-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Internal Medicine
p-ISSN: 2326-1064 e-ISSN: 2326-1072
2018; 7(1): 1-3
doi:10.5923/j.ijim.20180701.01

Obstructive Left Atrial Myxoma with Severe Pulmonary Hypertension and Co-Existing Cor Triatriatum: A Case Report
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLJesuorobo DE, Kiridi EK
Cardiology Unit, Department of Internal Medicine, Federal Medical Centre, Yenagoa, Nigeria
Correspondence to: Jesuorobo DE, Cardiology Unit, Department of Internal Medicine, Federal Medical Centre, Yenagoa, Nigeria.
| Email: |  |
Copyright © 2018 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Cardiac myxoma is a benign neoplasm that is the most common primary cardiac tumor. We present a 28 year old woman who presented with features of congestive heart failure and was found during transthoracic echocardiography to have a huge left atrial myxoma obstructing the mitral valve orifice with associated severe pulmonary hypertension and cor triatriatum. She was subsequently referred for surgery with good outcome. Transthoracic echocardiography is an important tool in the evaluation of patients presenting with features of heart failure and cardiac myxoma should be included in the differential diagnosis of mitral valve stenosis.
Keywords: Cardiac myxoma, Heart failure, Mitral stenosis
Cite this paper: Jesuorobo DE, Kiridi EK, Obstructive Left Atrial Myxoma with Severe Pulmonary Hypertension and Co-Existing Cor Triatriatum: A Case Report, International Journal of Internal Medicine, Vol. 7 No. 1, 2018, pp. 1-3. doi: 10.5923/j.ijim.20180701.01.
1. Introduction
- Myxoma is the most common primary tumor of the heart and can arise in any of the cardiac chambers, although the left atrium is the most commonly involved. (75%) [1, 2] In rare occasions, myxoma is found in more than one chamber. It is more common in women and can be manifested at any age. [3] At the time of diagnosis, 92% of patients have symptoms of congestive heart failure. [4] Atrial myxomas may mimick valvular heart disease, cardiac insufficiency, cardiomegaly, bacterial endocarditis, disturbances of ventricular and supraventricular rhythm, syncope and systemic or pulmonary embolism. [1] We report a case of a huge obstructive atrial myxoma mimicking mitral valve stenosis with severe pulmonary hypertension and co-existing cor tria-triatum.
2. Case Report
- A 28 year old woman presented at the cardiology clinic with complaints of recurrent dyspnea and leg swelling of six month duration with a history of recurrent admissions for congestive heart failure. She had no prior history of hypertension, diabetes or coronary heart disease. Physical examination revealed prominent jugular venous pulsations, rales at the lung bases and hepatomegaly. A loud mid-diastolic murmur was noted at the apex during cardiac auscultation. Chest radiograph showed cardiomegaly, perihilar infiltrates and right sided pleural effusion.The electrocardiogram showed normal sinus rhythm. The trans-thoracic echocardiography showed a huge mobile mass in the left atrium attached to the inferior edge of the interatrial septum (Figure 1). The mass was noted to prolapse through the mitral valve during diastole (Figure 2). The left ventricular function was preserved however the right atrium and ventricle were dilated with severe tricuspid regurgitation. The pulmonary artery systolic pressure was estimated to be 95.1 mmHg. A membrane separating the right atrium into two chambers (cor tria-triatum) was also noted (Figure 2). She was commenced on anti-failure medications such as diuretics, lisinopril, spironolactone and the anticoagulant enoxaparin. She improved clinically and was subsequently referred for cardiac surgery at a cardiothoracic surgery center in a different city. Unfortunately she was lost to follow up afterwards and the outcome of surgery is not known.
