-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Internal Medicine
p-ISSN: 2326-1064 e-ISSN: 2326-1072
2014; 3(2): 27-30
doi:10.5923/j.ijim.20140302.01
A Rare Case of a Pelvic Tumour Presenting as Incidental Right Atrial Mass on Routine Echocardiogram
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLIshaq Mohammed1, Eleni Syrimi2, Nurulizzah Ibrahim3, Mahrous Alsoud4
1MBBS MD MRCP, 65 Elmbridge Road, Birmingham UK, B44 8AH
2MD, Stafford Hospital, Weston Road, Stafford, UK, ST16 3SA
3MBBch BAO, Stafford Hospital, Weston Road, Stafford, UK, ST16 3SA
4MRCP, Stafford Hospital, Weston Road, Stafford, UK, ST16 3SA
Correspondence to: Ishaq Mohammed, MBBS MD MRCP, 65 Elmbridge Road, Birmingham UK, B44 8AH.
| Email: |  |
Copyright © 2014 Scientific & Academic Publishing. All Rights Reserved.
We present a case of 54 yr old Caucasian female who came for a routine echocardiogram requested by the primary care physician for mild shortness of breath following a chest infection.Routine echocardiogram revealed a mass like shadow in right atrium protruding into right ventricle across the tricuspid valve. It was seen coming from the IVC into right atrium. Trans oesophageal echocardiogram confirmed the findings. The shadow was not homogenous and consisted of cystic type of filling defects within, raising the suspicion of a malignant neoplasm. Patient went on to have further tests like full body CT scan and CT guided biopsy. The diagnosis was confirmed as extensive pelvic leiomyoma invading the heart via ovarian vein, iliac vein, inferior venacava and into right side of heart. Patient is awaiting major cardiovascular and abdominal surgery.
Keywords: Pelvic mass, Leiomyoma, Intravascular spread, Incidental right heart mass, Chemotherapy, Surgery, IVC-Inferior vena cava
Cite this paper: Ishaq Mohammed, Eleni Syrimi, Nurulizzah Ibrahim, Mahrous Alsoud, A Rare Case of a Pelvic Tumour Presenting as Incidental Right Atrial Mass on Routine Echocardiogram, International Journal of Internal Medicine, Vol. 3 No. 2, 2014, pp. 27-30. doi: 10.5923/j.ijim.20140302.01.
Article Outline
1. Learning Objectives
- Echocardiogram and transesophageal echocardiogram are excellent investigations to diagnose intracardiac tumours. Not all intracardiac masses arise from the heart. They can arise from different areas of the body and can present as intra cardiac masses. Asymptomatic patients can have serious underlying conditions. Degree of clinical suspicion is needed to pick up cues from history, clinical examination and basic investigations to investigate further for more serious conditions. Cardiac tumours provide unique diagnostic and therapeutic challenges.
2. Introduction
- Intravascular leiomyomatosis is rare, both benign and malignant variants of this tumour have been described in literature. Characterised by uncontrolled smooth muscle proliferation into the pelvic veins and then with intravascular extension, this can grow as far as up to heart from pelvis. This case is important because it was picked up on a routine echocardiogram arranged by primary care physician. The diagnosis came as a shock to the patient who was feeling absolutely fine without any symptoms. Also this case is one of only first few cases from UK and is rare. Particularly the presentation is unique in this case. This case has learning point in that a subtle shadow on routine echocardiogram can lead to a very sinister pathology like extensive pelvic tumour. It has lot of psycho social impact on patients. Now patient is left with the challenge of a very major invasive surgery involving various teams including cardiothoracic, vascular and gynaecological surgeons.Aim of the study is to increase awareness that subtle symptoms can lead to sinister pathology and any mass like shadow seen on routine echocardiogram needs a full evaluation by cardiologist.
3. Case History
- We present a case of 54 yr old Caucasian female who came for a routine echocardiogram requested by the primary care physician for mild shortness of breath following a chest infection. There were no other troubling symptoms of importance and also her past history was insignificant.
4. Methods
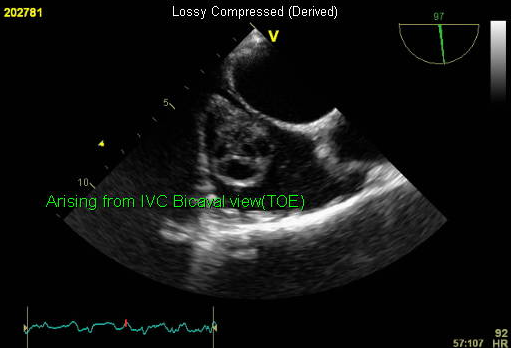
- Routine echocardiogram revealed a mass like shadow in right atrium protruding into right ventricle across the tricuspid valve. It was seen coming from the IVC into right atrium. Patient was admitted for Trans oesophageal echocardiogram which confirmed the findings (Fig.1). The shadow was not homogenous and consisted of cystic type of filling defects within IVC, raising the suspicion of a malignant neoplasm.
