-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Clinical Psychiatry
2016; 4(2): 27-32
doi:10.5923/j.ijcp.20160402.01

Influence of Social Support, Stress and Coping Strategies on Depression among Children with Physical Disability in Nigeria
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLOkhakhume A. S., Aroniyiaso O. T., Olagundoye O. A.
Department of Psychology, University of Ibadan, Nigeria
Correspondence to: Aroniyiaso O. T., Department of Psychology, University of Ibadan, Nigeria.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This study examined the influence of social support, stress and coping strategies on depression among children with physical disability in Nigeria. The study adopted cross sectional research design, purposive sampling technique was used to select 120 children with physical disability and questionnaires were used for data collection. The result of the findings revealed that there was a significant influence of social support on depression {t(118)=4.55; p<.05} and further analysis indicated that participants with low social support experienced higher levels of depression (Mean = 69.73) while participants with high social support experienced lower levels of depression (Mean = 62.22). More so, the finding depicted independent significant influence of stress and coping strategies on depression {β = .68, t = 11.47; P < .05 & β = .289, t = 4.96; p < .05}. Also, the finding depicted joint significant influence of social support, stress and coping strategies on depression {F (3, 116) = 881.39; p < .05}. Therefore, the study concluded that social support, stress and coping strategies are predictors of depression among children with physical disability in Nigeria and recommended that government and non-governmental organisation should endeavour to implement an ecological-based support programme to support, educate and enlighten physically challenged children, their family members and society on how to help the disabled children deals with life situation.
Keywords: Social support, Stress, Coping strategies, Depression and Physical disability
Cite this paper: Okhakhume A. S., Aroniyiaso O. T., Olagundoye O. A., Influence of Social Support, Stress and Coping Strategies on Depression among Children with Physical Disability in Nigeria, International Journal of Clinical Psychiatry, Vol. 4 No. 2, 2016, pp. 27-32. doi: 10.5923/j.ijcp.20160402.01.
Article Outline
1. Introduction
- Loss of functional part of one’s body can cause grief, fears of changed life, and can result into depression, complete denial of enjoying some good things of life in some part of the world like Nigeria where disabilities were not inculcated into the development curriculum of the nation. Although, disability varies as some may be physical, cognitive, mental, sensory, emotional and developmental or some combination of these. It is an umbrella term, covering impairments, activity limitations, and participation restrictions. The loss of one part of the body may be congenital or acquired. It is widely accepted as a traumatic change in life circumstances that is likely to have long term consequences due to the loss and which may lead to psychological reactions such as depression. Depression is one of the most frequent psychiatric disorders in people with disability (Ban 1994). The point prevalence of depression among people with disability is estimated to be 4% (Cooper & Bailey, 2001; Cooper, Smiley, Morrison, Williamson, & Allan, 2007; Deb, Thomas, & Bright, 2001), and the period prevalence is thought to be notably higher (Cooper and Smiley 2003). People with disability, therefore, experience depression at greater rates than do their peers without disability. However, there has been little systematic research regarding the processes that contribute to the onset or persistence of depression among disability populace. However, these little studies found adverse effects of disability on depression to be relatively high. Disability is one of the main causes of depression, especially among children and it is important to know how physical impairments can be prevented and how one can help the child if he/she becomes disabled. meanwhile studies have shown that if physical disability is attended to early, much of its negative effects like depression and low self-esteem can be lessened through timely surgery, exercises and use of mechanical supports. The age at which the condition develops often determines its impact on the child (Cooper and Smiley 2003).More so, studies revealed that depression among children with disability decrease with greater social support. For example, Sarason et al. (Sarason, Levine, Basham, & Sarason, 1983) found that the greater the number of persons providing social support, the lower the depression scores in male and female respondents. Social support has also been associated with better mental health among the disabled people, with less depression in particular and greater active coping (Antonucci & Jackson, 1987). Socially supporting relationships act as a coping resource and help with an individual’s emotional adjustment (Gottleib 1983, Pearson 1986). Fundamentally, social support appears to facilitate the coping process by providing additional resources such as advice, information and material services that could increase an individual’s coping resources (Pearson, 1986). A lot of love, affection, patience and fortitude from friends and family will be needed, and they will have to be around to encourage and support the affected persons to help navigate them through these difficult times particularly in situation of significant risk, such as exposure to a traumatic life event (Masten & coatsworth 1998). Studies have shown that psychological outcomes of people with disability can hinge on social support from others and social support can come from various systems within a person’s frame of reference and it plays a vital role in buffering the effects of trauma and meditating stress.People with physical disability are exposing to very stressful situations. The problems encountered by people with disability differ from those faced by their peers without disability and which put them at risk of developing depressive symptoms. Physical