-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Internal Medicine
p-ISSN: 2326-1064 e-ISSN: 2326-1072
2017; 6(2): 33-35
doi:10.5923/j.ijim.20170602.02

Clinical Study on Ischaemic Strokes after Disulfiram-Ethnol Reaction
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAlagesan S., Gratia T., Paulraj, Ahamed, Arumuga Pandian
Department of Medicine, Tirunelveli Medical College, Tirunelveli, Tamil Nadu, India
Correspondence to: Alagesan S., Department of Medicine, Tirunelveli Medical College, Tirunelveli, Tamil Nadu, India.
| Email: |  |
Copyright © 2017 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Disulfiram has been used in the treatment of alcohol addiction for more than 50 years. It causes aversive behaviour due to Disulfiram-Ethanol reaction which is characterised by vomiting, flush, sweating, tachycardia, hypotension and restlessness. Usually, it will not produce serious complication. Very rarely serious complications like stroke, myocardial infarction and severe hypotention can occur. In Disulfiram Ethanol reaction we present two cases of Ischemic strokes which occur during alcohol-ethanol reaction.
Keywords: Disulfiram, Disulfiram ethanol reaction, Ischaemic cerebral infarction
Cite this paper: Alagesan S., Gratia T., Paulraj, Ahamed, Arumuga Pandian, Clinical Study on Ischaemic Strokes after Disulfiram-Ethnol Reaction, International Journal of Internal Medicine, Vol. 6 No. 2, 2017, pp. 33-35. doi: 10.5923/j.ijim.20170602.02.
1. Introduction
- Disulfiram was first used in 1940 in the treatment of alcohol dependency. It produces aversive behaviour due to Disulfiram-Ethanol interaction. Clinical features of this unpleasant reaction occurs after ethanol intake characterized by tachycardia, sweating, flush, vomiting, hypotension [1] and restlessness [2, 5] Very rarely it can cause life threatening hypotension, stroke [3, 4] myocardial infarction [2, 5, 6] and death [1].
2. Case 1
- 32-years old man Mr. A with chronic alcoholism, initiated treatment with disulfiram 250mg/daily for 10 days prescribed by a psychiatrist. On day 10, he consumed 200 ml of brandy. About 30 minutes later he developed severe sweating, tachycardia, vomiting tremors, restlessness, and confusion. He was admitted in our hospital.On admission, he was confused, drowsy, afebrile. His blood pressure was 130/80mm/hg, pulse 90/mt. regular. Neurological examination revealed left hemiplegia. There was no signs of meningeal irritation. Cardiac vascular, respiratory and abdominal examination were within normal limits. On investigations complete haemogram, routine biochemical parameters like blood sugar, urea, creatinine, liver function test, lipid profile, serum calcium, magnesium, electrolytes, ABG were within normal limits.ECG, ECHO, were normal.CT scan Brain, and MRI diffusion image shows acute infarct in Left middle cerebral infarct. Doppler study showed reduced flow in right MCA and ACA.
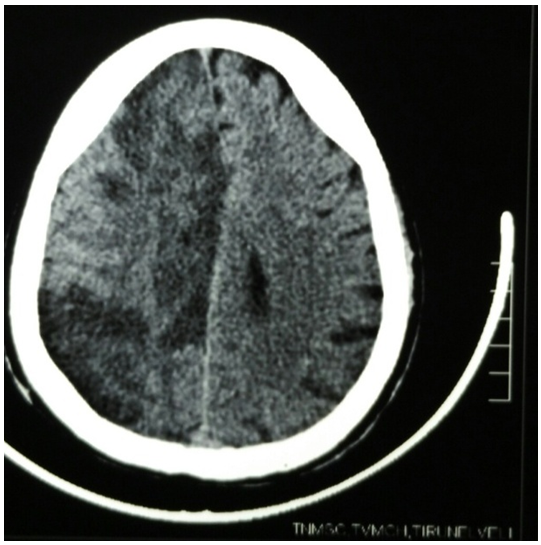 | Figure 1. Case - A, CT Scan Brain showing massive right MCA infract |
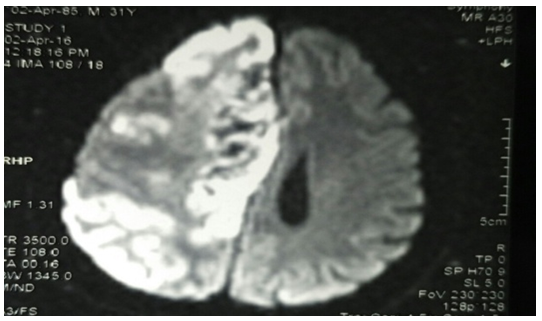 | Figure 2. Case A MRI Diffusion image showing massive right MCA infract |
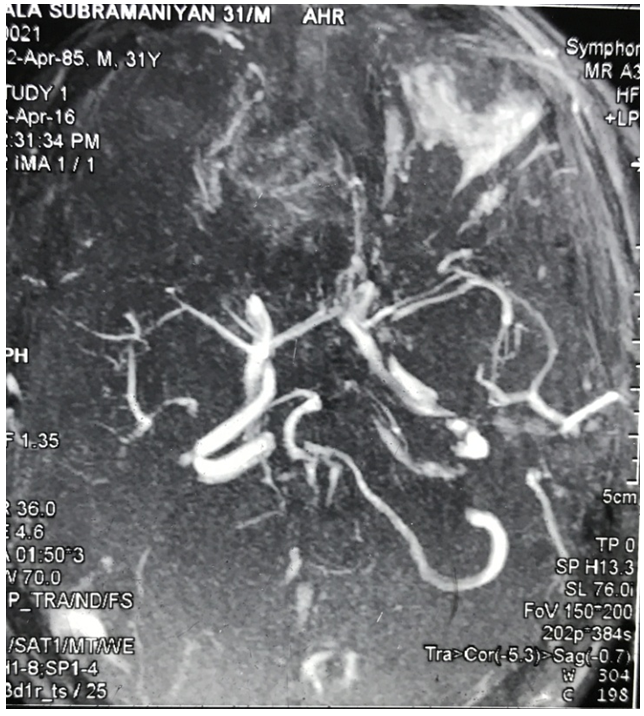 | Figure 3. Case B MRI Angio shows non visualisation of right MCA |
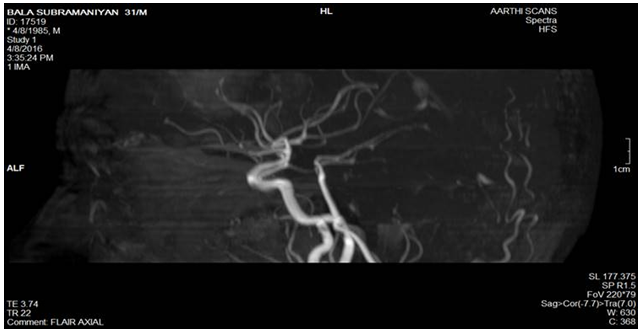 | Figure 4. Case B Repeat MR Angio showing regcanalisation right MCA |
3. Case 2
- 29 years old Mr.B chronic alcoholic admitted in psychiatry department for de-addiction treatment. Initiated with disulfiram 250 mg od for a week, and increased to 250 mg bd.Two weeks later he drank 100ml of whisky, 3 mints later he developed severe sweating, palpitation, tachycardia.On examination a patient was drowsy, afebrile, confused and right hemi paresis was present. Pupils were equal, with intact pupillary reflexes and there were no meningeal signs.On investigations, complete haemogram, blood sugar, renal function test, liver function test, lipid profile, ABG, electrolytes were within normal limits, his ECG, ECHO, was normal.CT scan brain shows moderate sized left parietal and frontal infract.HIV, VDRL, ANA profile, Homocystine Anti phospholipid antibody, lupus antibody and protein-s protein-c and antithrombin III were within normal limits.A final diagnosis of chronic alcoholism with Disulfiram Ethanol reaction with ischaemic stroke was made.
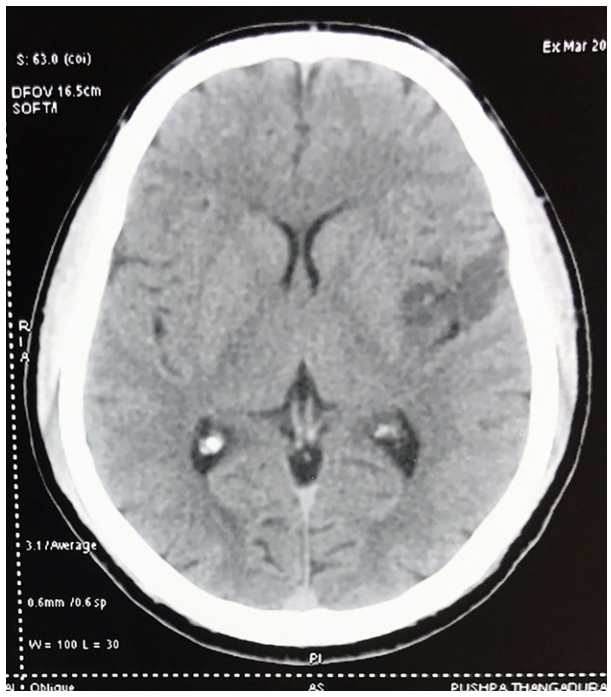 | Figure 5. Case 2 CT Scan brain showing left MCA infract |
4. Discussion
- Disulfiram has been used in alcohol dependency for more than 60 years. It acts by creating aversive behaviour in patients which deters them from alcohol abuse due to a phenomenon called Alcohol Disulfiram reaction. This unpleasant reaction is due to increased accumulation of serum acetaldehyde by the metabolism of ethanol since disulfiram is a powerful inhibitor of enzyme acetaldehyde dehydrogenase that degrades it.Disulfiram Ethanol reaction is clinically characterized by attacks of flushing, nausea, vomiting, excessive sweating, tachycardia and mild hypotension.In these two patients the DER was very severe. But there was no cardiovascular collapse, and blood pressure was maintained in both these patients.Patients who are taking disulfiram exposed to ethanol develop symptoms of DER within 15 minutes and are lasting up to 1 hour and then gradually subside over next few hours.Ischemic stroke following DER has been reported in just 2 cases [4, 5] in literature. Milne HJ et.al [2] and Ho.MP et.al have reported 2 cases of exceptionally severe reaction with hypotension and cardiovascular collapse. But in our cases ischaemic strokes have occurred without hypotension Maria. G Prancheva et. al [4] reported a case of right cerebral infarct in water shed zones in association with severe hypotension. M Suresh Babu et. al [5] reported first case of ischaemic stroke in hemodynamically stable patient in whom the details of the MR angiogram not available. In our first case was probably due to vasospasm of internal carotid artery as evidenced by the reduced flow both in MCA and ACA territory in carotid artery dopplar and MRA shows non visualisation of these arteries on initial MRA and visualization of this arteries in follow up MRI. The cerebral infarction can be attributed to the spasms of cerebral vessels which may be due to the release of catecholamines from the sympathetic terminals of the blood vessels and result in vasoconstriction. The incidence of AMI in patients with normal or near normal coronary arteries ranges from 1% to 12% [7] and mainly affects young people and is distinctly rare in patients older than 50 years [7]. The mechanism leading to AMI in these patients remain unknown. It has been postulated that the probable mechanism may be temporary occlusion of the infarct related vessel by spasm or thrombus or a combination of both.
5. Conclusions
- DER remains one of the best measure for creation of aversive behaviour in patients with alcohol dependency. Though complete recovery is the usual outcome in clinical settings life threatening complications like cardiovascular collapse myocardial infarction and ischemic cerebral infarct can occur. Despite the favourable outcome in our present case series it should be born in mind that disulfiarm is not a life saving approach to alcohol dependency and patients not complying to the strong restrictions in this therapy should not be eligible for that kind of alcohol dependency management.