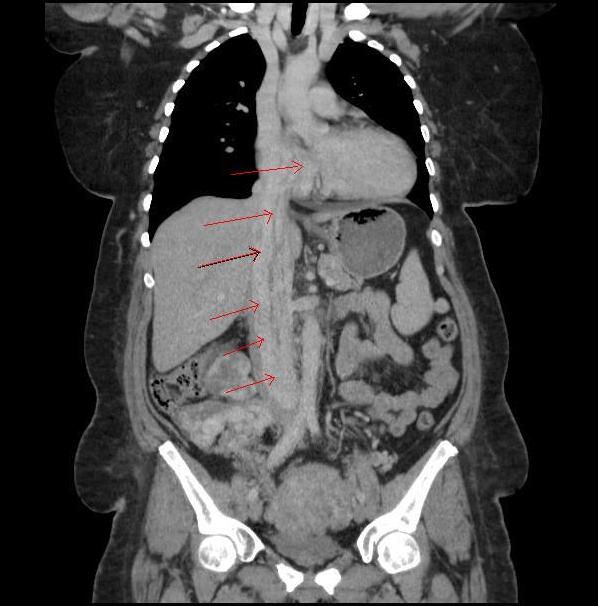
 | Figure 1. CT image showing a hyper vascular mass with calcification within involving the right adnexa and uterus and extending up the IVC, into the right atrium. Within the IVC are multiple linear structures enhancing the tumour |
 | Figure 2. Transesophageal echocardiogram image of Right atrium (Bicaval view) showing Inferior vena cava at top and Superior vena cava at bottom. Mass can be seen arising out of IVC |
5. Procedure
- Whilst CT scan of abdomen is a standard imaging modality to investigate intra abdominal masses, the sequence of investigations conducted was as follows-Transthoracic echocardiogram, Trans oesophageal echocardiogram (Fig.2), CT scan of brain, chest, abdomen and pelvis (Fig.1). Then patient had CT guided biopsy. Patient had CT guided right side nephrostomy done to treat hydronephrosis on same side which was caused by mechanical pressure on ureters.She had repeat CT scan after a trial therapy with anti estrogens.Initial suspicion was of right atrial myxoma but after investigations it confirmed a pelvic leiomyoma with intravascular growth and extension into right heart.This tumour was large in size with calcification within and intravascular extension through the ovarian vein into the inferiorvena cava and going into right atrium (Fig.1). This is well described in literature and only thing unusual in our case was the extension through the tricuspid valve in diastolic phase into right ventricle which was the cause of shortness of breath in this patient.
6. Results
- Patient is scheduled for major cardiovascular surgery to remove the tumour after she had initial anti oestrogen treatment. Patient is on Close follow up with Oncology, Gynaecology and cardiothoracic surgery. She needed a nephrostomy procedure to relieve the right sided hydronephrosis due to mechanical obstruction by the tumour.
7. Discussion
- Leiomyomas can grow intravascularly, are peculiarly rare, originating from uterus and growing intravascularly [1]. Suspected case of atrial myxoma which is commonest of space occupying lesions in left and right atria should always be followed up with TOE to ascertain the origin and nature of lesions and also CT imaging of abdomen, pelvis and chest [2, 3].This patient of ours had CT guided biopsy of the pelvic mass which confirmed the diagnosis of intravascular leiomyoma.There are case reports in literature describing the spread of pelvic leiomyomas and leiomyosarcomas to right heart2 but in our case it was an incidental pick up of right atrial mass on a routine echocardiogram that led to diagnosis on further investigations. This makes our case unique and first of this type of presentation.Malignant tumours are mostly sarcomatous in nature [4]. In spite of resections (complete or incomplete), median survival duration ranges from 10-24 months and recurrences are common.We believe that all cases of incidental mass in the right atrium should have in the first instance a full body CT scan and Tran oesophageal echocardiogram to ascertain the diagnosis and to make sure there is no pathology elsewhere in the body as demonstrated in our case report. Cardiac MRI is also a useful tool for diagnosis and further evaluation of intracardiac masses [4, 5].Usually Right atrial mass like shadow is a right atrial myxoma, thrombus, fibromas, secondary tumours or rare primary tumours [4]. The most common primary cardiac tumour is the atrial myxoma, which accounts for 40-50% of all these neoplasms [4]. The overall incidence of primary cardiac neoplasms is low (0.0001-0.5% in autopsy series). If right atrial mass is identified in a patient with prior hysterectomy secondary to leiomyomatosis or in a patient with history of uterine fibroids then intra vascular leiomyoma extending into right atrium should be strongly considered.Rhabdomyoma, fibroma, fibroelastoma, haemangioma, lipoma, teratoma, and hamartoma etc are benign tumours [4], and mortality rates in patients with these tumours do not differ significantly from that of the general population.Commonest Intracardiac lesion/shadow on echo which is non neoplastic is clot or a thrombus. It is usually associated with impaired LV function and or Atrial fibrillation atrial flutter, post MI (Aneurysmal LV), Valve diseases etc.More and more thrombi are being diagnosed and treated as more heart failure patients are being diagnosed and treated & more CRT pacemakers are being put in and heart failure patients are living longer.Similar cases have been reported from different parts of world but very few cases from UK [6]. Most of them are intravascular growing tumours into IVC and into right atrium with calcification [1, 7, 8].Long-term follow-up is essential for these patients and also familiarity with rare forms of benign smooth muscle uterine tumours is essential to correctly diagnose and treat these patients accordingly [9]. Some tumours have been treated with one stage procedure of median sternotomy (cardiotomy) with by-pass support and laparotomy and is increasingly recognised as standard surgical approach for immediate management [10].
ACKNOWLEDGEMENTS
- Helen Daniel Senior Staff Nurse, Cath lab, Stafford Hospital.