disability is a common experience of everyday life; it often causes a person to use special equipment like wheelchair, cane or prosthetic limb. Persons with physical disabilities may have difficulty with movement or self-care, but are otherwise just like anyone else. It is important to note that disability prevents somebody from being able to do something that other people of his age and the community does because of the body deficiency. Disability restricts easy accessibility to the facilities within the environment and this constituted the major or real problem facing disabled people. It can lead to frustration in some cases, which adversely degenerate to an individual not being able to actualize his aspirations (Crisp, 2002). Many physically challenged people encounter problems in going about their activities of daily living because of the limitation that interferes with a person’s ability to walk or lift. It may be referred to as a condition that substantially limits one from more basic physical activities, such as walking, climbing stairs, reaching, lifting, or carrying. People differ not only in the life events they experience but also in their vulnerability to them. A person’s vulnerability to psychological stress is influenced by his or her temperament, coping skills and the available social support.Some studies have focused on various techniques and strategies that have been adopted by various classes of individuals in coping with all manner of life problems and disabilities (Babar et al., 2004). Depression among the disabled person is related to lack of active coping skills aimed at altering the stressful situation or negative emotions surrounding the situation and increased use of avoidant coping intended to avoid or ignore the stressful situation and negative affect surrounding it (e.g., Aldwin & Revenson, 1987). Coping strategies or skills help protect people from being psychologically harmed by challenging experiences in their lives (Pearlin & Schooler, 1978). Lazarus and Folkman (1984) divided coping skills into two processes: emotion focused coping and problem-focused coping. Emotion-focused coping is designed to regulate emotional responses to the problem, while problem focused coping is coping that is directed at managing or altering the problem that is causing the distress. Examples of emotion-focused coping responses are avoidance, distancing, and selective attention. Problem focused coping employs techniques such as defining the problem, generating alternative solutions, weighing the alternatives, choosing a solution and acting. Several studies have found that persons with disability using problem-focused coping strategies (e.g., active coping, cognitive restructuring, positive reappraisal, seeking instrumental social support and threat minimization) have better acceptance and adaptation to their illnesses than those who use emotional-focused coping strategies (e.g., expressing emotion, blaming oneself, avoidant coping, cognitive and behavioral escape, behavioral disengagement or distancing). More than a decade ago, Mc-Daniel (1976) reported a lengthy list of references dealing with all types of physical disability that implicated depression as a highly significant response. There has been a tremendous interest on the risk of depressive symptoms among children with physical disability and how well they transit into adulthood. This issue is crucial to psychologists because as individuals grow older, the deprivation caused by physical barriers such as inaccessible entrances to buildings, barriers to education, employment opportunities and negative public attitudes can result in secondary social, emotional, and psychological disabilities that persist into adulthood (Penland et als, 2000). These secondary disabilities can include depression, isolation, poor self-esteem, poor social adjustment, low self worth, rejection and unemployment (Blum, Resnick, 1991). They may also experience trouble in the areas of daily living skills, independent living and participating in the community. In Nigeria, there are few studies on disability and less consideration on some variables that have influence on depression among people with physical disability. Therefore, this study examine the influence of social support, stress and coping strategies on depression among children with physical disability. This study utilizes psychological principles in investigating influence of social support, stress, coping strategies on depression among the physically challenged children and the findings will give support to the development, designing of programmes and seminars with the objectives of helping people with disabilities to manage and cope with daily and future challenges.Purpose of the StudyThe main purpose of the study is to examine the influence of social support, stress and coping strategies on depression among children with physical disability in Nigeria. While the specific objectives include:i. To examine the influence of social support on depression among children with physical disability in Nigeria.ii. To determine the independent and joint influence of social support, stress and coping strategies on depression among children with physical disability in Nigeria.iii. Proffering credible and actionable recommendations to identified problemsHypotheses1. Children with high social support will report significant low level of depression compare to those with low social support.2. There will be significant independent and joint influence of social support, stress and coping strategies on depression.
2. Methodology
2.1. Research Design
- The study design method was cross sectional research design. The independent variables of the study include social support, stress and coping strategies, while dependent variable is depression.
2.2. Research Setting
- This research was conducted among children with physical disability in Ondo State School of the physically challenged Ikare Akoko located in Ondo State, Ekiti State special school for the disabled children, Ido-Ekiti located in Ekiti state, Oluyole Chesire School in Ibadan located in Oyo state and the rehabilitation center for the disabled, Moniya Ibadan, Oyo state. All the states were situated in Nigeria.
