-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Internal Medicine
p-ISSN: 2326-1064 e-ISSN: 2326-1072
2017; 6(2): 36-41
doi:10.5923/j.ijim.20170602.03

Prevalence of Depression among Tenth Graders one Month Prior to Board Exam (SSS)
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAnurag Raje1, Madhav Gajananrao Raje2
1Dept. of Medicine, Institute of Medical Sciences & Research, Mayani, Satara, India
2Dept. of Psychiatry & Psychotherapy, Mahakali Hospital & Polyclinic, Nagpur, India
Correspondence to: Madhav Gajananrao Raje, Dept. of Psychiatry & Psychotherapy, Mahakali Hospital & Polyclinic, Nagpur, India.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

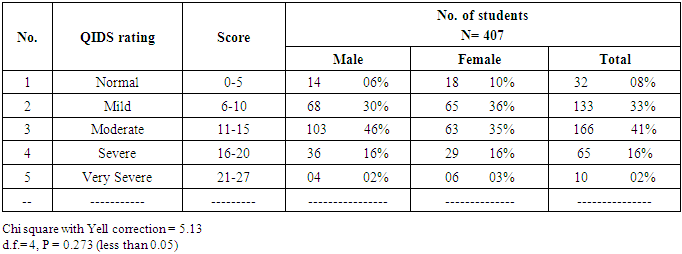
To know prevalence of depression among tenth graders one month prior to board exam & to assess their symptomatology of depression a cross-sectional study among the tenth graders in rural area, using the Quick inventory of depressive symptomatology (QIDS) a self assessment report was undertaken. Research question underlying was whether exam causes depression. Study was conducted in three schools under the vigilance of respective class teachers. Total 407 students took the QIDS self report questionnaire along with personal information questionnaire. 92% students were found depressed. Out of 407 students, 166 students (41%) were suffering from moderate depression, 65 students (16%) were suffering from severe and 10 students (2%) were suffering from very severe depression. 32/407 (8%) students did not fulfill the criteria of depression. Gender prevalence ratio i.e. male to female students were almost equal. Prevalence of somatic symptoms was higher though guilt was the most common symptom noticed. Possibility of board examination being attributer may be considered, however further detail study is need of hour to confirm role of board examination.
Keywords: Adolescent, Depression, Board exam going students, Excessive guilt, Common symptoms of depression, Role of exam
Cite this paper: Anurag Raje, Madhav Gajananrao Raje, Prevalence of Depression among Tenth Graders one Month Prior to Board Exam (SSS), International Journal of Internal Medicine, Vol. 6 No. 2, 2017, pp. 36-41. doi: 10.5923/j.ijim.20170602.03.
Article Outline
1. Introduction
- Depression (major depressive disorder or clinical depression) is a common but serious mood disorder. It causes various symptoms that affect how you feel, think, and handle daily activities, such as sleeping, eating, or working [1]. To be diagnosed with depression, the symptoms must be present for at least two weeks. It has become a common and alarmingly increasing disorder among adolescents [1]; affecting their socialization, family relations, and school performance; with long term consequences. Some long term consequences include risk of alcohol abuse, antisocial behaviors, & hospitalizations.Biggest concern among adolescents is rising rate of suicides, the third leading cause of death among older adolescents (Centre for Diseases Control, WISQARS) [2]. WHO has stated that incidence of depression is rapidly rising and threat looms that depression will be the most common disease, surpassing Diabetes Mellitus and Cancer. WHO stated that by 2020 depression could be 2nd most prevalent disease [3].Previous studies with similar premise have proven an increase in the prevalence of depression among school students. A study done in NIMHANS Bangalore, found 18.4% adolescents depressed. Malaysian Study revealed 10.3% of secondary school students suffering from depression. Karim Munir, Psychiatrist from Harvard Medical School & Ibrahim Yildirim, PhD, Turkey University, found 45.1% of the students with depressive symptoms, while preparing for national University entrance examination. A Saudi Arabian study revealed prevalence of depression among school students was 22.4% as moderate, 7.3% as severe and 3.7% as very severe, with self criticism, agitation, and loss of energy as the commonest symptoms. Prevalence of depression among adolescents was 50.3% in one Malaysian study published in 2015 [1]. Trinidad study revealed, one fourth of the secondary school students were significantly depressed which was strongly associated to age, gender, school type & family structure [4]. All of these studies found clear predominance of depression among girls. Other variables according to the 1986 study of Minnesota high school students revealed that trouble with brother or sister (Sibling role) was one of the most common risk factor for developing depression among adolescents and according to Kaslow et al, family variables associated with depression are parental psychopathology, divorce, low socio-economic-status (SES), negative life circumstances including loss of family member, domestic abuse, or neglect, and low levels of social support.Nowadays, depression and suicidal tendencies among students have been found correlated [1, 5] & increased especially before and after board exams. Does that mean board exams have a role to attribute depression among students? To find answer of this question if not directly but indirectly, we decided to examine students of tenth grade one month before the board exams. We decided to focus on symptomatology & level/intensity of depression just before exam.
