-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Clinical Psychiatry
2016; 4(1): 17-25
doi:10.5923/j.ijcp.20160401.03

Feasibility Study Using In-Water EEG Measurement during Dolphin Assisted Therapy
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLBernd Johannes 1, Peter Bernius 2, Juergen Lindemann 3, Olaf Kraus de Camargo 4, Rolf Oerter 5
1Institute of Aerospace Medicine, German Aerospace Center (DLR), Cologne, Germany
2Center of Children Neuro-Orthopedics, Schön Clinic München Harlaching, Germany
3Dolphin Aid
4Developmental Paediatrics, McMaster University, Hamilton, Canada
5LMU München, Psychology and Pedagogics; Munich, Germany
Correspondence to: Bernd Johannes , Institute of Aerospace Medicine, German Aerospace Center (DLR), Cologne, Germany.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Dolphin aided therapy (DAT) is still lacking convincing scientific verification. To assess neurophysiologic changes in the brain during therapy sessions a novel methodological approach was developed and tested. It consists of a reliable and good quality registry of electroencephalogram (EEG) during in-water interactions between patients (children) and the dolphin. In a feasibility study we could demonstrate that this was technically possible. The procedure did not interfere significantly with the therapeutic process. Children and parents tolerated the procedure well. The registered EEG could be used for clinical analyses and represents an addition to existing assessments to describe therapy effects on brain activity during the therapy sessions in the water. Further studies are recommended to determine ideal test protocols and include a greater number of subjects.
Keywords: Dolphin aided therapy, Electroencephalogram
Cite this paper: Bernd Johannes , Peter Bernius , Juergen Lindemann , Olaf Kraus de Camargo , Rolf Oerter , Feasibility Study Using In-Water EEG Measurement during Dolphin Assisted Therapy, International Journal of Clinical Psychiatry, Vol. 4 No. 1, 2016, pp. 17-25. doi: 10.5923/j.ijcp.20160401.03.
Article Outline
1. Introduction
- Dolphin therapy or dolphin assisted therapy (in the following always labeled as DAT) has received critical discussion. A range of studies reports that dolphin therapy is successful (Smith 1987; Nathanson & de Faria 1993; Nathanson, de Castro, Friend & McMahon 1997; Nathanson 1998; Lindeblad 1996; Donio 2003; Humphries 2003; Dilts 2008; Likura et al. 2001; Lukina 1999; Antoniolo & Revelely 2005; Dilts, Trompitsch & Bergquist 2011). Other studies focus on specific aspects of dolphin therapy such as changes in interaction and communication of patients and their parents (Breitenbach, v. Fersen, Stumpf & Ebert 2006, 2009) or interaction between dolphin and patient (Poizat 2003). Dolphin therapy is also viewed as a special form of animal assisted therapy (Kruger & Serpell 2006; Prothmann 2006; Serpell, Coppinger, Fine & Peralta 2010). Skeptical and negative evaluation of DAT is presented by Scheer (2005) and Marino & Lilienfeld (2007). Humphries’ (2003) critical assessment of six studies points out the necessity to conduct further studies in order to prove the effectiveness of dolphin therapy. Kohn and Oerter (2004) summarized four central questions to be answered for a verification of DAT effects. They provide a scientific analysis of psychological data supporting the positive effect of DAT in two of the first DAT centers in the world. There are actually three studies run that provide evidence which is methodologically better founded than earlier studies. The first was conducted by Nicole Kohn (2004). 220 young handicapped patients underwent a dolphin assisted therapy in Eilat, Israel, and Key Largo, Florida, U.S.A. In a pre-post-follow-up design they verified efficiency of the treatment using a questionnaire. In a second study Nicole Lämmerman (2013) measured in a pre-post design non-verbal intelligence, attention/concentration and motor skills with objective tests and found an increase of scores in all domains, while control groups - one of them received another treatment – showed no significant change. Since intelligence scores normally do not change within a few weeks and other improvements of test achievements can also not be expected in such a short time, the best interpretation of results is probably that dolphin therapy acts as an icebreaker or door opener enabling existing potential. Patients seem to be blocked or unable to produce their optimal level of achievement, and