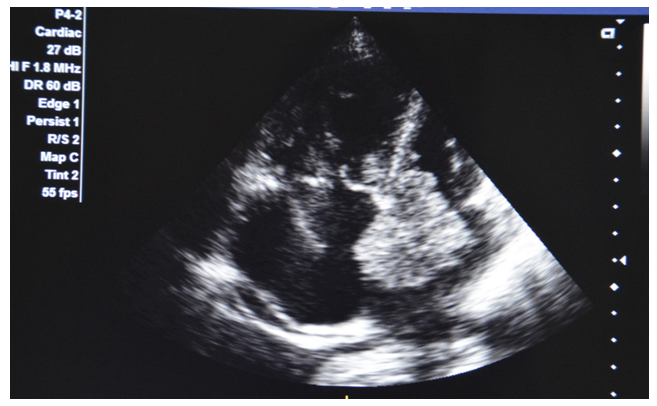 | Figure 1. Transthoracic echocardiography (Apical 4- chamber view) showing a huge left atrial mass attached to the atrial septum |
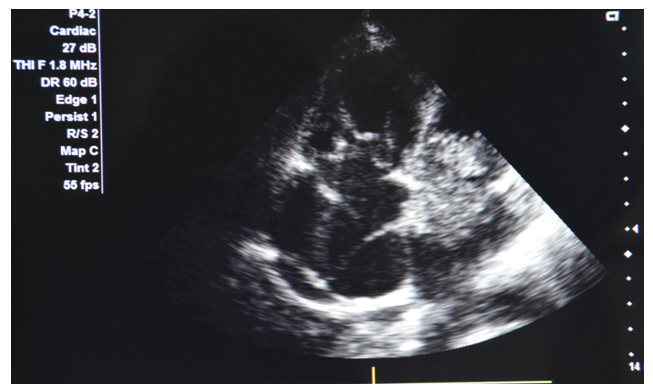 | Figure 2. Apical 4 chamber view showing the left atrial mass prolapsing through the mitral valve during diastole. Also note the dilated right atrium and ventricle and a membrane dividing the right atrium (cor triatriatum) |
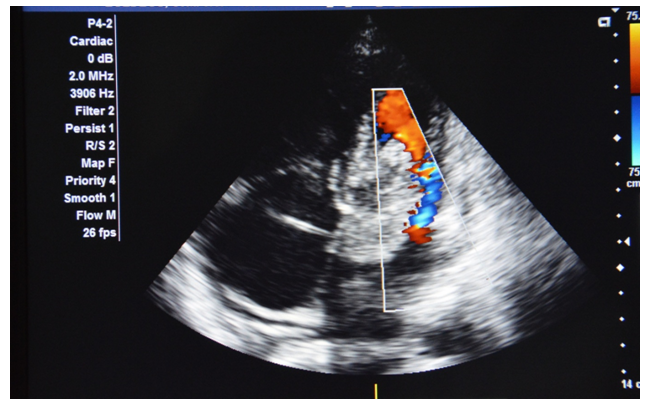 | Figure 3. Turbulent blood flow as the left atrial mass protrudes through the mitral valve mimicking mitral stenosis |
3. Discussion
- Myxoma is the most common primary cardiac tumor, and account for 83% of primary tumors. [5] The age of presentation varies from one month to 81 years with predilection for female gender (65%). [6] The majority of cardiac tumors are sporadic however, a mutation of chromosome 17 (17q24) in protein kinase A type 1-A can lead to Carney complex, a familial cardiac myxoma. [7] The clinical findings of cardiac tumors are characterized by the triad of embolism, intra-cardiac obstruction and constitutional findings. Congestive heart failure is the most common clinical presentation followed by neurologic and systemic embolic events. Embolic events more frequently affect the cerebral arteries and retinal arteries but embolization into visceral, renal or coronary arteries has been reported and can affect nearly 29% of patients. [1] Common constitutional symptoms are fever, malaise, weight loss, fatigue, anemia, and elevated erythrocyte sedimentation rate (ESR). [8]Mitral valve obstruction caused by atrial myxoma represents an important hemodynamic consequence leading to symptoms of congestive heart failure, pulmonary hypertension, syncope and sudden death. Clinico-pathologic correlations showed that mitral stenotic effects occurred when the tumor diameter exceeded 5 cm [8] as was the case in our patient. Up to more than a half of left atrial myxomas showed obstructive symptoms but only in 10% of patients will it cause severe mitral stenosis. [9] In our patient the huge myxoma occupied almost the entire left atrium and prolapsed into the mitral valve annulus during diastole causing functional mitral valve stenosis and severe pulmonary hypertension. Our patient also had an incidental finding of cor tria-triatum in her right atrium which has not been reported to co-exist with left atrial myxoma in the literature.Surgical removal is the treatment of choice for myxomas with the site of attachment resected with clear margin. This may be followed by artificial creation of an atrial septal defect that needs to be closed with a pericardial patch. The recurrence of myxomas has been reported to be less than 2% hence follow-up is necessary with a combination of clinical examination and echocardiography. [10]
4. Conclusions
- The importance of early echocardiography in a patient suspected of having heart failure cannot be over-emphasized. Cardiac myxomas are easily misdiagnosed and should be considered in the differential diagnosis in patients with suspected mitral valve disease.