2. Material and Method
- We approached students of tenth grade from three different schools on consecutive days, one month prior to their final board exams in 2015. They were all apparently healthy students, with no known illnesses.Instrument- depression was assessed by QIDS scale and a personal information questionnaire. QIDS is a linkert type of self report scale with fourteen questions. A Marathi (local language) translated version was used. Personal information questionnaire consisted of 9 questions regarding age, sex, qualification of parents, number of siblings, total number of family members, total income of family, exam phobia, getting ‘blank’ during exam, excessive parental worry about SSC/board exam.Method- We obtained school’s permission and written consent from students. We collected data from 407 students (of which boys were 226 and girls were 181) of 3 schools participated on consecutive days, 1 month prior to SSC exam.All the students were briefed about the test & research project. Test was simultaneously administered in class-room settings under the strict vigilance of teachers & investigators. Discipline and care was taken to constraint students from imitating/copying or interacting with each other while writing self report questionnaire. There was no time constraint while answering questionnaire. Observations made were tabulated, prevalence was inferred, major symptoms were evaluated percentage wise & other variables were noted.
3. Results
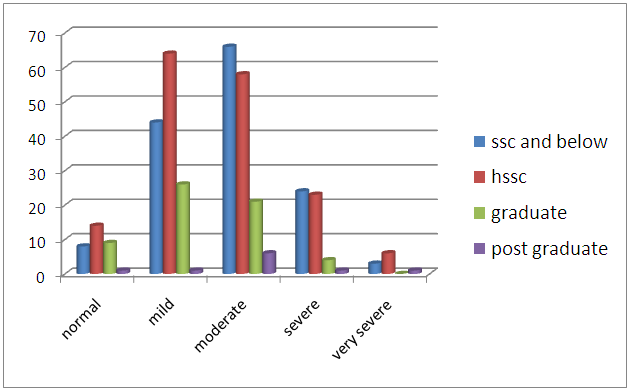
- 92% students of our study population were depressed. Out of them 55.53% were male & 44.47% were female students. 90.05% female students among themselves (out of 181 female students) showed depressive tendencies, whereas in case of male it was 93.80% (out of 226 male students). Prevalence of depression among both sexes was similar. Out of the 407 students, 10 students (2%) revealed very severe depression, 65 (16%) had severe depression, and 166 (41%) had moderate depression. 18 female and 14 male students (total approx. 8%) were not suffering from depressive features out of total study group of 407. Other factors attributing depression were lower literacy of parents, worrisome parents (79%) & their children (90%). More than 50% students were suffering from exam-phobia like symptom.We did not find significant association between grades of depression & sex of students. This means levels of depression are similar among both sex.
4. Discussion
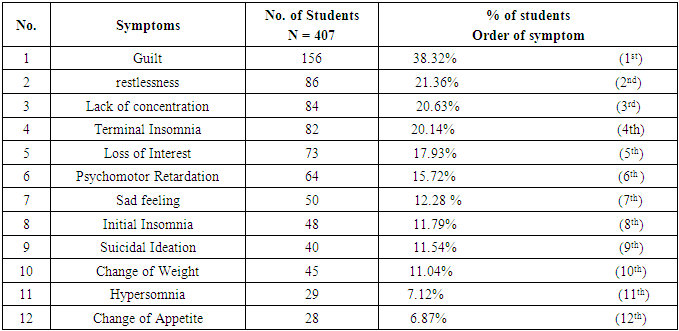
- Our findings should be interpreted in the light of study’s limitations, first being a study of exam-going students i.e. students under the sheer pressure of first qualifying/life turning exam may over-react to the questions. No such other study is done as per our search hence value of observations even with limitations cannot be under-rated or disregarded, we thought. Second limitation was assessment of depression was done in class rooms based on one-timed applied self-report questionnaire. Though use of self-report questionnaire is well accepted & considered valid for such assessment studies, however limitations are also accepted in view of generalization. Third limitation is statistical value. Instead of vigorous statistical evaluation our results are derived through percentage based analysis. Significance of this study rests on observations, it’s percentage-wise strength and the direction one gets for further future study to explore research question. Our focus in this study was to find out presence of depression & its symptomatology. One review mentions that depressive symptoms & depressive disorder in adolescents are much similar and can be considered equal while diagnosing it [6]. This review published in Lancet 2012 corroborates our decision to consider diagnosis of depression in adolescents very close to symptomatology. Hence our focus was both depression & symptoms. Many researchers had mentioned too many common symptoms of depression which causes difficulty in fixing only a few; e.g. only 3/5 common symptoms are not mentioned by researchers while discussing symptomatology of adolescent depression. Some studies had mentioned common symptoms like irritability, conduct disorder, substance abuse, mood reactivity, somatic complaints, and change in appetite/behavior. While another study observed self-criticism, agitation, & loss of energy most common symptoms [7]. Weiner (1980) reported that the triad of common symptoms is fatigue, hypochondria & difficulty in concentration [7]. However, these studies were not focusing on symptomatology especially. So we decided to focus our search to find out only 5 commonest symptoms if possible & observe the order if any. Table 2 depicts it.
|
|
|
5. Conclusions
- 92% students of our study population were depressed just before board’s exam. This observation demands further study. Commonest symptom was guilt (38.32%). Possibility of exam attributing depression in adolescents merits further detail study.
ACKNOWLEDGMENTS
- We are thankful to Dr. Ashok Jadhav, Professor, HOD of Dept of Community Medicine, IGGMC, Nagpur & to Dr. Sanjay Agrawal, Associate Professor of Community Medicine, IGGMC, Nagpur, India for their assistance in application of statistical work.