Nasr A. Belacy1, 2, Abdullah H. Altemani3, Mostafa H. Abdelsalam1, 4, Magdi A. El-Damarawi1, 5, Basem M. Elsawy1, 6, Noha A. Nasif1, 7, Eman A. El-Bassuoni1, 8
1Department of Physiology, School of Medicine, University of Tabuk, Saudi Arabia
2Department of Physiology, School of Medicine, Benha University, Egypt
3Department of Family Medicine, School of Medicine, University of Tabuk, Saudi Arabia
4Department of Physiology, School of Medicine, Zagazig University, Egypt
5Department of Physiology, School of Medicine, Tanta University, Egypt
6Department of Physiology, School of Medicine, Beni Swaif University, Egypt
7Department of Physiology, School of Medicine, Ain Shams University, Egypt
8Department of Physiology, School of Medicine, El Minia University, Egypt
Correspondence to: Mostafa H. Abdelsalam, Department of Physiology, School of Medicine, University of Tabuk, Saudi Arabia.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
Abstract
Background/Aim: Lung function testing is an important measure to diagnose many respiratory disorders. However, their proper interpretation relies mainly on the availability of appropriate reference data. Many reference values are available but most of them are directed to western populations, leaving the rest of the world uncovered despite the established effects of different ethnicity on Lung function tests. Moreover, Very little data are available that can be used as reference values for Saudi people. Therefore, this study was designed to generate prediction equations for respiratory parameters that could be applied for Saudi adult persons. Methods: Three hundred healthy- never smoker adult Saudi students from Tabuk University (150 male and 150 female) with age range 18-25 years were assessed for respiratory functions by oral spirometry. Measured parameters included: Vital capacity (VC), forced vital capacity (FVC), forced expiratory volume first second (FEV1), FEV1/FVC%, forced expiratory flow in mid portion of FVC (FEF25-75%) and maximum voluntary ventilation (MVV). Multiple regression analysis; using sex, height and weight as predictors; was carried out to estimate prediction equations for the respiratory parameters measured. Our results were then compared with data obtained from other studies for Caucasian, African and Japanese ethnic groups. Results: The predicted values for Saudi adults were lower for both male and female subjects than Caucasian, African and Japanese subjects for most of the parameters tested. The greatest difference was obsereved between Saudi adults and Caucasians. However, FEV1/FVC% was higher in Saudi subjects than all other ethnic groups. Moreover, FEF25-75% was higher in male Saudi adults than the other ethnic groups. In addition, in adult Saudi females VC was higher than African and Japanese and lower than Caucasian ones. Conclusions: A considerable difference was found between prediction equations and reference values obtained in the present study and other ethnic groups as Caucasian, African and Japanese. Therefore, pulmonary function reference values and prediction equations were derived for both sexes between the ages 18-25 years in healthy non-smoker Saudi adults. This will provide accurate interpretation for lung functions in this population.
Keywords:
Spirometry, Lung function tests, Vital capacity, FEV1, FVC, FEF25-75%, MVV
Cite this paper: Nasr A. Belacy, Abdullah H. Altemani, Mostafa H. Abdelsalam, Magdi A. El-Damarawi, Basem M. Elsawy, Noha A. Nasif, Eman A. El-Bassuoni, Reference Values for Lung Function Tests in Adult Saudi Population, International Journal of Internal Medicine, Vol. 3 No. 3, 2014, pp. 43-52. doi: 10.5923/j.ijim.20140303.02.
1. Introduction
Pulmonary function tests fulfill a pivotal role in respiratory medicine [1]. Reliable interpretation of pulmonary function results relies on the availability of appropriate reference data [2]. Pulmonary function varies with age; standing height, sex and ethnicity [1]. American Thoracic Society (ATS) recommended the use of the ThirdNational Health and Nutrition Examination Survey (NHANES III, 1988-1994) as a reference for spirometric functions. This survey is nationally representative and generalizable as it included an oversampling of African-American and Mexican-American population [3]. In Europe, they use the European Community for Steel and Coal reference [4]. However, in other countries it is left for individual laboratories to select appropriate reference equations [2]. Recently, Quanjer et al. [1] developed prediction equations for spirometric indices, which are applicable globally to different ethnic groups, and was referred to as Global Lung Function 2012 Equations. However, this study did not give significant attention to the Arab World. Different studies from other countries like Brazil [5], Australia [6], Iran [7], India [8], and Pakistan [9] had published their data in an attempt to establish their own reference values. In addition, few studies from Arab countries presented reference equations for spirometric functions in Jordanians [10] and Omani adults [11]. In Saudi Arabia, very little data were available from few old studies [12-14]. The aim of this work was to do an updated assessment of pulmonary functions in Saudi adults, to set a local reference equation of the Saudi population and to compare our results with some other ethnic groups.
