-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Clinical Psychiatry
p-ISSN: 2332-8355 e-ISSN: 2332-8371
2018; 6(3): 57-61
doi:10.5923/j.ijcp.20180603.03

Prevalence and Comparison of Problematic Cell Phone Use amongst University Students in Western U.P Region in India: Correlates with Stress and Anxiety
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLPrerana Gupta, Jigar Haria, Swati Singh
Teerthanker Mahaveer Medical College, U.P. India
Correspondence to: Prerana Gupta, Teerthanker Mahaveer Medical College, U.P. India.
| Email: |  |
Copyright © 2018 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Introduction: Since their introduction 12 years ago, there has been a wide proliferation of uptake of cell phone usage in India. Studies acknowledging excessive and problematic use of cell phone have also been reported from various parts of world. Systematic studies from India are still sparse. Aims: The present study aims to target the young cohort of university students pursuing education in a prominent deemed university of Northern India and to find the prevalence of cell phone addiction in the various groups of students belonging to various streams of education. Materials and methods: 50 students with age groups ranging from 18-24 were selected on a random basis by lucky draw method. They were explained the nature of study and its purpose and a 24 item self report questionnaire prepared on lines from ICD-X and CAGE questionnaire was administered to them after taking a informed consent. They were also administered Perceived Stress Scale and Hamiltons Anxiety Rating Scale to measure stress and anxiety. Results: Female students scored significantly higher on the dependence criteria. Female students scored significantly higher on the dependence criteria. Stream of study, type of family and monthly allowance of the students had no major role in the development of cell phone dependence in the sample. There was no significant correlation between the perceived stress of the students and the development of cell phone dependence. There was a significant relation between anxiety and high level of cell phone dependence Conclusion: Increasing cell phone usage among young students to the levels of cell phone dependence is a cause of much concern for the society especially when seen in conjunction with the higher levels of anxiety seen in this group.
Keywords: Problematic Cell Phone use, Cell phone dependence, Anxiety, Stress
Cite this paper: Prerana Gupta, Jigar Haria, Swati Singh, Prevalence and Comparison of Problematic Cell Phone Use amongst University Students in Western U.P Region in India: Correlates with Stress and Anxiety, International Journal of Clinical Psychiatry, Vol. 6 No. 3, 2018, pp. 57-61. doi: 10.5923/j.ijcp.20180603.03.
Article Outline
1. Introduction
- Since their introduction 12 years ago, there has been a wide proliferation of uptake of cell phone usage in India [1]. According to the statistics, India has the second largest cell phone customer base, after China and this base is expanding fast. There are currently 929.37 million users (74.71% of total population) in India [1]. Telecom subscription data from TRAI indicate 8.35 million new additions monthly [1]. There are a number of reasons for this prolific popularity of this communication technology. Decreasing costs, good network coverage, multiple uses of the cell phone and availability of non-communication purposes have increased the user potential.Negative effects of cell phone use like lowered concentration, headache and insomnia due to night time use are widely documented [2-6]. Studies acknowledging excessive and problematic use of cell phone have also been reported from various parts of world [7-11].Systematic studies from Indi are still sparse and have mainly focussed on the dependence potential of internet [12]. Cell phone dependence study amongst resident doctors, 39.6% met 3 or more of ICD-X diagnostic criteria for substance dependence [13].Cell phones are integral to the social functioning of young individuals today as having cell phones allows them to be contactable by their friends aiding in the formation and maintenance of social groups [14, 15]. This young population has shown a steep rise in cell phone use in terms of frequency and harmfulness [16]. Recent ACMA Report has shown that young people have reported that they are heavily dependent on their cell phones and could not imagine living without it. Some have said that they cannot turn their phone off and they feel anxiety when they are unable to use their phone [17, 18].The term behavioural addiction has been applied to describe a wide range of behaviours which are excessive and harmful to the user, including eating [19], exercise [20], Internet use [21-23], sex [24], shopping [25]. Technological addictions are defined as non-substance addictions involving excessive human computer interactions and are finding a place in the subset of behavioural addictions [21, 26], though they are still to find a place in the current diagnostic manuals. Despite the differences in literature, excessive or addictive technological use is related to an expected reduction in difficult states such as loneliness and benefits from use such as social inclusions [21]. High interpersonal anxiety has been seen in excessive cellphone use [27] and individuals suffering from clinical anxiety are likely to exhibit heavy cell phone use [28].
2. Objectives of Study
- The present study aims to target the young cohort of university students pursuing education in a prominent deemed university of Northern India and to find the prevalence of cell phone addiction in the various groups of students belonging to various streams of education. It also aims to compare these groups in term of their Problematic Smartphone use and also to find correlates between stress and Problematic Smartphone use and presence of psychiatric co morbidity of Anxiety amongst the various groups.
3. Study Design and Participants
- 50 students with age groups ranging from 18-24 were selected on a random basis from the university premises by lucky draw method. The students belonged to the Medical college, Nursing college, Dental college and engineering college of the University which is located in Moradabad, Uttar Pradesh India. 95% of the sample resided in hostels and were from various parts of India and rest 5% were residing in or around Uttar Pradesh. They were explained the nature of study and its purpose and a 24 item self report questionnaire prepared on lines from ICD-X [29] and CAGE [30] questionnaire would be administered to them after taking a informed consent. They were also administered Perceived Stress Scale and Hamiltons Anxiety Rating Scale to measure stress and Anxiety.Inclusion Criteria:1. Possessing atleast one Smartphone for the last 1 month2. Using their Smartphone atleast once a dayExclusion Criteria:1. Those suffering from any psychiatric disorder and taking treatment for it in the last one month.Tools:1. Self designed performa containing sociodemographic details,2. Cell phone dependence Questionnaire containing 27 items. First 4 items enquiring about duration and reasons for cell phone use, next three items focussing on finances spent on usage of cell phone and the other items corresponding to ICD-X research criteria for substance dependence and CAGE questionnaire. The last item enquired about other substances used by the cohort. 3. Perceived Stress Scale4. Hamiltons Anxiety Rating ScaleStatistical Analysis:The frequencies and percentages were calculated from data. Comparisons were done by using Chi Square tests. Associations between various variables were computed using Pearsons co-relation coefficient.
4. Results
|
|
|
|
|
|
|
|

5. Discussion
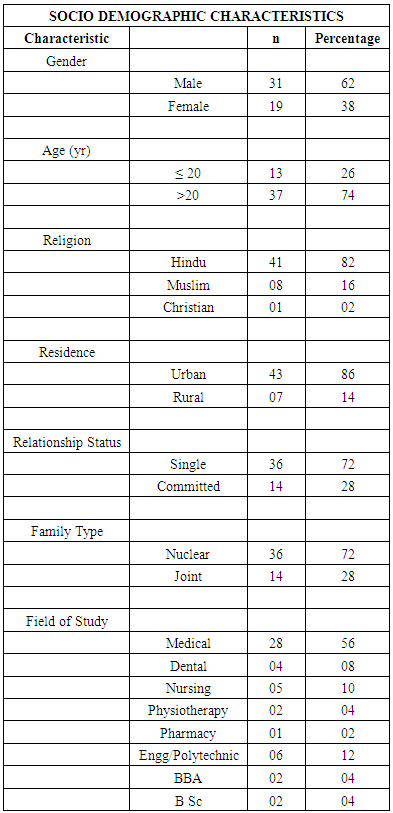
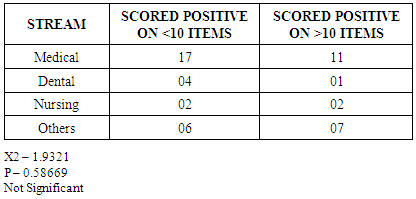
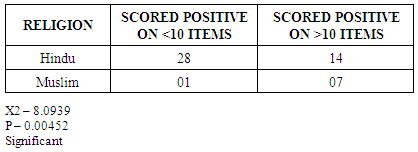
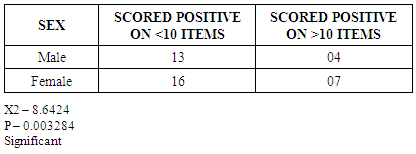
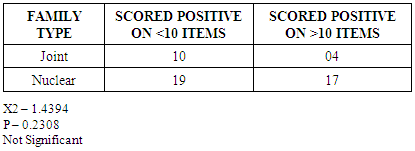
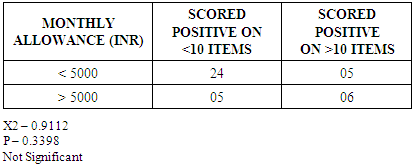
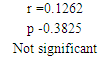
- Technological Addictions are on the rise in today’s developing world.Almost 100% of our sample possessed a cell phone. Mean age of our sample was 22.5 years with 62% males and 38% females. 72% of the sample was single. 92.5% had a cell phone for 3 years or more. 95% of the sample was residing in the various hostels in the university campus itself. Most of the sample was Hindu which were 82% of thge sample. (Table 1)88% of the sample reported the main use of the cell phone to communicate with family and friends while the remaining sample attributed the main use of internet usage. 92% of the sample had an average daily use of 2 hours or more. 68% of the sample met 4 or more criteria for dependence. 42% of the sample met 10 or more criteria for dependence.Female students scored significantly higher on the dependence criteria (table 4). This is in accordance with the previous studies [29], where various reasons have been attributed to more significance of cell phones in females who use it majorly to remain in touch with family and friends.Female students scored significantly higher on the dependence criteria (table 3). This is the first study to find the impact of religion in development of technological addiction. Religiosity, in general has been found to have a negative factor in the development of alcohol and nicotine addictions [29]. Higher levels of personal devotion amongst Muslims could be one of the reasons for higher levels of cell phone dependence amongst this group though this finding needs to be evaluated further by conducting larger sample and matched studies.Stream of study, type of family and monthly allowance of the students had no major role in the development of cell phone dependence in the sample. This is an interesting finding as the cost of cell phone bills seem to have no influence on the development of cell phone dependence in the sample. (table 2, 5 & 6)There was no significant correlation between the perceived stress of the students and the development of cell phone dependence (Table 7). This is not in accordance with the previous studies which have shown a higher amount of stress in individuals having higher level of dependence on their cell phones (ref). This could be attributed to the fact that cell phone usage has become ubiquitous in the current generation and on the contrary more cell phone usage could lead to lower the levels of stress in the sample by producing meaningful social interactions.There was a significant relation between anxiety and high level of cell phone dependence (Table 8). This is in accordance with the previous studies [27, 28] which have concluded that higher levels of anxiety lead to more heavy cell phone usage in the sample.
6. Conclusions
- The young adults of a population are the major contributors in the development of the nation. Professionals form the major workforce of any nation. Increasing problematic smart phone use among this workforce to the levels of cell phone dependence is a cause of much concern for the society especially when seen in conjunction with the higher levels of anxiety seen in this group. There is an increased risk of Problematic Smart Phone use in females and this carries social implications and also the fact that females are more prone to stress and anxiety related disorders and thus explaining their higher problematic use, it could also highlight the fact that Smart phone addictions might be looked upon as more socially acceptable ways of gratifying oneself in a largely patriarchal society. The same social acceptibilty can be the reason for the higher number of Problematic Smart Phone Use seen in Muslim population because of strict religious restrictions on alcohol and nicotine. Further studies on this new behavioural addiction are the need of the hour as this might represent a growing plethora of new age addictions and psychiatry needs to address this problem in a more pro-active way in terms of new additions in classification of current substance dependence disorders.