DAT helps them to become open for interest in environment, social contact and general attention to reach their optimal level of achievement. This assumption is supported by a third study in which Stenczel (2013) analyzed video-taped scenes of dolphin-child interaction. She found among others an increase of patients’ initiative with their reactions toward the dolphin, while the dolphin adapted its behavior to the changing behavior of the patient reducing its own initiative. Patients also showed increasing positive emotions during the therapy. On the whole, the study of dolphin-patient interactions demonstrated a dramatic change of patients’ behaviors toward a more active, attentive, social and emotionally positive conduct. Stenczel formulated a hypothesis about a dual attention required of the child and provoking an improvement of cognitive information processing: attention towards the dolphin as a multisensory stimulus and attention towards the dolphin as a social stimulus.Children receiving DAT are mostly non-verbal and difficult to be assessed in traditional ways. The observations made above should have a neurophysiological correlate. It therefore seemed reasonable to use EEG methodology during therapy sessions. If the hypothesized changes in attention processes during therapy could be confirmed by EEG it could be an indicator of possible therapy mechanisms and effects.Although the knowledge of the relation between changes in EEG activity and behavioral or health consequences is only emerging, it seemed to us a good starting point to gather more information about what happens during DAT. There was only one study presented at a conference using electroencephalogram (EEG) as an objective physiological measure (Cole 1996). Cole found changes in the intensity of frequency ranges between pre- and post-measures of therapy sessions with direct dolphin contact. He interpreted them to be similar to changes observed during anesthesia responses. Replicating this study would add to our understanding, but having EEG-readings obtained during therapy sessions in the water could provide new insights into the interaction effects between kids and dolphins. The main effects of EEG-change might occur during therapy sessions in the water.Changes in EEG activity related to physical activity and mood have been reported before (Mierau, Schneider, Abel, Askew, Werner & Strüder 2009, Schneider, Askew, Diehl, Mierau, Kleinert, Abel, Carnahan & Strüder 2009, Woo, Kim, Kim Petruzzello & Hatfield 2009, Brümmer, Schneider, Abel, Vogt & Strüder2011) and could also be occurring in children participating in DAT. Continuous EEG-monitoring in children being investigated for epilepsy is available for several years now, but it has been used mainly to identify interictal discharges (Curless, Ramsay, Katz, Gadia & Sheehan 1990). We are not aware of the availability of a technology and studies done to monitor EEG-activity in children moving in the water.To our knowledge it was impossible until our days to register EEG for clinical purposes during in-water treatment. Therefore, it was the primary goal of this methodological feasibility study to test, whether it is practically possible to register EEG reliably and with clinical relevant quality during the in-water therapy sessions. The secondary goal was to verify, whether the EEG-measurement was tolerable and accepted by the children and their parents. In addition, it was important to ensure for future studies regarding DAT that the registration procedure does not disturb the therapy process.
2. Methods
- Dolphin Aid Therapy at Curacao Dolphin Therapy and Research CenterThe non-for profit organization "dolphin aid" supports and assists mostly patients from Germany to facilitate their participation in dolphin assisted therapy. The foundation is a registered charity and is advised by medical, parental, legal, scientific and veterinary boards. One of the goals of the foundation is to establish conceptual guidelines for DAT and promote the scientific research of this therapy option. Our project is in accordance with these goals. The mainstay of DAT is the interaction between patient and dolphin. This interaction is supported by the therapist and the dolphin's trainer. The therapy concept of dolphin aid consists of four components: patient-therapist interaction, dolphin-patient interaction, the dolphin as supporter and the therapeutic goals (guidelines for dolphin therapy, dolphin aid e.V. Düsseldorf).
2.1. Subjects
- Four girls and one boy, in the age from 4 to 15 years and normal weight took part. Table 1 presents their different clinical diagnoses.
|
2.2. Measurements
- Two measurement systems were used. A standard clinical device THERA PRAX® Q-EEG (sponsored by neuroConn GmbH, Ilmenau, Germany) with a standard 10-20 cap was used for the clinical pre- and post-measurements (Berkes et al. 2002). Mobile polygraph equipment based on the HealthLab-system (Koralewski Ind. Elektronik oHG, Hambühren, Germany) was used for the in-water measurements. This measurement hardware had been used in several previous studies (although, outside the water but in demanding environments like inside the International Space Station). The equipment originally developed for uses under extreme environments (Johannes & Salnitski 2000; Ledderhos, Roth, Gens & Johannes 2008; Johannes, Salnitski, Soll, Rauch & Hoermann 2008) was specifically adapted to the in-water application.There were several technical verification tests run in pools in Germany with volunteer healthy children prior to the application in Curacao. The fully water-protected equipment has an external antenna which is fixed at the electrode cap and kept above the water surface for a telemetric transmission (BlueTooth®) of the data to a standard notebook. The data were monitored and stored online on the computer and in parallel in the mobile system itself. The monitor software (SpaceBit GmbH, Germany) allowed marking behavioral events by the investigator. The event list and marker list were developed in close cooperation with the therapists prior to the first measurement. This system allowed registering eight uni-polar EEG-channels and voice pitch (Johannes et al. 2007). As the throat microphone for the voice pitch registration was not accepted by all children it had to be excluded from the study. The EEG was sampled and stored with 256Hz. The channels Fp1, Fp2, F3, F4, C3, C4, P3 and P4 were recorded. For practical reasons the T6-electrode was used as common reference instead of the mastoid (A2). Two sizes (52-54cm; 55-57cm) of standard 20-10 EEG-caps (Electro-Cap International, Inc., Eaton, Ohio, USA) with Ag/AgCl-electrodes were used allowing the application of the hydro-gel (Electro-GelTM, Electro-Cap International, Inc., Ohio, USA) after positioning of the electrodes. For one child a smaller cap would have been needed for proper registration conditions.Corresponding to the physiological registration the whole sessions where video-taped with a digital SONY camcorder (S100E), fixed on a tripod and operated by a second investigator. Camcorder and measurement equipment were synchronized daily prior to the first session. The one-day desynchronization was about 500 ms and can be neglected.
2.3. Study Protocol
- On day 1 after arrival the EEG-measurement was successfully tested on the beach and in-water worn by the investigators themselves. Dolphin Aid provided us the possibility for self-experience with the dolphins.On day 2 the group of investigators observed the therapy process. They introduced the aim of the study to the parents, therapists and dolphin trainers. A preliminary event list was prepared, supported by the therapists. The equipment was presented and tested by a therapist in-water.From day 3 to day 6 the measurement sessions were run.
2.4. Procedure
- The children and their parents arrived 30 minutes prior to the usual session time. In an air-conditioned office a standard EEG equipment was attached to the children and EEG was registered for 5 minutes in supine position under calm conditions, including opening and closing eyes. Afterwards, the EEG-cap was taken off. This procedure was run by two well experienced medical-technical assistants of the Neurological Clinic Vogtareuth, Germany, used to register EEGs in children with disabilities during their daily routine. The parents of the child and the personal therapist were present and supported the kid. The therapy session started with a preparation phase in another room. The investigators prepared the mobile system and waited for the kid at the water side. It required additional 10 minutes to apply the mobile system to the child before the usual session protocol was continued. When arriving at the therapy platform, the video-taping was started. One investigator operated the notebook computer, entering event markers and verifying signal quality. The second investigator operated the camera, keeping the child in the focus. The therapy session consists of 4 phases: 1. a preparation phase on the platform2. a first in-water phase3. a mid-term mental work phase on the platform and 4. a second in-water phase. In case of signal quality loss, the third phase was used to add hydro-gel and to correct electrode positioning. Immediately after the last phase the mobile system was removed from the child.
2.5. Therapy Session Protocol
- A single in-water therapy session was clearly structured and could be divided into a certain amount of events. The order and the kind of events varied among the sessions. Single events, which repeatedly occurred during a DAT session could be marked in the data-recording by pressing a menu button.
2.6. Data Analysis
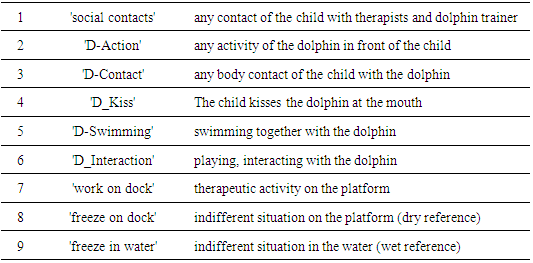
- In the whole there were twelve therapy sessions during which occasionally EEG-measurement could be carried out. For one child we could register only one session. A second child was available for two measurement sessions. For three kids we could successfully measure the EEG during three sessions. For intra-individual comparison the large amount of therapy events were combined into seven event classes plus two reference measures (“freeze”, see Table 2).
|
2.7. Visual Verification of the EEG
- The original registration software was not intended for a clinical evaluation of EEG-signals. The EEG-specialists were also not familiar with the software. To allow for a visual analysis of the EEG-signals those were copied in a format of 2 cm per second and 1 cm per mV into Word-files. In a second step, one of the assistants merged screen shots of the film for certain events with the respective time interval of EEG-registration (12 seconds). In a later step the visual verification was repeated by the software system INTERACT (MANGOLD GmbH, Germany), allowing synchronized visualization and frequency analysis in movies and physiological data.After the confirmation, that the registered data actually corresponded to EEG activity as opposed to movement artifacts, a frequency analysis of the EEG was run for each marked phase by the HealthLab software (Spacebit GmbH, Germany).The statistical analysis had to remain restricted to descriptive statistics. The low statistical power of the data set does not allow inference analyses. The statistical description was run with SPSS for Windows.
2.8. Relevance and Hypothesis
- If the main effect of DAT occurs during the sessions with the dolphin, the observed change in emotion and behavior (Stenczel, 2013) should also result in a change of EEG during the session. Therefore, the use of EEG-Measurement during the encounter between patient and dolphin seems to be crucial for proving positive effects of the dolphin himself. So, our hypothesis is that the interaction between dolphin and patient is accompanied by changes in the EEG that could mirror the observed psychological change by corresponding electro-physical data.
3. Results
- The basic investigation of EEG under rest conditions provided no differences between the pre and post session (figure 1). The findings do not suggest a shift of intensity from the beta-alpha range towards the theta range after the DAT session as found by Cole (1996).
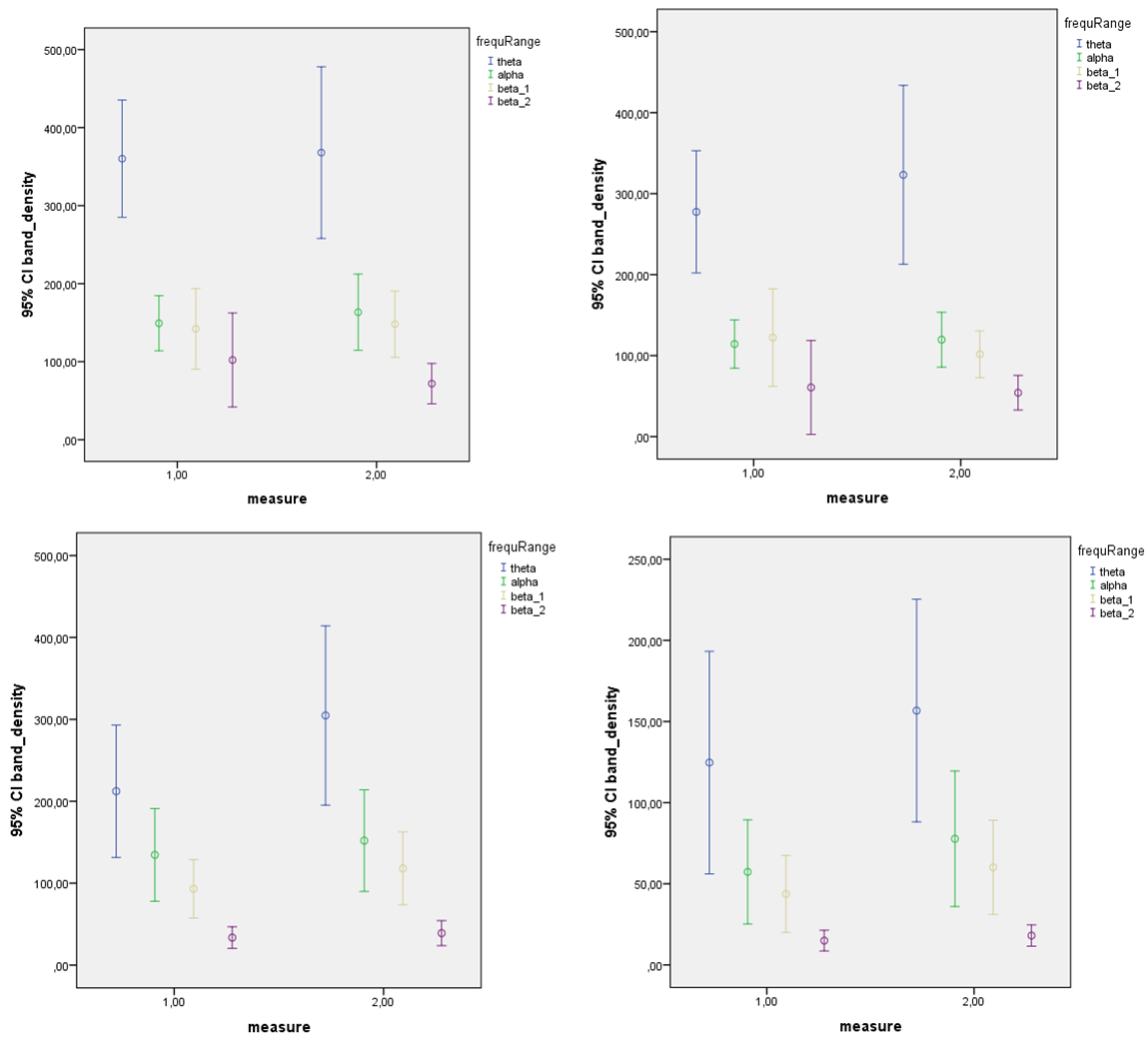 | Figure 1. Pre- post session comparison of theta, alpha, beta1 and beta2 densities for the electrodes F3, F4, P3 and P4 |
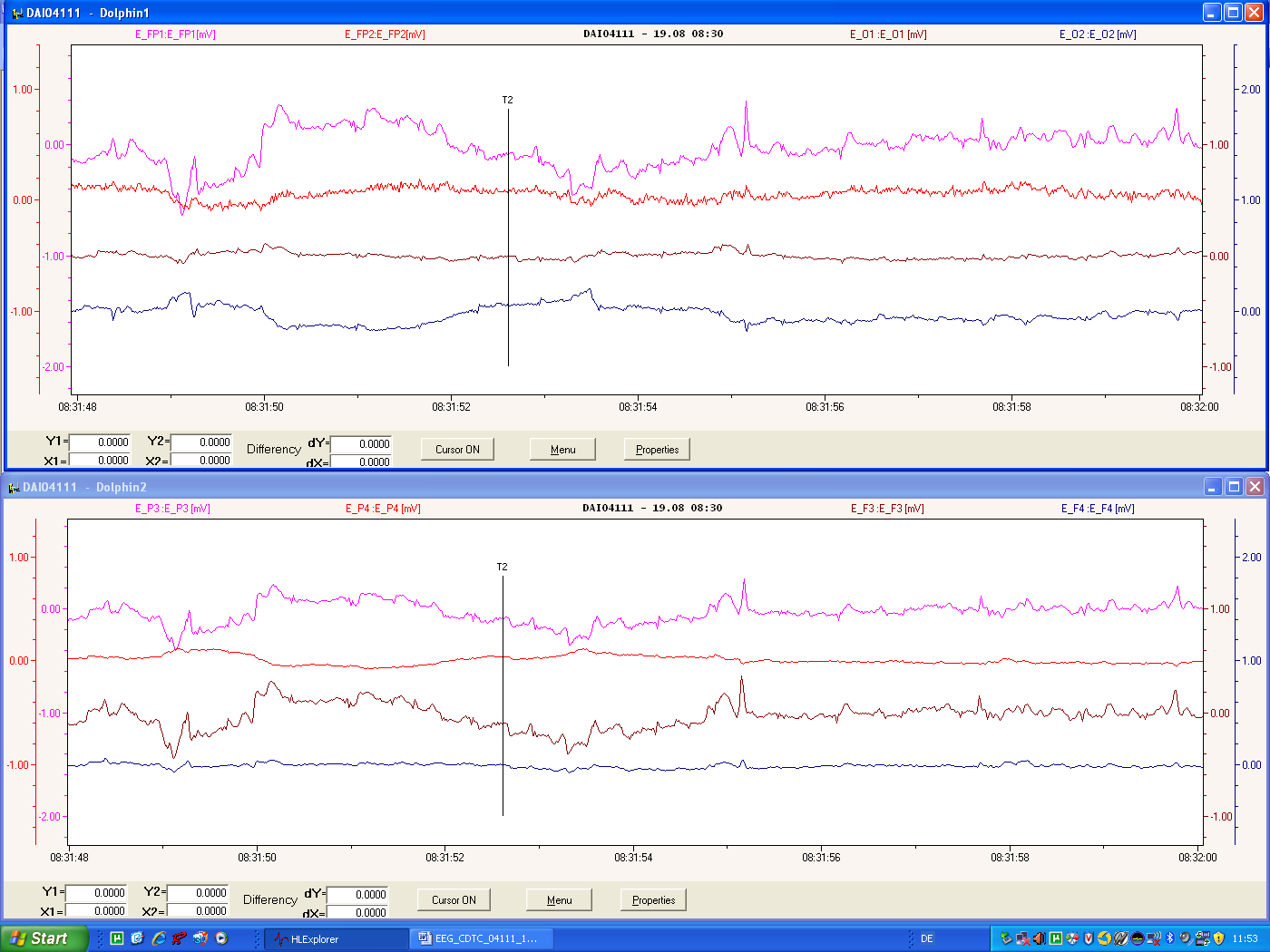 | Figure 2. Screen shot of the graphical visualization of EEG-data in a Word document. The T2-line represents a marker, set by the investigator |
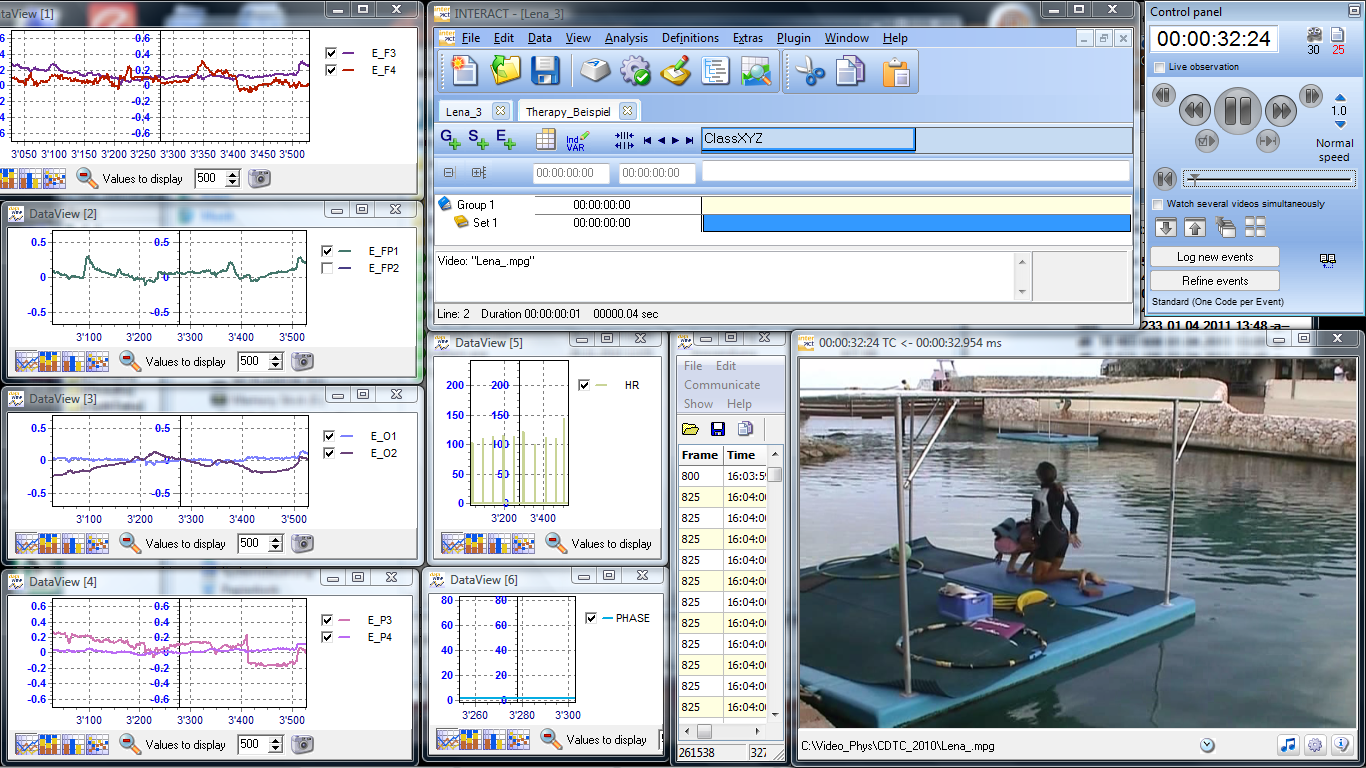 | Figure 3. Screen shot of synchronized video and physiological data |
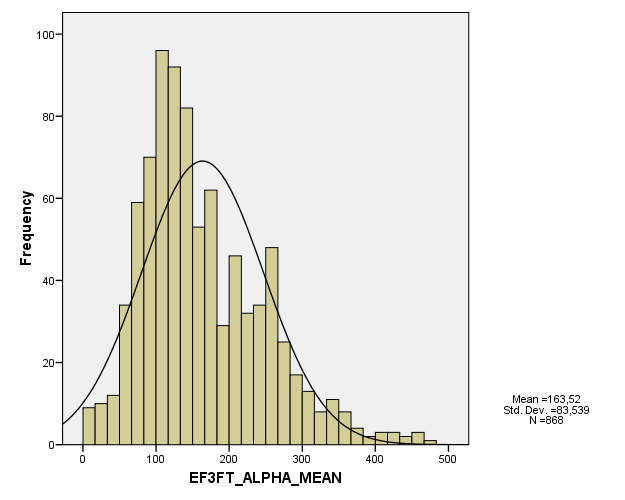 | Figure 4. Data distribution example of the alpha activity |
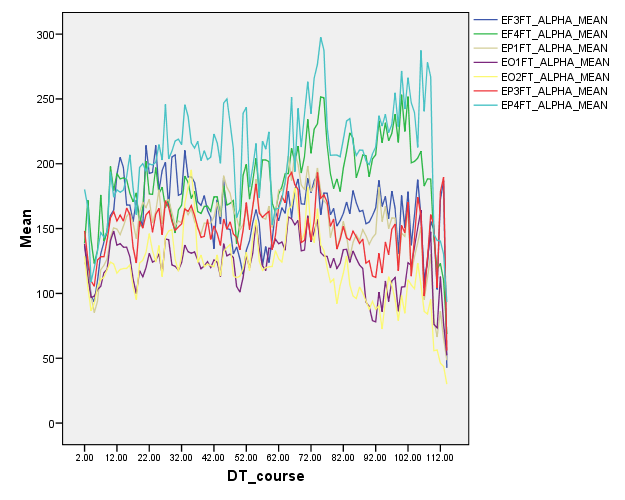 | Figure 5. Timelines of the alpha acitivity measures, pooled over all sessions |
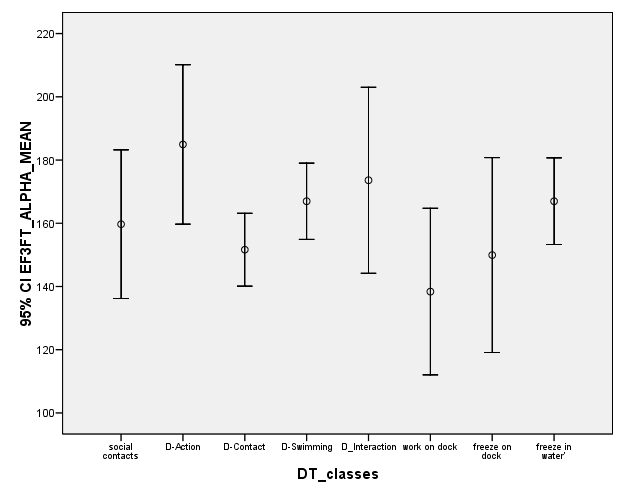 | Figure 6. Alpha activity during different dolphin behavior event classes |
4. Discussion
- The technology of choice to describe neurophysiologic phenomena in the brain is the EEG. We were able to demonstrate that it is feasible to obtain EEG data of acceptable quality from children in the water during DAT. We could estimate the occurrences, frequencies, and amplitudes of alpha and theta waves. This allows generally also the interpretation of their changes. Electroencephalographic potentials which are typical for epilepsy could be detected when they were generalized, e.g. as 3 per second sharp-wave-complexes in subclinical or clinical epileptic attack pattern (seizure pattern, not presented here). For a detection of focal epileptic paroxysms, a larger number of electrodes and a bipolar registration type would have been necessary.We could identify dolphin behavior related synchronous changes in alpha and theta waves and amplitudes. Whether these changes were mostly evoked by eye closing could not be excluded by the videotaping. The camera was at a fixed position and often the face of the child not visible. However, the preliminary spectral analysis of the EEG periods related to certain dolphin behaviors suggests systematic changes. Generally, the alpha band was extended when being in the water, indicating a general relaxation. But an impressive decrease of alpha activity occurred when children had an intense direct contact with the dolphins – kissing the dolphin or being kissed by the dolphin. That could indicate a focusing of attention towards the dolphin. Several limitations need to be identified for this study. It was only designed as a feasibility study. Statistically founded conclusions would require a larger number of data. The presented date only allow for the generation of research hypotheses. It remains also an open question whether the observed EEG-changes are specific effects of the dolphin therapy or could also be observed during other animal aided therapies even during classical therapy interventions. The small number of participants with different diagnoses was sufficient to demonstrate feasibility but would require a larger number and diagnostic subgroup analysis for further conclusions.Summarizing, we were able to demonstrate that it is possible to register EEG under salty water open sea conditions in children with disabilities. The collected data are of clinical value and provide the possibility for frequency analysis. The measurement does not impact the therapy process except for adding 15 minutes to the whole session. The children tolerated the measurement well and the parents supported the investigation and expressed their great hopes in understanding better, what processes are occurring during the session. To further understand the effects and mechanisms of dolphin assisted therapy it would be important to combine our approach and methodology with psychological observational methods as described in previous studies (Kohn & Oerter 2004).
ACKNOWLEDGEMENTS
- We have to thank our participating children and their parents for their interest and cooperation in the study. A great thank you goes to the therapists of CDTC who helped a lot with their skills and knowledge. Without the work of our assistants Silke Link and Hannelore Demel the huge amount of measurements could not have been managed within the few days. And last but not least, we thank the space agency German Aerospace Center, DLR, in person, Horst Binnenbruck, for supporting the present work as well as for providing the hardware.