise,” Circ Res, 1981. |
| [12] | Mitchell J, Wildenthal K, “Static (isometric) exercise and the heart: physiological and clinical considerations,” Annu Rev Med, vol. 24, 1974. |
| [13] | Carré F, Guide pratique de la cardiologie du sport, Paris: Expression santé, 2010. |
| [14] | Netea RT, Lenders JW, Smits P, Thien T, “Both body and arm position significantly influence blood pressure measurement,” J Hum Hypertens, vol. 17, no. 7, pp. 459-62, July 2003. |
| [15] | Pickering TG, Hall JE, Appel LJ, Falkner BE, Graves J, Hill MN, Jones DW, Kurtz T, Sheps SG, Roccella EJ., “Recommendations for blood pressure measurement in humans and experimental animals: part 1: blood pressure measurement in humans: a statement for professionals from the Subcommittee of Professional and Public Education of the American Heart Association Cou,” Circulation, vol. 111, no. 5, pp. 697-716, 2005. |
| [16] | Corneloup L, "L’électrocardiogramme de l’athlète: particularités et limites,", OMD, 2006. |
| [17] | Ducardonnet A, Coeur et Sport. In: Traité Akos. Manuel du généraliste-cardiologie, Paris: Tsunami, 2012. |
| [18] | Carré F, "Le coeur de l'athlète,", Urgences, vol. 38, 2013. |
| [19] | D'Andrea A, Bossone E, Radmilovic J, Casso P; Calabro R, Russo M, Galderisi M, “The role of new echocardiographic techniques in athlete’s heart,” Eur Heart J, vol. 289, no. 4, 2015. |
| [20] | Baylos I, Bergeles N, Apostolidis N, Noutsos K and Koskolou M, Anthropometric, Body Compositionand Somatotype Differences of Greek Elite Female Basketball, Volleyballand handball Players, Dafni, Greecz, 2004. |
| [21] | Maaike G, Uberoi A, Vy-Vav S, Oort E, Myers J and Froelicher V, “The effect of sport on computerized electrocardiogram measurements in college athletes,” European Journal of preventive cardiology, vol. 19, no. 1, pp. 126-138, 2011. |
| [22] | Mitchell J, Haskell W, Snell P, Van Camp S, “Task Force 8: classification of sport. In: Maron B, Zipes D, eds. Bethesda Conference eligibility recommendations for competitative athletes with cardiovascular abnormalities,” J Am Coll Cardiol, vol. 45, 2005. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML