-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Clinical Psychiatry
p-ISSN: 2332-8355 e-ISSN: 2332-8371
2018; 6(2): 34-39
doi:10.5923/j.ijcp.20180602.02

Comparison between Carbamazepine and Divalproate on the Improvement of Clinical Symptoms of Bipolar Mania with Psychotic Feature
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSonny Teddy Lisal1, Saidah Syamsuddin1, Veronika Suwono2
1Department of Psychiatry, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia
2Postgraduate, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia
Correspondence to: Veronika Suwono, Postgraduate, Faculty of Medicine, Hasanuddin University, Makassar, Indonesia.
| Email: |  |
Copyright © 2018 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Mania with agitation and psychotic feature can be improving with antipsychotic (haloperidol) combined with mood stabilizer (carbamazepin, divalproat). This study aimed to compare the effectiveness between haloperidol carbamazepine and haloperidol divalproate on the improvement of the clinical symptoms of bipolar mania disorder with psychotic feature. The research was conducted in teaching hospital and its network as an observational analytic study with prospective cohort design. The samples were fifty patients having bipolar affective disorder of current episode manic with psychotic feature. They had therapies using haloperidol carbamazepine and haloperidol divalproate for eight weeks. The statistical analysis which was carried out on the research data revealed the score decrease of Young Mania Rating Scale after the treatment with the haloperidol carbamazepine and haloperidol divalproate therapy from the 1st week to 8th week. There is no significant difference between haloperidol carbamazepine and haloperidol divalproate in improving the clinical symptoms of bipolar mania with psychotic feature. But haloperidol divalproate tend better than haloperidol carbamazepine in improving the remission symptom of bipolar mania with psychotic feature from the 3rd week to 6th week.
Keywords: Carbamazepine, Divalproate, Young Mania Rating Scale
Cite this paper: Sonny Teddy Lisal, Saidah Syamsuddin, Veronika Suwono, Comparison between Carbamazepine and Divalproate on the Improvement of Clinical Symptoms of Bipolar Mania with Psychotic Feature, International Journal of Clinical Psychiatry, Vol. 6 No. 2, 2018, pp. 34-39. doi: 10.5923/j.ijcp.20180602.02.
Article Outline
1. Introduction
- Bipolar affective disorder is a chronic mental illness characterized by mood swings, disability, and impaired quality of life. Bipolar affective disorder is a recurrent illness experienced throughout life with high rates of inpatient, suicide and comorbidity [1]. It is the sixth highest cause of disability in the world, causing more disadvantages and disabilities than cancer or neurological diseases such as epilepsy and Alzheimer's disease [2].Bipolar disorder is a severe disease with a high prevalence, with episodes of mania or depression and a symptom-free period. Although untreated episodes of mania last between 2 to 8 months, undesirable events can affect a patient's life and thus require effective and immediate treatment.Bipolar disorder is likely to have a genetic origin, seen in familial co-aggregation of bipolar disorder. Women are more often cyclical and mixed-type and have different comorbid patterns than men [3].Bipolar treatment includes a complex treatment because the disease has several phases, various symptoms and the mood stabilizer can only work on a particular spectrum. Research has shown that patient with bipolar episode mania who treated with mood stabilizer combination antipsychotic give better results compared with a single treatment of mood stabilizer.The last few years, treatment of bipolar disorder have changed with the use of divalproate, carbamazepine (CBZ), lamotrigine (LTG) and other anticonvulsants that can replace lithium. This is because lithium has a narrow window therapy, which means that the difference between the dose of therapy and toxic doses is very small. Typical antipsychotics are still used in the treatment of acute mania, but research on the effects of prophylaxis is lacking. Mania accompanied by agitation and psychotic symptoms can be treated as such as acute psychotic with antipsychotic drugs, such as haloperidol often used in conjunction with benzodiazepines, lithium and mood stabilizers. The neuroleptic dose is equivalent to haloperidol 8 to 10 mg / day. Higher doses increase the risk of side effects without showing any clinical improvement [4].Empirical research has shown that the most commonly used mood stabilizers are lithium, valproate and carbamazepine. The most common atypical antipsychotic is clozapine. The most commonly used antipsychotic is haloperidol.A study comparing three weeks of treatment between divalproate and placebo gave divalproate results more effectively than placebo and the antimania effect of divalproat appeared on the fourth day of treatment. While carbamazepine takes time to respond between 1 to 2 weeks.Previous research by Rajasuriya et al (2010), found no difference between divalproate and carbamazepine in the treatment of bipolar affective disorder.Health financing in Indonesia today is largely based on capitation systems. So the effectiveness of drug and the costs taking into clinician’s consideration. Carbamazepine is much cheaper than divalproat. However, many clinicians are cautious in administering Carbamazepine because of the life-threatening side effects of Steven Johnson's syndrome. To the author's knowledge, this research is still lacking in Indonesia and has never been done in Makassar.Based on this, this study was aimed to compare the effectiveness of therapy between haloperidol carbamazepine and haloperidol divalproate to improve clinical symptoms of affective disorder bipolar episode present mania with psychotic symptoms.
2. Methods
2.1. Subjects
- The population of this study were affective bipolar episodes of current episodes of mania with psychotic symptoms, who had been diagnosed according to ICD-10 and underwent outpatient or inpatient at UNHAS Education Hospital and its network. The samples in this study were all patients with bipolar affective affective episodes now mania with psychotic symptoms that have been diagnosed according to ICD-10 who underwent outpatient and inpatient at UNHAS Education Hospital and its network that fulfilled inclusion and exclusion criteria.Inclusion criterias are: [1] men and women 18 - 45 years of age, [2] diagnosis of axis I meets criteria of affective affective bipolar episode current mania with psychotic symptoms according to ICD-10, [3] patients affective bipolar disorder episodes mania with psychotic symptoms, early or recurrent episodes that have acute exacerbations, [4] willing to follow the research.Exclusion criterias are: [1] the patient is pregnant, [2] mental disorders due to substance abuse, [3] suffering from mental disorders due to organic disease (epilepsy, severe head injury, brain tumor and other neurological diseases), [4] the presence of severe physical disease that accompanies.All subjects were given informed consent following a description of the procedure, and all subjects were given opportunity to ask questions about the study.
2.2. Design and Procedure
- This study was an observational analytic study using cohort prospective design. The study was approved by the Ethics Commitee of Faculty Medicine, Hasanuddin University. Subjects were divided into 2 groups, the group receiving haloperidol plus carbamazepine (group 1), the group receiving haloperidol plus divalproat (group 2). The investigators measured the Young Mania Rating Scale between two group before treatment until 8th week after treatment.
2.3. Measurement
2.3.1. Psychometric Measures
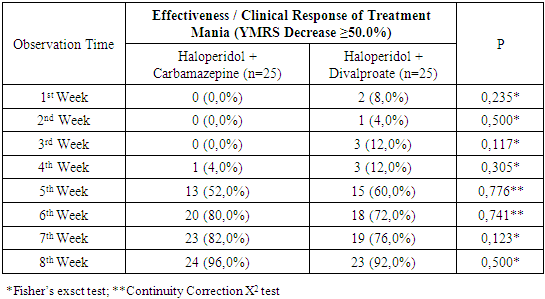
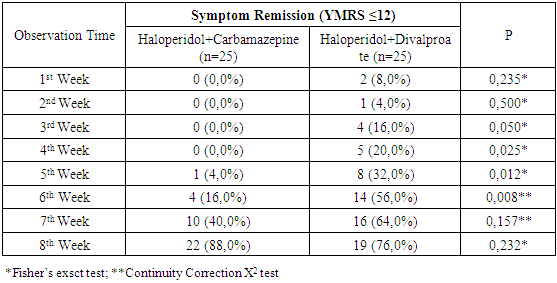
- Psychiatric symptomatology was evaluated using Young Mania Rating Scale. The scale consists of 11 questions and is based on the patient's subjective report on his clinical condition within the last 48 hours. Additional information based on clinical observation during a clinical interview. Consisting of four questions on a scale of 0 to 8 (irritability, verbalization, thought content and aggressive behavior, and seven 0 to 4 scale questions (mood elevation, increased motor activity, sexual interest, sleep, impaired thinking, appearance and insight) the question is more on objective appraisal as compensation for uncooperative patients. This scale may be performed by a clinician or someone who has been trained and takes 15 to 30 minutes to complete. Greater Young Mania Rating Scale (YMRS) score, the more severe the symptoms mania. Improved symptoms of mania / benefit in the treatment of acute mania, is a decline in Young Mania Rating Scale (YMRS) score ≥ 50%. Patients who achieved symptomatic remission defined patients who scored Young Mania Rating Scale ≤ 12 [5].
2.3.2. Statistical Analysis
- The data was analyzed using statistical program (SPSS) and presented as tables and graphs.
3. Result
3.1. Sample Characteristic
3.2. Comparison of Young Mania Rating Scale (YMRS) between the Two Treatment Groups
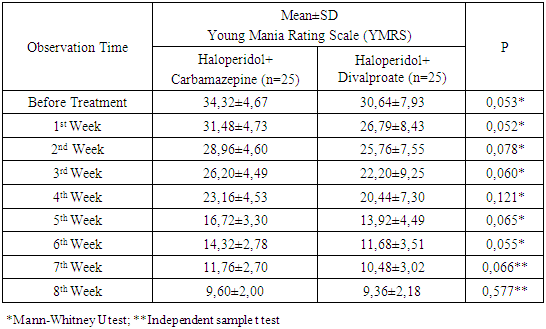
- Young Mania Rating Scale score between Haloperidol Carbamazepine group and Haloperidol Divalproat group did not differ significantly before treatment to 8 th week after treatment.Young Mania Rating Scale score in group haloperidol and carbamazepine group is more stable compared to group haloperidol and divalproate. Although from statistical analysis there was no significant difference. It appears that the starting point of the mean YMRS group Haloperidol Carbamazepine differs from the Haloperidol Divalproate group, but by 8 th week the two groups met at the same point.
|
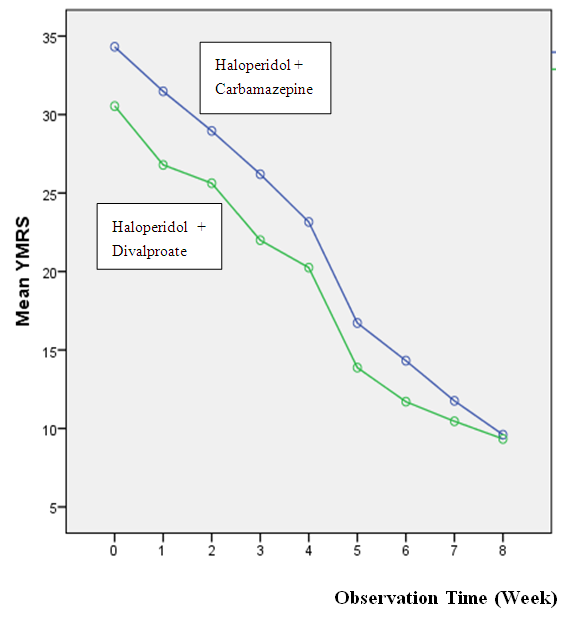 | Graphic 1. Comparison of Young Mania Rating Scale (YMRS) Between the Two Treatment Groups |
|
|
|
4. Discussion
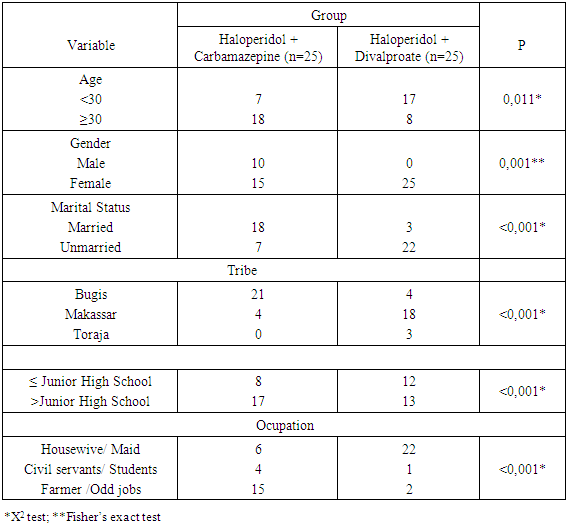
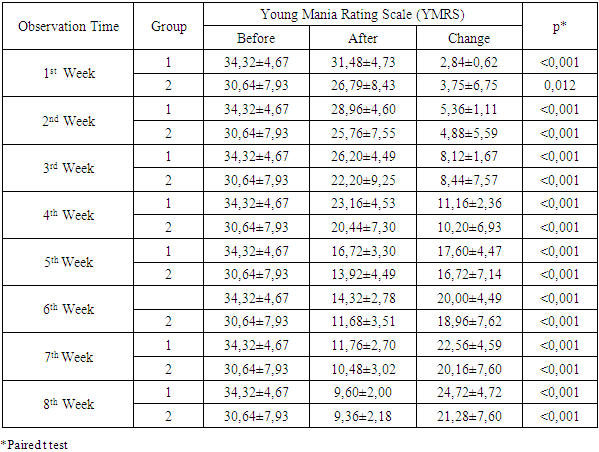
- In the group receiving haloperidol carbamazepine therapy, most of the samples (18 people) were ≥ 30 years old, whereas in the group treated with haloperidol divalproate, most of the samples (17 people) were <30 years old. Distribution of the number of samples by age characteristics is not homogeneous, as the tendency to treated young patients with divalproate due to carbamazepine may have side effects of Steven Johnson syndrome. While carbamazepine is given to patients who have previously been receiving carbamazepine therapy or inpatients multiple time. So much more is given Carbamazepine at age ≥ 30 years. Of the characteristics of sex is also not homogeneous. Where the sample with male sex is present only in haloperidol carbamazepine group. Overall, the number of male samples is only 10 people, while the female sample is 40 people. From etiology, bipolar I disorder has the same prevalence between men and women. In this study more female samples can be linked that men bipolar I disorder are treated with comorbid substance abuse. [6]The samples in this study were not diagnosed with rapid bipolar affective disorder, ie four or more episodes in one year.Table 2 comparing the Young Mania Rating Scale (YMRS) score between the two haloperidol carbamazepine groups with haloperidol divalproate showed no significant difference from before therapy until week 8 after therapy. Graph 1 depicting the declining score of Young Mania Rating Scale can be seen that the decrease of Young Mania Rating Scale score in group 1 is more stable compared to group 2. Although from statistical analysis there was no significant difference. It appears that the starting point of the mean YMRS group Haloperidol Carbamazepine differs from the Haloperidol Divalproate group. Where the initial value of the mean YMRS Haloperidol Carbamazepine is higher than Haloperidol Divalproate. This can happen because there is a tendency to give Haloperidol Carbamazepine to a more restless sample. On 8 th week both groups meet at the same Young Mania Rating Scale score point. This implies that the decline in the Young Mania Rating Scale group of Haloperidol Carmabamazepine tends to be more stable than the Haloperidol Divalproate group, although statistically the difference between the two groups was not significant. [7]In Table 3 showing a Young Mania Rating Scale (YMRS) change, there was a decrease in Young Mania Rating Scale score in each group receiving Haloperidol Carbamazepine therapy and in the group receiving Haloperidol Divalproat therapy from 1st week to 8 th week.Improved symptoms of meaningful mania / benefit in the treatment of acute mania, ie decreased Young Mania Rating Scale (YMRS) score ≥ 50%. Table 4 comparing the effectiveness / clinical response of treatment mania (YMRS decline ≥50.0%) was seen in the Haloperidol Carbamazepine group which achieved a 50% reduction in YMRS score only in the fourth week of 1 sample. While in the group Haloperidol Divalproat which reached 50% YMRS score reduction has been there from week 1 that is as much as 2 samples. This is consistent with studies from Ozcan and Boztepe which suggest that the antimania effect of divalproate appears from week I of treatment, whereas carbamazepine takes a longer time of 1-2 weeks. [8]Patients who achieved symptomatic remission were defined by patients with a Young Mania Rating Scale (YMRS) score ≤ 12. Table 5 comparing the symptomatic remission (YMRS ≤12 score) between the two groups showed a significant difference between the two groups from the 3rd to the third week 6th. That is, in the 3rd week there is no haloperidol carbamazepine group that achieves remission, while in haloperidol group divalproat there are 4 samples (16%). In the 4th week there was no haloperidol carbamazepine group that achieved remission, while in haloperidol group divalproat there were 5 samples (20%). In the 5th week of the haloperidol carbamazepin group there were 1 sample (4%) who achieved symptomatic remission while in haloperidol divalproat group there were 8 samples (32%) who achieved symptomatic remission. In the 6th week of the haloperidol carbamazepin group there were 4 samples (16%) who achieved symptomatic remission while in the haloperidol divalproat group there were 14 samples (56%) who achieved symptomatic remission. From statistical analysis, the difference in both groups in achieving significant symptomatic remission from 3 rd week to 6 th week.In this study there was no significant difference between Haloperidol Carbamazepine and Haloperidol Divalproate in improving clinical mania. However Haloperidol Divalproate tends to be better in achieving symptomatic remission than Haloperidol Carbamazepine.Divalproate can be said to be better than carbamazepine in achieving symptom remission because divalproate works in three ways: reducing the flow of this calcium ion by directly blocking the Voltage Sensitive Sodium Channels (VSSCs) and the second by inhibiting enzyme phosphorylation that regulates the sensitivity of sodium ion channels. Divalproate also regulates the flow of transduction signals that inhibit Glycogen Synthetase Kinase 3 (GSK3), Phosphokinase C (PKC) and Myristulated Alanine Rich C Kinase, thereby enhancing long-term neuroprotection and plasticity as an antimania / mood stabilizer. While Carbamazepine works only on the sodium and calcium channels. [9]Limitations of this study were the study was conducted observationally so characteristics of sample data (age, gender) and Young Mania Rating Scale starting point between the two groups non homogenous, the existence of confounding factors, the subjectivity in charging Young Mania Rating Scale.
5. Conclusions
- In the group receiving Haloperidol Carbamazepine therapy, there was a significant decrease in Young Mania Rating Scale score from before therapy until 8 th week after therapy. In the group receiving Haloperidol Divalproat therapy, there was a significant decrease in Young Mania Rating Scale score from before therapy until 8th week after therapy. There was no significant difference between Haloperidol Carbamazepine and Haloperidol Divalproate in improving clinical mania symptoms. Haloperidol Divalproate tends to be better in achieving symptomatic remission than Haloperidol Carbamazepine especially at 3 rd week to 6 th week.
ACKNOWLEDGEMENTS
- The authors declare that there is no conflict of interest regarding the publication of this paper. The authors would like to acknowledge the important support and contibutions of Ilhamjaya Patellongi, M.D (Phisiology; Research Methodology).