2. Material and Methods
2.1. Subjects
This study was carried out on 300 (150 male and 150 female) healthy, adult students aged 18-25 years. Participants (randomly chosen from the University of Tabuk in Saudi Arabia) were nonsmokers and were free from any acute or chronic conditions that could affect the validity of the tests. Subjects with a history of asthma, chronic bronchitis, chronic cough, exposure to any toxic chemicals, or surgery involving the chest wall were excluded. In addition, Subjects who were unable to perform spirometry according to ATS guidelines were excluded.Spirometry was postponed if the subjects had any flu-like illness or cold. The study was approved by the Research Committee of the University of Tabuk. All subjects gave their informed consent after explanation of all the test procedures. Data were obtained for each subject regarding age, sex, height, and weight. The height was measured with the subject standing barefoot, and weight in light clothes was recorded by an electronic balance.
2.2. Spirometry
A computerized Spirolab II® spirometer (Medical International Research MIR, Rome, Italy) with a mouthpiece connection was used for this study. This Spirolab is based on a turbine sensor that works on the infrared interruption principle. Spirolab makes breathing tests and calculates an index of test acceptability (test quality control) and a measure of reproducibility. It also gives functional interpretation with 11 possible levels following the latest ATS/ ERS (American Thoracic Society/ European Respiratory Society) classification [15-17]. Measured parameters of spirometry included: Vital capacity (VC), forced vital capacity (FVC), forced expiratory volume first second (FEV1), FEV1/FVC%, forced expiratory flow between 25% and 75% of forced vital capacity (FEF25-75%) and maximum voluntary ventilation (MVV).
2.3. Instructions to Subjects
All subjects received the same instructions. They were allowed to do multiple trials before the start of the experiment in order to be familiar with the test procedures. The ATS guidelines for spirometry were rigidly followed [17]. For performing spirometry, a conventional cardboard mouthpiece (supplied with the spirometer) without teeth grip was used, whereby the subject was required to hold the mouth piece and the nose was closed tightly with the nose clip. The subject was allowed to complete at least 3 trials and the highest one was considered the right one. At least 3 minutes for rest were allowed between any two trials.
2.4. Statistical Analysis
The results of VC, FVC, and FEV1, FEV1/FVC%, FEF25-75% and MVV were measured by spirometry. The data were expressed as mean ± SD and it were analyzed using IBM SPSS® for Windows (v. 21). Normal distribution of data was detected by Shapiro-Wilk Test. Then, all variables were compared using unpaired student t test. The results were considered significant if p value < 0.05. In order to generate prediction equations for spirometry in young Saudi people, correlations were made for different parameters measured against age, height, weight and sex as independent variables in all subjects. Multiple regression analysis were then performed (Only the significant correlations were included in the equations) to derive separate prediction equations for each spirometric measurement.
2.5. Comparisons of Reference Equations
The newly derived reference equations were compared with those used by European Respiratory Society (ERS) for other ethnic groups including Caucasian, Japanese and those with African descent.
3. Results
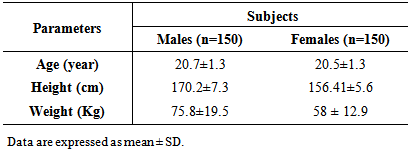
As shown in table (1): this study included 300 subjects (150 male and 150 female). The mean age was 20.7±1.3 and 20.5±1.3 year, the mean height was 170.2±7.3 cm and 156.4±5.6 cm and the mean weight was 75.8±19.5 and 58±12.9 Kg for males and females respectively.Table 1. Number, age, height and weight in male and female subjects
 |
| |
|
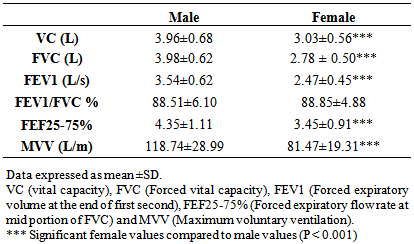
Table (2) shows the mean values (± SD) of all the measured parameters: VC, FVC, FEV1, FEV1/FVC%, FEF 25-75% and MVV. It is clear that male values are significantly higher than female values in all measured parameters (P < 0.001) except FEV1/FVC ratio where there was no significant difference.Table 2. Mean values ± SD of VC, FVC, FEV1, FEV1/FVC%, FEF25-75% and MVV in male and female subjects
 |
| |
|
On studying the effect of sex, age, height and weight as independent factors on the respiratory parameters, it was found that VC, FVC, FEV1, FEF25-75% and MVV have a significant correlation with sex, height and weight of subjects (P<0.001 for all). However, none of the parameters showed significant correlation with age. On the other hand, FEV1/FVC % ratio showed no significant correlation with any of the independent factors (Table 3), although when multiple regression analysis was done FEV1/FVC % showed significant coefficients with height and weight (P<0.001).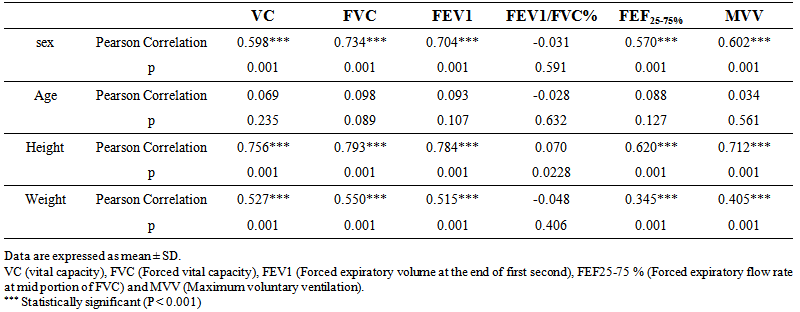 | Table 3. Correlation coefficients (Pearson) and significance of VC, FVC, FEV1, FEV1/FVC, FEF25-75% and MVV versus sex, age, height and weight in all subjects |
In the regression models, height and sex were found to be important independent variables for all pulmonary function parameters. The addition of weight to the regression models offered lower but significant improvement to the model fit. However, age has no significant correlation with any parameter and when added to the regression models, it did not offer any significant improvement to the model fit. So, only height, sex and weight were used in the reference equations for lung function parameters (figs. 1-12).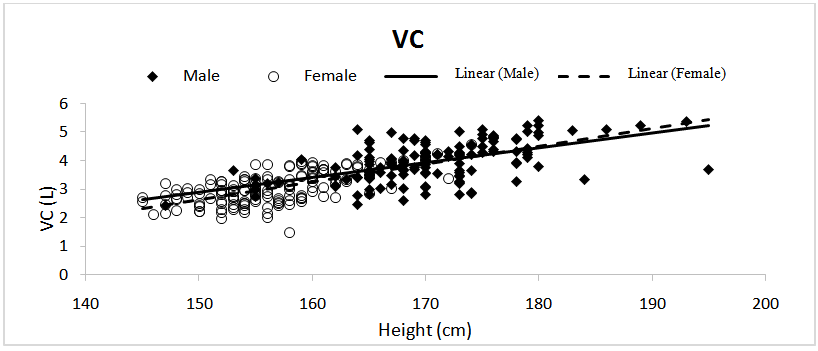 | Figure 1. Correlation between vital capacity (VC) and height in males and females subjects |
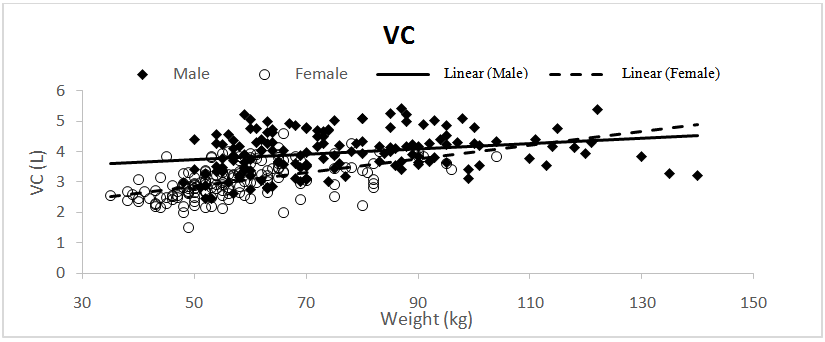 | Figure 2. Correlation between vital capacity (VC) and weight in males and females subjects |
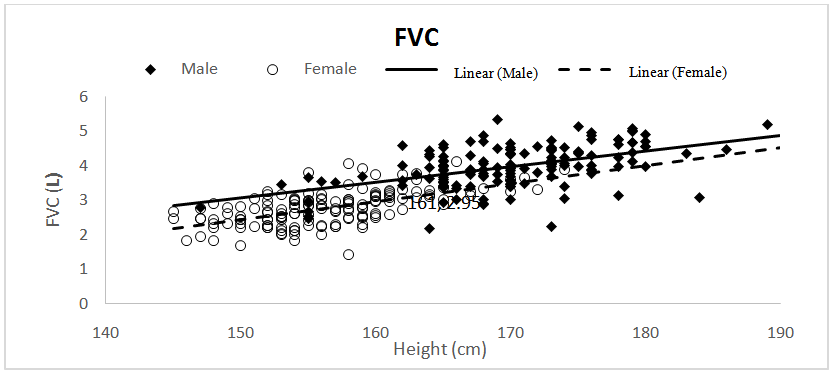 | Figure 3. Correlation between Forced vital capacity (FVC) and height in males and females subjects |
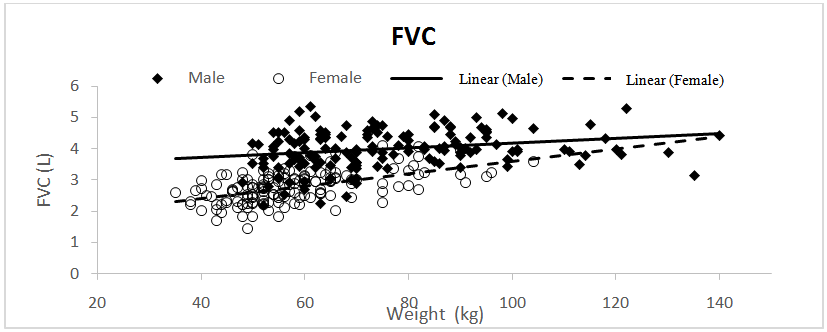 | Figure 4. Correlation between Forced vital capacity (FVC) and weight in males and females subjects |
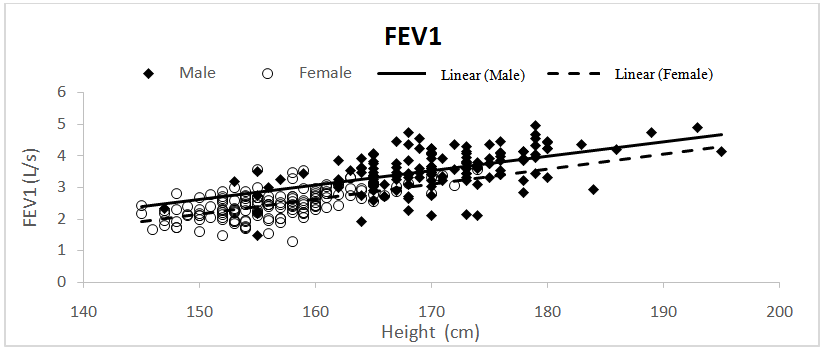 | Figure 5. Correlation between Forced expiratory volume at first second (FEV1) and height in males and females subjects |
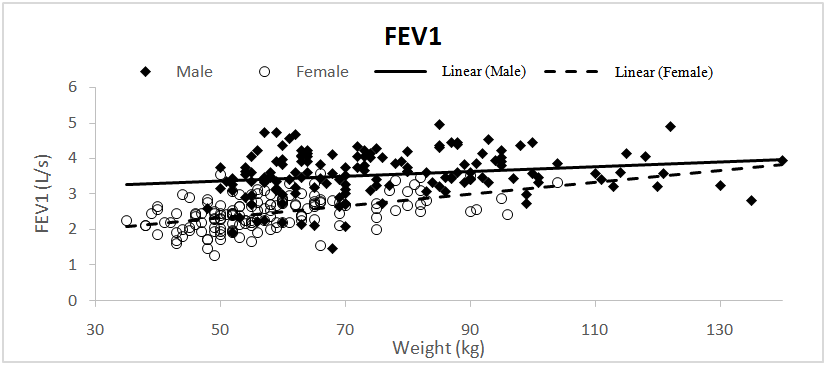 | Figure 6. Correlation between Forced expiratory volume at first second (FEV1) and weight in males and females subjects |
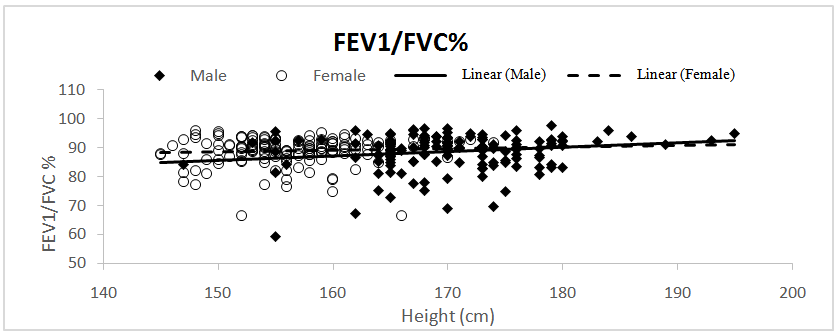 | Figure 7. Correlation between percentage of Forced expiratory volume at first second to forced vital capacity (FEV1/FVC%) and height in males and females subjects |
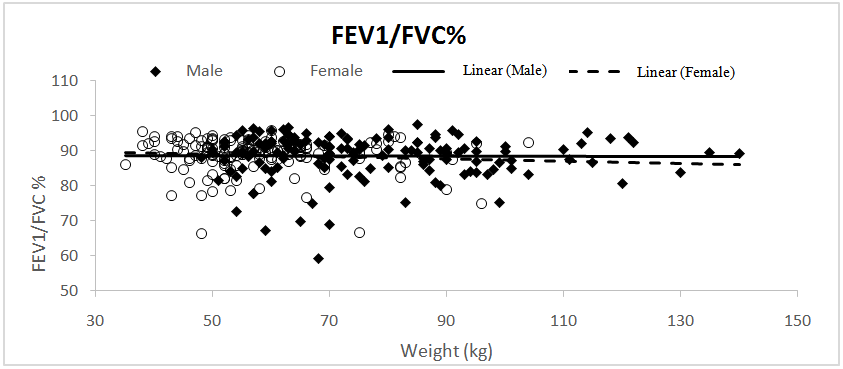 | Figure 8. Correlation between percentage of Forced expiratory volume at first second to forced vital capacity (FEV1/FVC%) and weight in males and females subjects |
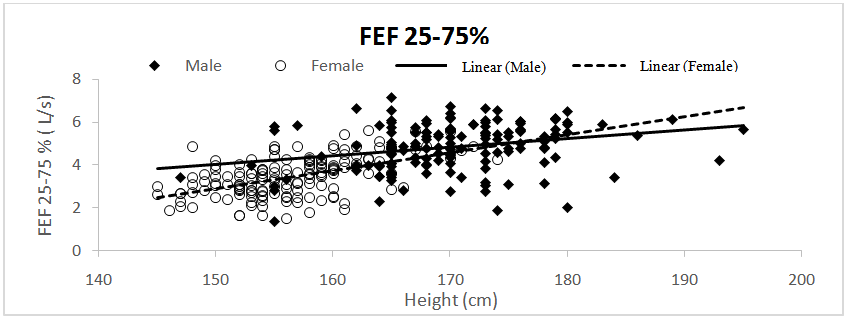 | Figure 9. Correlation between Forced expiratory flow at mid portion of FVC (FEF25-75 %) and Height in males and females subjects |
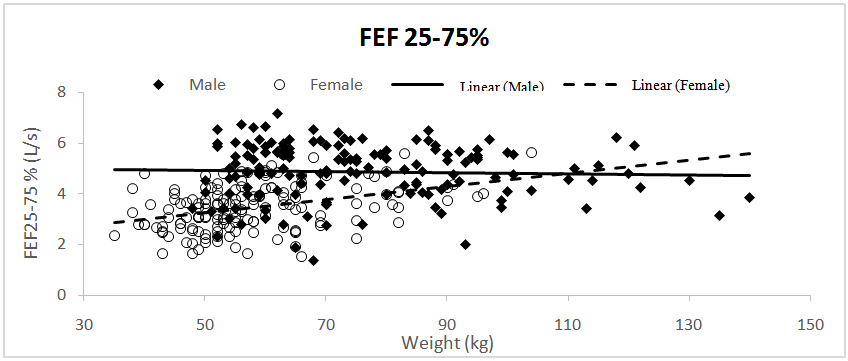 | Figure 10. Correlation between Forced expiratory flow at mid portion of FVC (FEF25-75 %) and weight in males and females subjects |
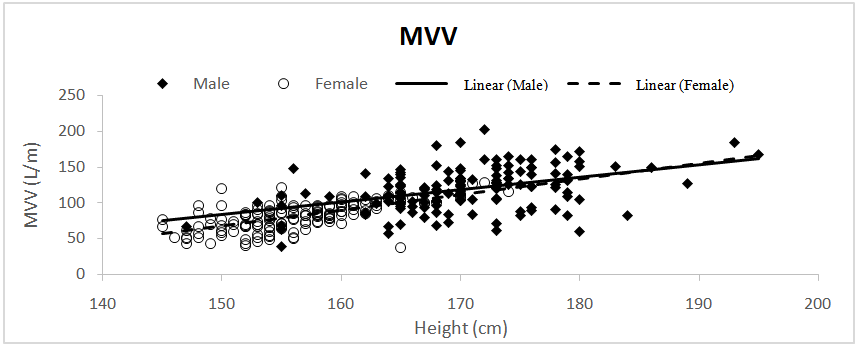 | Figure 11. Correlation between Maximum voluntary ventilation (MVV) and Height in males and females subjects |
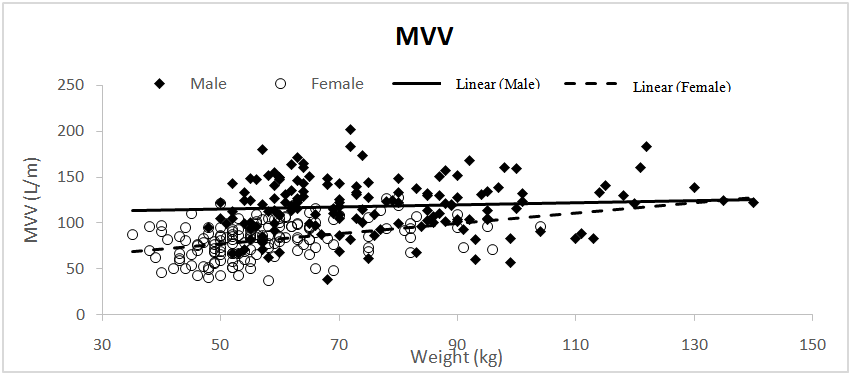 | Figure 12. Correlation between Maximum voluntary ventilation (MVV) and weight in males and females subjects |
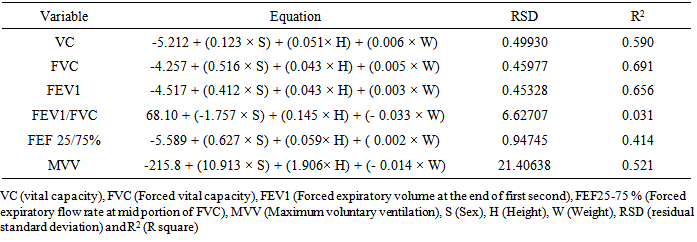
As regards FEV1/FVC ratio, it was found that sex did not significantly correlate to this parameter. On performing, the multiple regression analysis it was found that regression coefficient for sex was also not significant so we used only height and weight as predictors for this parameter. Results of regression analysis for lung function parameters (FVC, FEV1, FEV1/FVC%, FEF 25-75% and MVV) for all subjects are shown in table (4).Table 4. Prediction equations for spirometric parameters in the present study
 |
| |
|
We can estimate each lung function value by using the following equation: X = a + b × H + c × S +d × WWhere, (x) is the mean predicted lung function value, (a) is a constant, and (b, c, d) are the, regression coefficients for height, sex and weight respectively. In the equations, S is substituted with (1) in case of male and (0) in case of female. This equation apply to male subjects with age range 18-25 y, height, 147-195 cm and body weight, 48-140 Kg and female subjects with age range 18-24 y, height 145-174 cm and body weight 35-104 Kg.Then, we compared the results of the current study with other results derived from prediction equations for other ethnic groups (Caucasian, African and Japanese). The predicted values for all groups were calculated using male height 170 cm and weight 75 kg and a female height 155 cm and weight 58 kg. The age value for both males and females was 20 y. The data were compared as a percentage difference. As shown in table (5), when we calculate the percentage difference between the different groups we found that the predicted values for Saudi adults are lower for both male and female subjects than Caucasian, African and Japanese subjects for most of the parameters tested, the greatest difference was that calculated between Saudi adults and Caucasians. However, for FEV1/FVC% and FEF25-75%, the male Saudi adults where higher than the other ethnic groups, while in Saudi female subjects VC was found to be higher than African and Japanese females and FEV1/FEV% was higher than all the other groups.
X = a + b × H + c × S +d × WWhere, (x) is the mean predicted lung function value, (a) is a constant, and (b, c, d) are the, regression coefficients for height, sex and weight respectively. In the equations, S is substituted with (1) in case of male and (0) in case of female. This equation apply to male subjects with age range 18-25 y, height, 147-195 cm and body weight, 48-140 Kg and female subjects with age range 18-24 y, height 145-174 cm and body weight 35-104 Kg.Then, we compared the results of the current study with other results derived from prediction equations for other ethnic groups (Caucasian, African and Japanese). The predicted values for all groups were calculated using male height 170 cm and weight 75 kg and a female height 155 cm and weight 58 kg. The age value for both males and females was 20 y. The data were compared as a percentage difference. As shown in table (5), when we calculate the percentage difference between the different groups we found that the predicted values for Saudi adults are lower for both male and female subjects than Caucasian, African and Japanese subjects for most of the parameters tested, the greatest difference was that calculated between Saudi adults and Caucasians. However, for FEV1/FVC% and FEF25-75%, the male Saudi adults where higher than the other ethnic groups, while in Saudi female subjects VC was found to be higher than African and Japanese females and FEV1/FEV% was higher than all the other groups.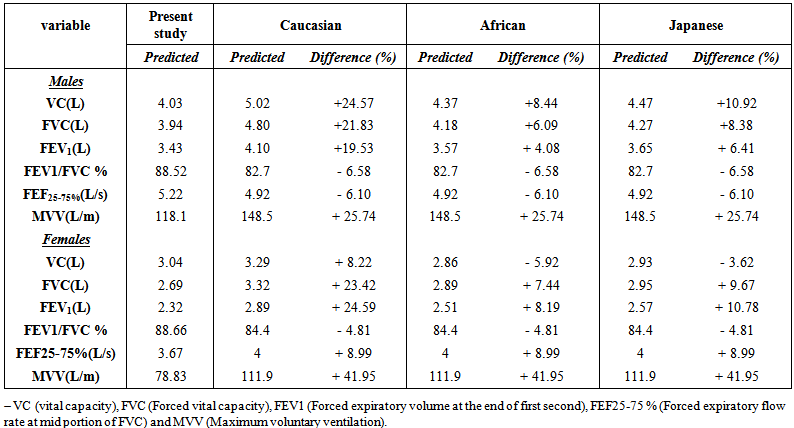 | Table 5. Comparison of the predicted values of the present study and other ethnic groups |
4. Discussion
In the current study, we generated a reference value for spirometric parameters for Saudi adults living in Tabuk region in Saudi Arabia, and then we compared our results with that of some other ethnic groups. Our prediction equations were derived by relating age, sex, height and weight as independent factors to the respiratory function parameters (VC, FVC, FEV1, FEV1/FVC%, FEF25-75% and MVV). These results were obtained by testing 300 healthy adults (150 male and 150 female) for respiratory functions using oral spirometry. Sex was an important factor affecting most of the parameters of spirometry. VC, FVC, FEV1, FEF25-75% and MVV were significantly lower in females than males, while the percentages of FEV1/FVC showed no significant difference. The differences between male and female parameters could be explained by differences in fat-free mass, chest dimensions and power of respiratory muscles [18]. On the other hand, the factors affecting FVC and FEV1 are the same in males and females so the ratio showed no significant difference. On applying the age as an independent factor, it was found that age was not an effective factor on the respiratory parameters in the current study and when it was added to the regression models, it did not offer any significant improvement to the model fit and this is why age is not included as a predictor. Like other studies in which the factor of age was not effective [19], this could be attributed to the narrow age range in our study 18-25 years and 22-33 years in Korotzer et al. study [19]. Falaschetti et al. [20] denoted that usually adult reference values are used from the age of 18 years, although this does not reflect the relationship between age, lung function growth and body size. However, age was an effective independent variable in a study by Hankinson et al. [3] on a sample of the U.S. population that covered a wide age range (8-80 years). When the different parameters of nasal spirometry were evaluated against the factor of height, it was found to affect all the parameters by a positive relationship. In several other studies, height was also shown to be an important variable affecting the parameters of oral spirometry [18, 21, 22]. In contrast, the effect of weight was small, but significant. Weight significantly affected VC, FVC, FEV1, FEF25-75% and MVV. From Table 3, it can be seen that all of the parameters affected by weight were affected primarily by height. So, the positive effect of weight could be explained by accompanying increase in height. In a study by Falaschetti et al. [20], they reported no relationship between weight and lung function, although height was effective. This may be due to the large number of subjects that includes many elder persons.On comparing our results with other different ethnic groups, it was clear that the predicted values for Saudi adults are lower for both male and female subjects than Caucasian, African and Japanese subjects for most of the