-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Internal Medicine
p-ISSN: 2326-1064 e-ISSN: 2326-1072
2017; 6(3): 43-48
doi:10.5923/j.ijim.20170603.01

Association of Marital Status with Cardiovascular Risks in Urban Dwellers in Nigeria
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLErnest Ndukaife Anyabolu1, 2, Innocent Chukwuemeka Okoye1
1Department of Medicine, Chukwuemeka Odumegwu Ojukwu University, Awka, Nigeria
2Department of Medicine, Imo State University, Orlu, Nigeria
Correspondence to: Ernest Ndukaife Anyabolu, Department of Medicine, Chukwuemeka Odumegwu Ojukwu University, Awka, Nigeria.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

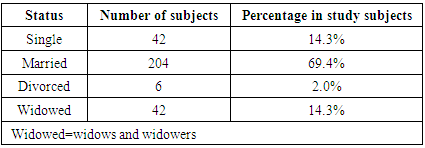
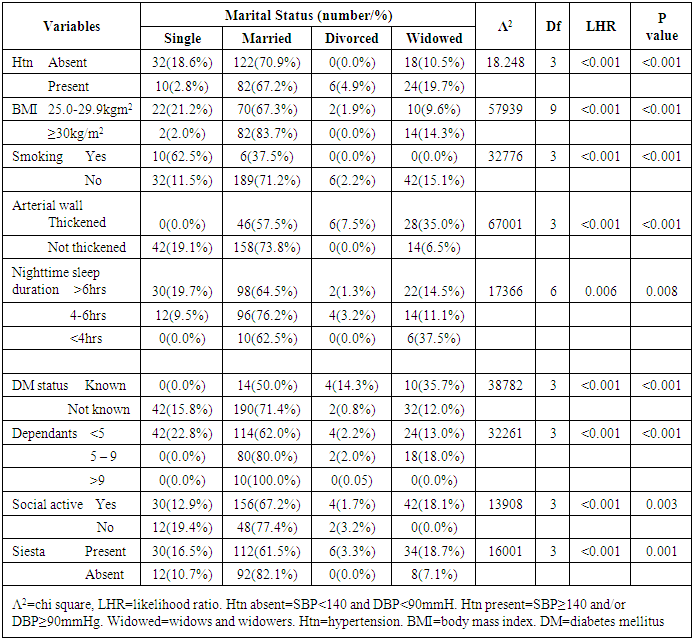
Background and Objectives: Marital status usually changes as life progresses. The seemingly increasing incidence of divorce and single status in the developing countries following the advent of westernization has not been completely characterized. The relationship arising from the status of marriage may impact positively or negatively on lifestyle and prevailing circumstance and subsequently influence the health of the subject. This study sought to assess marital status and determine the cardiovascular factors associated with married, single, divorced and widow status in people living in an urban city in Nigeria. Methodology: This was an unstructured cross-sectional study of urban dwellers. Anthropometric, clinical and other relevant data were obtained. Data were compared between different levels of marital status. Results: Females constituted 72.9% and males 27.1% of the subjects. Majority (98.6%) of the subjects were Igbo. Divorce was prevalent in 2.0% (males 2, females 4), widow status in 14.3% (M4, F38) and married status in 69.4% (M52, F152) of the subjects. Divorce was significantly absent among those aged <50 years and those ≥70 years. There was significant association between married status and Hypertension (67.2%), overweight (67.3%), obesity (83.7%), diabetes mellitus (50.0%), thickened atrial wall (57.7%), social activity (67.2%), seasta (61.5%), as well as short duration of nighttime sleep (<4hr) (62.5%), df=3, p<0.001. Majority (62.5%) of the smokers were single, df=3, p<0.001. Single and divorced subjects have the least number of children/dependants, (df=6, p<0.001). Conclusion: The prevalence of divorce was low and widow status high in this study. Cardiovascular risks - hypertension, overweight, obesity, diabetes mellitus, short nighttime sleep duration - were common among married subjects, and smoking among single subjects, in urban dwellers.
Keywords: Marital status, Single, Married, Divorced, Widowed, Cardiovascular risks, Short nighttime sleep, Seasta, Social activity, Urban dwellers, Nigeria
Cite this paper: Ernest Ndukaife Anyabolu, Innocent Chukwuemeka Okoye, Association of Marital Status with Cardiovascular Risks in Urban Dwellers in Nigeria, International Journal of Internal Medicine, Vol. 6 No. 3, 2017, pp. 43-48. doi: 10.5923/j.ijim.20170603.01.