2.3. Study Population
- The general population of interest in this study was children with disability in Nigeria. children with disability, who are between the age range of 8 and 20 years were the focus of the researcher. One hundred and twenty participants (94 males and 26 females) participated in the study. Participants had a mean age of 9.2 years, the frequency distribution of participants varies as educational qualification showed that 101 had primary school certificate, 15 had SSCE and 4 had OND/NCE. Also, 94 of the total respondent were Yoruba, while 11 of them were Hausa, 13 were Igbo and 2 from other ethnic groups. However it was discovered that 52 of the total participants were Christians, 62 were Muslims and the remaining 6 practice traditional African religion.
2.4. Instruments
- Questionnaires were used to collect relevant information from the participants of the study. The questionnaire was divided into five segments with each of the segments tapping information based on the identified variables of interest. It comprised of five sections; A, B, C, D and E. The structure of the questionnaire is outlined below.Section A: Demographic characteristics In this section of the questionnaire, demographic information of the participants were captured ranging from age to their highest level of education. This section consisted of variables such as age, sex, religion and educational background.Section B: Social Support Scale for the Special Need Children The Social Support Scale for the Special need children was developed by Okhakhume (2008). It was 12-items constructed on 4-point Likert scale format, ranging from Highly use (4) to Highly use (4) and was design to tapped information on Social Support among Special need children. The resultant 12 - items scale yielded alpha coefficient of .61.Section C: Special Need Children Stress Scale IndexThe Special need children stress scale index was developed by Okhakhume (2008). It was 24-items constructed on 4-point Likert scale format, ranging from Not difficult (1), Little difficult (2), Moderately difficult (3), Maximum difficult (4) and was design to measure the level of stress experienced among Special need children. The resultant 24 - items scale yielded alpha coefficient of .81.Section D: Coping Strategies ScaleA modified version of Folkman and Lazarus (1985) scale, reversed by Folkman (1988) was use to measure coping strategies. it was originally a 50-items with 5-point rating scale but compressed into 34-items with 4-point rating scale for the purpose of this study with values: Does not apply (1), Used somewhat (2), Used quite a bit (3), and Used a great deal (4). The 34-items were divided into eight sub-scales with the sub-scale measuring different behavioural or cognitive activity: Scale 1 (item 1-4 designed to tap information on cognitive coping), Scale 2 (item 5-9 designed to tap information on distance coping), Scale 3 (item 10-14 designed to tap information on self control coping), Scale 4 (item 15-19 designed to tap information on social support coping), Scale 5 (item 20-22 designed to tap information on accepting responsibility coping), Scale 6 (item 23-25 designed to tap information on wishful thinking coping), Scale 7 (item 26-30 designed to tap information on problems-solving coping), Scale 7 (item 31-34 designed to tap information on positive appraisal coping). Scales 1 and 7 are problem-focused coping while the other sub-scales are considered emotion-focused coping. In this study, 15-items were retained after being subjected to items total correlation. The cronbach coefficient alpha of the 15-items was r=0.50, Guttman split-half reliability coefficient yielded .66.Section E: Children Depression ScaleThe Children Depression Scale was developed by Tisher and Lang (1978) and was reviewed using the Australian children in 1983. The instrument consisted of 66 items of which 48 are depressive items and 18 are positive items. The 48 depressive items are spread over 6 sub-scales (affective response, social problems, self-esteem, preoccupation with sickness and death, and miscellaneous D). The remaining 18 positive items are spread over 2 sub-scales (pleasure and enjoyment, and miscellaneous positive). All together, the instrument consists of 8 sub-scales, each items is scored on a range of 1-5 with 1 being very wrong, 2 being wrong, 3 being know, 4 being right and 5 being very right. The authors reported cronbach alpha of 0.96 which indicated high internal consistency among the items.in this present study, the short version of the original scale consisting of 28 items was used, which yielded alpha coefficient of .55, a split-half reliability coefficient using spearmen brown formula yielded .71 and Guttman split-half reliability was established 0.71.
2.5. Procedure for Data Collection
- Permission was first sought from all the head of the schools through inform consent letter from the department of psychology, university of Ibadan before the administration of the questionnaires. The researcher then administered the questionnaire, retrieved and one hundred and twenty were accurately satisfied. Prior to the given questionnaire to fill, the researcher instructed them on how they were expected to respond to the statement in the questionnaire and also informed them that their confidentiality was guaranteed and therefore they should not write their names on the questionnaire.
3. Results
- Research hypothesis one predicted that Children with high social support will report significant low level of depression compare to those with low social support was tested using independent sample t-test and the result is presented in Table 1 below;
|
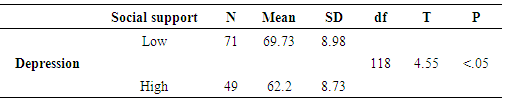
 = 69.73) while participants with high social support experienced lower levels of depression (
= 69.73) while participants with high social support experienced lower levels of depression ( = 62.22) and the result also indicated that the difference was statically significant.Hypothesis two predicted the independent and joint influence of social support, stress and coping strategies on depression. This hypothesis was analyzed using multiple regression analysis and the result revealed that stress, social support and coping strategies yielded a coefficient of multiple correlations (R) of 0.979 and multiple correlation square of 0.958. This shows that about 95.8% of the total variance of depression was accounted for by the linear combination of the three independent variables (stress, social support and coping strategies). This table also indicated that the two independent variables had significant joint influence on job satisfaction [F = (3, 116) = 881.39; P < .05].
= 62.22) and the result also indicated that the difference was statically significant.Hypothesis two predicted the independent and joint influence of social support, stress and coping strategies on depression. This hypothesis was analyzed using multiple regression analysis and the result revealed that stress, social support and coping strategies yielded a coefficient of multiple correlations (R) of 0.979 and multiple correlation square of 0.958. This shows that about 95.8% of the total variance of depression was accounted for by the linear combination of the three independent variables (stress, social support and coping strategies). This table also indicated that the two independent variables had significant joint influence on job satisfaction [F = (3, 116) = 881.39; P < .05].
|

4. Discussion
- The purpose of this research is to understand the adjustment of physically challenged children over time and to examine the influence of social support, stress and coping strategies on children with physical disability on depression. The first hypothesis verified the difference between participants with high perceived social support and those with low perceived social support on depression. The result revealed that social support has significant influence on depression which indicates that participants with low social support experienced higher levels of depression while participants with high social support experienced lower levels of depression. The hypothesis was therefore confirmed and this finding is supported by Lehman et al, (1986) who found that social support plays a vital role in buffering the effects of trauma and mediating stress. This finding was also consistent with finding of Stroebe et al, (1996) who postulated that People with disability who perceived the social support system available to them as high reported less depressive and somatic symptomatology than those who reported low support. In the aftermath of a traumatic event, efforts to reduce stressfulness (e.g. by providing information, orientation, warmth and hope) have an essential role in reducing depression (Shalev 2000). it was observed that supportive behaviours are always result to positive outcome and studies have shown that social support has been found to have beneficial effects on both physical health and psychological well being of individuals coping with disability, and has specifically been found to minimize the effects of physical limitations resulting from disability on psychological adjustment and this support the finding of this study.The second hypothesis predicted the independent and joint significant influence of social support, stress and coping strategies on depression. The result revealed that social support, stress and coping strategies had a significant independent and joint influence on depression. The hypothesis is confirmed and this is consistent with the previous findings that stress and coping strategies are cognitive appraisal component of how to survive the challenges of life (Andersen & Williams, 1988; Folkman & Lazarus, 1991; Weiss & Troxel, 1986; Wiese- Bjornstal, Smith, Shaffer, & Morrey, 1998). The basic framework of these models is centred on the individual’s cognitive appraisal of his or her situation (i.e., physical disability). In essence, how an individual interprets or appraises the disability determines how the individual will react emotionally (e.g., anger, depression, and acceptance). As Brewer (1994) states, “the fact that the disability has occurred is considered less critical to understanding emotional reactions than the way in which the disability is perceived” Once a disability occurs, the individual begins the process of cognitive appraisal, which Lazarus and Folkman (1984) have broken down into two processes: (a) primary appraisal, and (b) secondary appraisal. Each of these processes can be summarized by key questions asked by the individual. For the primary appraisal, the individual asks, “Is this harmful to me?” Once this initial assessment is made, the secondary appraisal begins with the question “Will I be able to cope with this situation, and, if so, how?”. Emotional and behavioral responses (i.e. coping skills) to the disability are then generated as a result of the individual’s appraisal of the situation. Coping skills help protect people from being psychologically harmed by challenging experiences in their lives (Pearlin & Schooler, 1978) and this was consistent with the finding of this study.
5. Recommendations & Limitations
- Based on the findings of this study, the following recommendations are made:It is imperative for the professionals and community members associated with children with physically disability to be more diligent in responding to the emotional needs of individual experiencing physical disability as the result of this study revealed that social support had significant influence on depression among children with physically disability. It is recommend that government and non-governmental organisation should endeavour to implement an ecological-based support programme in order to support, educate and enlighten physically challenged children, their family members and society on how to help the disabled children deals with life situation.This research is limited to social support, stress, coping strategies, depression and 120 children with physical disability in three states in a country, other factors and large sample such also be considered for further research. Also, there is need to carry out longitudinal studies as most of the research carried out in this area has been cross-sectional.