parameters tested. The greatest difference was that calculated between Saudi adults and Caucasians while data obtained from subjects with African descent and Japanese persons were more or less nearer to Saudi data. These results are similar to results obtained from other studies with different ethnic groups like African, Asian, and African Americans [3, 19, 23], whose values were also less than those obtained from Caucasian. This could be explained by the fact that the Caucasians have larger trunk to leg ratio at a given height, which could be attributed to some genetic factors that may control body shape [3]. However, according to Stanojevic et al. [2] sitting height was not found to explain the variability observed in Asian subjects. In addition, difference in chest dimensions did not explain the effect of ethnicity on lung functions [24]. However, environmental factors like nutrition, exercise, air quality and occupational exposure may count for the difference [11]. This may also be applied for the explanation of the difference between Saudi, African and Japanese persons.On the contrary, the higher values for FEV1/FVC% and FEF 25-75% in Saudi males over that of the corresponding Caucasian values, were found to be in agreement with other previous Saudi study [13]. This observation was not restricted to Saudi or even other Arab studies, but was also in agreement with ATS statement [25], which concluded that most races show similar or higher FEV1/FVC% compared to Caucasian races. However, the FEV1/FVC% depends on the ratio between the maximum effort in the first second (needed for FEV1) and the sustained effort needed for the whole FVC, the later may be better in Caucasian than other ethnic groups.In Saudi female subjects, VC was found to be higher than African and Japanese females and this could be because slow VC needs slow maintained effort of moderate intensity, which could be more efficient in Saudi females than Japanese and African ethnic groups. Also, and like male subjects FEV1/FEV% was higher in Saudi females than all the other groups.
5. Conclusions
A considerable difference was found between prediction equations and reference values obtained in the present study and other ethnic groups as Caucasian, African and Japanese. Therefore, pulmonary function reference values and prediction equations were derived for both sexes between the ages 18-25 years in healthy non-smoker Saudi adults. This will provide accurate interpretation for lung functions in this population.
6. Recommendations
We recommend that our prediction equations could be used to estimate the reference value for spirometric parameters in adult Saudi persons. We recommend also that further studies are necessary to cover a wider age range so that Saudi people can have their specific reference values that help in proper assessment of lung functions.