Article Outline
1. Introduction
- For an individual, marital status is expected to change, from single status to married, and for some, to divorced status, yet for others, widowed status, as life progresses. There is seemingly an increasing incidence of divorce and single status in the developing countries, including Nigeria, following westernization [1, 2]. Studies have shown that the relationship encountered in any given marital status may impact positively or negatively on lifestyle and influence the health of the subject [3]. Married people have been shown to fair well following stroke events and chronic heart failure compared to single, divorced or widowed subjects [4, 5]. Some studies have also revealed that marital status confers some measure of protection and satisfaction that contribute to increased quality of life and good health [6, 7]. On the contrary, living alone in a non-marriage state, whether as a single, separated, divorced or widowed person, reduces quality of life and is associated with cardiovascular morbidity and mortality [6-8].Cardiovascular risk factors have been reported in the setting of stress, lack of social support, altered patterns of feeding, poor socioeconomic factors and poor night sleep duration at differing levels of marital status [4, 5, 9-14].There is a paucity of studies on the effects of marital status on health from Nigeria. This has prompted this study which sought to evaluate marital status and the association of some cardiovascular risks with the different levels of marital status in an urban city in Nigeria, with a view to creating awareness among these groups of people and to whittle down adverse outcomes.
2. Materials and Methods
- This study was cross-sectional and unstructured. It involved 294 subjects in Awka, an urban city in Nigeria. The subjects consisted of hawkers, artisans, clerical staff, traders among others, drawn from Eke Market in Awka, Nigeria. The management of the market approved the study. With the support of the management of the market, through a gong crier, the subjects were informed of the study. Informed oral consent was obtained from each study participant. The thrust of the study was explained to them.Data were obtained with the aid of a questionnaire. Addressed in the questionnaire were biodata, diabetes mellitus status, cigarette smoking, tobacco snuff use, alcohol use, marital status, night-time sleep duration, economic status, annual leave duration, number of dependants, social activities, siesta.Anthropometric and demographic data were obtained. Weight (kg) and height (m) were taken and BMI was determined as weight/height2 (kg/m2). Radial and brachial arteries were examined for thickening, and pulse rate was obtained. Blood pressure (mmHg) was recorded from the non-dominant hand in a sitting position, after the subjects had rested for 10 minutes, using appropriate cuff size to cover about 80% of the arm, using Accoson mercury sphygmomanometer. Three blood pressure readings were taken 5 minutes apart, and the average obtained. [15, 16] The variables were graded into groups as follows:Marital status: 1) single, 2) married, 3) divorced, 4) widowedSmoking: 1) those who were smokers and 2) those who were non-smokersTobacco snuff use: 1) those who used tobacco snuff and 2) those who did notAlcohol: 1) those who have positive alcohol history and 2) those who have notArterial wall: 1) those who have thickened arterial wall and 2) those with normal arterial wallNight-time sleep duration: A) >6 hours, B) 4 – 6 hours, C) <4 hoursDiabetes mellitus: 1) those known to be diabetic prior to the screening and 2) those whose diabetic status was not known prior to the study.Number of children/dependants: A) <5, B) 5 – 9, C) >9Annual leave duration: A) >4 weeks, B) 2 – 4 weeks, C) <2 weeks, D) noneEngaged in Social activity: 1) yes and 2) noneSiesta: 1) some siesta and 2) noneThe influence of the variables on marital status were compared between the groups for each variable. The potential factors of marital status evaluated were diabetes mellitus, cigarette smoking, tobacco snuff use, alcohol use, annual leave, night-time sleep duration, number of dependents, social activities, siesta, thickened arterial wall. [16]Data AnalysesThe data were analyzed using the Statistical Package for Social Sciences (SSPS Inc, Chicago, IL) version 17.0 statistical software. For continuous variables, mean values and standard deviations were calculated and the means compared using ANOVA or two sample t-test. Categorical variables were compared using the nonparametric tests Chi-square. The distribution and characterization of variables with BMI were analyzed using cross tabulation. Correlation statistics were used to determine the association between BMI and variables, while multivariate linear regression was used to determine the strength of the variables to predict BMI, underweight and obesity. All tests were two-tailed with P < 0.05 taken as statistically significant. Definition of terms:Hypertension: SBP ≥140mmHg and or DBP ≥90mmHg [17];Mild hypertension: SBP 140–159 mmHg and/or DBP 90–99 mmHg;Moderate hypertension: SBP 160–179 mmHg and/or DBP 100–109 mmHg;Severe hypertension: SBP ≥ 180 mmHg and/or DBP ≥ 110 mmHg.Body mass index: [16, 18]Underweight: BMI <18,5kg/m2Normal body weight: BMI 18.5 – 24.9kg/m2Overweight: BMI 25.0 – 29.9kg/m2Mild obesity: BMI 30.0 – 34.9kg/m2Moderate obesity: BMI 35.0 – 39.0kg/m2Severe obesity: BMI ≥40.0kg/m2Obesity: BMI ≥30.0kg/m2. In this study Obesity was defined as BMI ≥30.0kg/m2Counselling was given to those subjects who were found to have cardiovascular risks. They were advised to see clinicians in the hospitals.
3. Results
- This study evaluated the association of cardiovascular risks with the different levels of marital status in 294 subjects in an urban city in Nigeria. Females made up 72.9% and males 27.1%. Their mean age was 43.1±15.4years and range 70years. Majority (98.6%) of the subjects were Igbo. The mean values of the variables were: BMI 28.1±6.0kg/m2, SBP 129.3±23.7mmHg and DBP 82.6±14.7mmHg (Table 1).
|
|
4. Discussion
- This study showed a prevalence of 2.0% for divorce among urban dwellers in Nigeria. This value is low compared to the values reported in 2 studies in US (10.0%) and Europe [15, 16]. Sociocultural differences might be advanced as explanation for these observed differences. However, this is similar to the divorce prevalence reported in Asia [17] a population that has a related sociocultural background as Nigeria. The widow status prevalence of 14.3% observed in this study is high compared to the value documented in another study [18]. Low life expectancy in Nigeria might contribute in this high prevalence of widow status [19, 20]. However, more females (90.5%) than males (9.5%) as was observed in this study have widow status reflecting the global trend that women live longer than men [29, 30].Divorce was significantly absent among those aged <50 years and those aged ≥70 years in this study. The observed absence of divorce among those aged <50 years contrasts with a high rate reported in other studies in Lagos, Nigeria [31, 32]. Religious concerns and the present wave of Pentecostalism in this domain profoundly protect and sustain many marriages, and might proffer an explanation [33]. With increasing age, the propensity to divorce would decline as the very fabrics, the psychosocial support, and economic security which drive marital unions might not have attractive, dependable alternatives, should divorce be contemplated. This perhaps night explain the absence of divorce among those aged ≥70 years observed in this study, similar to that reported in other studies [34, 35]. In this study it was demonstrated that hypertension (67.2%), overweight (67.3%), obesity (83.7%), diabetes mellitus (50.0%), thickened atrial wall (57.7%), social activity (67.2%), seasta (61.5%), and short duration of nighttime sleep (<4hr) (62.5%), observed in married subjects were significantly high. Studies have reported low incidence of hypertension, stroke mortality and other cardiovascular risks among married people compared to unmarried subjects, contrasting with the observation in our study [40-43]. It was shown that marital relationship in which couples feel a good measure of satisfaction and protection confers minimal stress, and amplifies the security that would reduce cardiovascular risks, when compared with those observed in unmarried, separated, divorced or widowed people. [6, 7]. Short nighttime sleep duration, a cardiovascular risk, observed in married people in this study, might stem from the engagement in nighttime duties as seen in those involved in essential duties and in independent business persons who wake early every day to prepare for their business [16]. Access to health facilities and care provided by partners also contribute in low morbidity and mortality among married subjects [6-8]. However, the opposite was observed in married subjects in this study; which showed an association between married status and hypertension, overweight, obesity, DM, thickened arterial wall, as well as short nighttime sleep duration. One Nigerian study has reported an association between marital status and hypertension and another between marital status and overweight/obesity [16, 44]. It was inferred that marriage provides a soothing relationship that bolsters food security and encourages regular nutrition, sometimes leading to over nutrition with resultant tendency to the development of overweight and obesity and subsequently dyslipidemia, all cardiovascular risks. This, perhaps, could explain in part the observations in our study subjects. Married subjects are more likely to eat at home, compared to single and divorced subjects who eat outside the home, in bookers and restaurants, an observation reported in one study within the same domain as this study [44]. Added to this might be the universal rising incidence of obesity and overweight with increasing socioeconomic status in developing countries including Nigeria, accounting for the observed difference in the association of cardiovascular risk factors with marital status, compared to those in the developed nations.Family support, religious influence and the presence of a new marriage tend to dissuade obnoxious and unhealthy habits among couples [45]. This could explain in part the observation in this study that found majority (62.5%) of the smokers were single. Family size, anchored by the number of children and dependants, is a source of succor as well as of worries. Single and divorced subjects, who have a very small number of dependants, perhaps, might have minimal worries to contend with, compared to married subjects, as was observed in this study. Such stress related to a high number of children/dependants might explain the association of cardiovascular risks with the status of marriage observed in this study [46].Discordance in marriage might lead to stress, abnormal eating and drinking behavior and negatively impact on the health of married subjects [46]. This might explain the association of cardiovascular risks with marital status documented in this study. However, the influence of marital discordance or disaffection was not evaluated in this study. Overall, this study has demonstrated that hypertension, DM, overweight and obesity, thickened arterial wall, short nighttime sleep duration, large family size/dependants, and social activity were cardiovascular risks associated with marital status, whereas smoking was associated with single status among urban dwellers in Nigeria.
5. Conclusions
- The prevalence of divorce was low and widow high in this study. Cardiovascular risks - hypertension, abnormal weight, DM, short nighttime sleep duration - were common among married subjects, and smoking among single subjects in this urban city. There is a need for clinicians, epidemiologists and other stakeholders to search for cardiovascular risks among married subjects in routine practice to forestall adverse outcomes.
Limitations of the Study
- The influence of marital relationship satisfaction and marital relationship disaffection on the health of partners were not evaluated in this study. This would have helped in further identifying cardiovascular risks among these subgroups of married people. The study population was small. A larger study size would have been more representative of the population.