References
| [1] | Quanjer PhH, Stanojevic S, Cole TJ, Baur X, Hall GL, Culver BH, Enright PL et al. Multi-Ethnic Values for Spirometry For The 3-95 Year Age Range: The Global Lung Function 2012 Equations: Report of the Global Lung Function Intiative (GLI), ERS Task Force to establish improved Lung Function Reference Values. Eur.Respir. J. 2012; 40(6):1324-1343. |
| [2] | Stanojevic S, Wade A, Stocks J. Reference values for lung function: past, present and future. Eur. Respir. J. 2010; 36(1):12-19. |
| [3] | Hankinson JL, Odencrantz JR, Fedan KB. Spirometric reference values from a sample of the general U.S. population. Am. J. Respir. Crit. Care Med. 1999; 159(1): 179-87. |
| [4] | Degens P, Merget R. Reference values for spirometry of the European Coal and Steel Community: time for change. Eur Respir J 2008; 31(3):687-688. |
| [5] | Pereira CA, Sato T, Rodrigues SC. New reference values for forced spirometry in white adults in Brazil. SCJ Bras Pneumol. 2007; 33(4):397-406. |
| [6] | Gibson J, Gallagher H, Johansen A, Webster I.: Lung function in an Australian population: 1. Spirometric standards for non-smoking adults. Med J Aust. 1979; 1(7):292-5. |
| [7] | Boskabady MH, Keshmiri M, Banihashemi B, Anvary K. Lung function values in healthy non-smoking urban adults in iran. Respiration 2002; 69(4):320-6. |
| [8] | Aggarwal AN, Gupta D, Jindal SK Comparison of Indian reference equations for spirometry interpretation. Respirology 2007; 12(5):763-8. |
| [9] | Memon MA, Sandila MP, Ahmed ST. Spirometric reference values in healthy, non-smoking, urban Pakistani population. J Pak Med Assoc. 2007; 57(4):193-5. |
| [10] | Sliman NA, Dajani BM, Dajani HM. Ventilatory function test values of healthy adult Jordanians. Thorax 1981; 36:546-9. |
| [11] | Al-Rawas OA, Baddar S, Al-Maniri AA, Balaji J, Jayakrishnan B, Al-Riyami BM. Normal spirometric reference values for Omani adults. Lung 2009; 187(4): 245-51. |
| [12] | Haddock DRW, Al-Hadramy MS, Macfarlane SB. Normal spirometric values investigated in King Abdul-Aziz Teaching Hospital, Jeddah. Saudi Med. J. 1982; 3:159-170. |
| [13] | Abdullah AK, Abedin MZ, Nouh MS, Al-Nozha M. Ventilatory function in normal Saudi Arabian adults. Observations and comparison with some Western and Eastern reference values. Trop. Geogr. Med.1986; 38(1):58-62. |
| [14] | Al-Fayez SF, Kassimi MA, Ardawi MS: Normal spirometry values in saudi nationals in the western region of saudi Arabia. Saudi Med. J. 1989; 10(2): 129-133. |
| [15] | Standardized lung function testing. Official statement of the European Respiratory Society. Eur. Respir. J. 1993; 16: 1-100. |
| [16] | Miller MR, Crapo R, Hankinson J, V. Brusasco, F. Burgos, R. Casaburi, A. Coates, P. Enright, C.P.M. van der Grinten, P. Gustafsson, R. Jensen, D.C. Johnson, N. MacIntyre, R. McKay, D. Navajas, O.F. Pedersen, R. Pellegrino, G. Viegi and J. Wanger. General considerations for lung function testing. Eur. Respir. J. 2005; 26: 153-161. |
| [17] | Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, Crapo R, Enright P, van der Grinten CP, Gustafsson P, Jensen R, Johnson DC, MacIntyre N, McKay R, Navajas D, Pedersen OF, Pellegrino R, Viegi G, Wanger J. Standardisation of spirometry. Eur. Respir. J. 2005; 26(2): 319-38. |
| [18] | Stocks J, Quanjer PhH. Reference values for residual volume, functional residual capacity and total lung capacity. ATS Workshop on lung volume measurements. Official Statement of the European Respiratory Society. Eur. Respir. J. 1995; 8(3):492-506. |
| [19] | Korotzer B, Ong S, Hansen JE Ethnic differences in pulmonary function in healthy nonsmoking Asian-Americans and European-Americans. Am. J. Respir. Crit. Care Med. 2000; 161(4 Pt1):1101-8. |
| [20] | Falaschetti E, Laiho J, Primatesta P, Purdon S. Prediction equations for normal and low lung function from the Health Survey for England. Eur. Respir. J. 2004; 23(3): 456-63. |
| [21] | Kuster SP, Kuster D, Schindler C, Rochat MK, Braun J, Held L, Brändli O. Reference equations for lung function screening of healthy never-smoking adults aged 18-80 years. Eur. Respir. J. 2008; 31(4):860-8. |
| [22] | Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, Coates A, van der Grinten CP, Gustafsson P, Hankinson J, Jensen R, Johnson DC, MacIntyre N, McKay R, Miller MR, Navajas D, Pedersen OF, Wanger J. Interpretative strategies for lung function tests. Eur. Respir. J. 2005; 26(5):948-68. |
| [23] | Yang TS, Peat J, Keena V, Donnelly P, Unger W, Woolcock A. A review of the racial differences in the lung function of normal Caucasian, Chinese and Indian subjects. Eur. Respir. J. 1991; 4(7):872-80. |
| [24] | Whittaker AL, Sutton AJ, Beardsmore CS. Are ethnic differences in lung fuction explained by chest size?. Arch Dis. Child Fetal Neonatal Ed. 2005; 90(5):F423-F428. |
| [25] | American Thoracic Society. Lung function testing: selection of reference values and interpretative strategies. ATS Statement. Am. Rev. Respir. Dis. 1991; 144(5):1202-18. |
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML