Nicole Kohn, Rolf Oerter
Department of Psychology, University of Munich, Leopoldstraße 13, 80802, Munich
Correspondence to: Rolf Oerter, Department of Psychology, University of Munich, Leopoldstraße 13, 80802, Munich.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Abstract
Aim of the study was to examine whether dolphin assisted therapy has an effect at all and how a possible effect can be explained. 220 young handicapped patients underwent a dolphin assisted therapy in Eilat, Israel, and Key Largo, Florida, U.S.A. In a pre-post-follow-up design the efficiency of the treatment was tested by a questionnaire with a five-point Likert Scale that was administered to parents as well as teachers and therapists at home, respectively. Subjects were asked before the therapy, six weeks after the therapy and in Key Largo also six month later. Factor analysis of the items resulted in four factors: cognition, emotion, conspicuous behavior and motor skills. Internal consistency was satisfying (Cronbach’s alpha lies between .600 and .926). Correlations between the teacher’s/therapist’s judgements and parents’ ratings ranged from .411 to .533. Since the ratings of teachers and therapists at home can serve as a criterion of external validity, results can be assessed with regard to their validity. In all four domains parents as well as teachers/therapist perceived an improvement. This was also true after six month where the raters observed a further progress. Therefore, results suggest that dolphin assisted therapy had positive effects for children and adolescents under investigation. The therapy procedure differed remarkably in Eilat and Key Largo which support the assumption that the dolphin himself and not other additional conditions is the main condition for the outcome.
Keywords:
Dophin Therapy, Handicapped Childern, Reliability, Validity of Ratings
Cite this paper: Nicole Kohn, Rolf Oerter, Dolphin Assisted Therapy Works: Scientific Findings from Eilat and Florida, International Journal of Clinical Psychiatry, Vol. 1 No. 1, 2013, pp. 1-16. doi: 10.5923/j.ijcp.20130101.01.
1. Introduction
Dolphin therapy or dolphin assisted therapy (in the following always labeled as dolphin therapy) has received critical discussion. A range of studies report that dolphin therapy is successful (Nathanson,[1]; Dilts,[2]; Humphries, [3]; Likura et al.,[4]; Lukina,[5]; Kohn,[6]; Dilts, Trompitsch &Bergquist,[7]. Other studies focus on specific aspects of dolphin therapy such as changes in interaction and communication of patients and their parents (Breitenbach, v. Fersen, Stumpf & Ebert,[8]) or interaction between dolphin and patient (Poizat,[9], Stenczel,[10]; Beeck,[11]. Dolphin therapy is also viewed as a special case of animal assisted therapy (Kruger & Serpell,[12]; Prothmann,[13]; Serpell, Coppinger, Fine & Peralta,[14]. Skeptical and negative evaluation of dolphin therapy is presented by Scheer[15] and Marino & Lilienfeld[16]. Humphries’[3] critical assessment of six studies points out the necessity to conduct further studies in order to prove the effectiveness of dophin therapy. This paper reports empirical findings about dolphin assisted therapy in two different geographical locations. This investigation may provide preliminary answers to the four main hypotheses elaborated below.
1.1. First Question: Does the Dolphin really Play the Major Role?
The attempt to proof the effect of dolphin therapy is connected with several difficulties. One of the problems consists of the fact that there are many different dolphin therapy programs offered that differ in many ways. Furthermore, besides the contact with the dolphin there is a number of supporting measures, so that it must be clarified whether the actual experience of interacting with the dolphin is the one that has the healing and helping effect.Two quite different therapy forms were incorporated into this investigation and research, the Dolphin Human Therapy in Key Largo, Florida, and the Dolphin Reef in Eilat, Israel.Nathanson, director of the Dolphin Human Therapy, leads the effects back to the interaction of three components: Water – Dolphin - New environment. By means of water, relaxation, pain reduction and decrease of fears and depressions is reached.According to Nathanson’s opinion, the dolphin itself has an effect on the handicapped child due to its intelligent adjustment, its harmonious and aesthetic qualities and due to the relaxing, but at the same time also concen- tration-increasing characteristics.Nathanson builds however particularly on the positive reinforcement effect - a term from behavior therapy. This means that the dolphins are used as reward for desirable mental, physical or emotional reactions.On the contrary, the program of Dolphin Reef in Eilat, structured and conceived by Sophie Donio, provides the free interaction with the dolphin. Spontaneous experience, the special experience of touching, looking at and common swimming are regarded as crucial. This means that Donio pursues rather an emotional (experience-oriented) approach. The animals in the Reef behave quite differently than the trained animals in Key Largo. Their behavior is specific according to their species and is affected less by precise reactions taught to them by their trainers. They get near when they want to and approach humans only on own initiative.In contrast to this, the dolphins at the Key Largo facility carry out a sometimes artistic scenario with children and adults: They push them at their feet or pull them on the dorsal fin through the water and “shake hands” with them by offering their fins in upright position. Can one expect that two quite different therapy forms show a similar outcome? If this is the case, we may assume that the special experiences with the dolphin play a decisive role in the therapy. Therefore, the costs of such therapy would be justified because the dolphin would not be replaceable by other measures.Hypothesis 1: Dolphin therapy helps independently of any specific procedure and its basic therapeutic conceptions. This assumption is assisted by prior results mentioned above.
1.2. Second Question: For which Type of Impairments does Dolphin Therapy Actually Help?
As will be demonstrated, the treated group of children and adults exhibits different types of defects and impairments. Usually it is expected that there is a correspondence between the type of impairment and a specific treatment. A general positive effect independently of a specific handicap would throw a new light on dolphin assisted therapy insofar as its effect cannot be described as one single causal pathway. Results will show that there is indeed a comprehensive effect of the therapy.Hypothesis 2: The effect of dolphin therapy depends of the type of impairment.
1.3. Third Question: Can the Effect of Dolphin Assisted Therapy be Proven at All?
The most important effect is surely not to be expected in physical improvement, as for example with Cerebral palsy, but rather in the psychological realm, i.e. for mental and social skills, e.g. improvement of the attention and concentration span, of communication, of emotional experiences and of the behavior problems. The two most important ways of proving such effects probably are objective tests and the judgments of parents and therapists.The first possibility has been disregarded because children and young people affected live in different areas around the world, which makes it impossible to organize cost efficient visits before the scheduled therapy. Beside this organizational reason, there is also another limitation: the strong impairment of many children makes it very difficult to apply standardized tests that offer characteristic values for the vast extent of impairments.Therefore, the only survey available was for the experts. In this case, the prior experts are the parents, who know their child best and are dedicated to his/her daily care. Another group of experts is formed by the therapists and teachers who regularly treat the children and evaluate progress or regress. However, judgments of both groups may also be unreliable, because opinions may vary strongly depending upon momentary impressions, the mood on that particular day and the motivation to answer the survey.For this reason, how reliable the opinions really are, must be carefully evaluated. There are good references for the reliability of these opinions. If both groups agree about how and to which extent the skills of the child have improved after the therapy, then the conclusion can be drawn that the therapy was successful.Hypothesis 3: If there is at least a partial agreement between the ratings of parents and the ratings of teachers and therapists, a certain objective efficiency of dolphin therapy can be assumed.
1.4. Fourth Question: Straw Fire or Continuous Glow?
What would have been gained, if dolphin assisted therapy that is related to substantial costs, which are not yet covered by health insurance companies, a long journey and a high commitment of the parents would only produce short-term successes and the effect then fades away? Surely - the deep emotional experience through the contact with the dolphins is a great gift, but dolphin assisted therapy should mean more than that, especially when the question arises if health insurance companies shall cover the costs of treatment.Therefore the survey was conducted three times among the “experts” –the parents: At the beginning of the therapy, six weeks after the therapy and half a year later.If the positive effect continues or is reinforced, it may be concluded that dolphin assisted therapy crucially contributes to the patients’ improvement, whereby the combination with running long-term therapies may represent a contributing factor to the outcome. Hypothesis: we expect the maintenance of a therapeutic effect over a longer period of time..
2. Method
The whole scientific research was led and implemented by Nicole Kohn, under the supervision and organization of Rolf Oerter.The research followed guidelines of the Declaration of Helsinki and Tokyo for humans, and was approved by the institutional human experimentation committee or equivalent, and that informed consent was obtained.
2.1. Instruments of Investigation
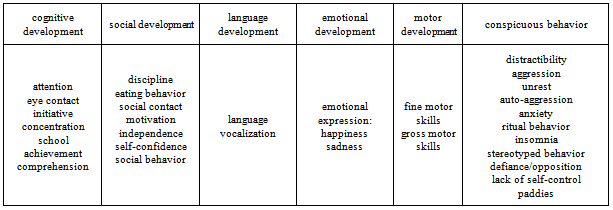
Data of parents and therapists could be included based on designed and prearranged interviews and evaluation scales, neuro-pediatric examination by doctors, microanalysis of videos showing the human- animal interaction and the systematic behavior observations of the veterinarians.The implemented survey procedures were based upon the relevant requirements of the special therapy methods in the USA and in Israel, and were therefore applicable only to them.As follows, we will be limited to the parents’ questionnaire as well as the judgments of the therapists at the respective residence of the participants. They data received from the questionnaire represent the subjective evaluation of parents and therapists/teachers. The questionnaire comprised mainly items regarding competencies and behavior of the patients. Parents were asked to evaluate their child based on a questionnaire of 36 specifics items on a five-subdivision scale: 0 =never; 1 = rarely; 2 = sometimes; 3 = often; 4 = always.The questionnaire with 36 items is subdivided into two parts. The first part (consisting of 24 items) concentrates on the competencies of the patient (e.g. attention, independence), whereas the second part (consisting of 12 items) focuses on behavior observations (e.g. general unrest, aggressiveness). Altogether six dimensions are covered, from which five refer to competencies - cognitive development, social development and autonomy, language development, emotional development and motor function. The sixth dimension refers to behavioral problems. Table 1 gives an overview of the categories of the six domains.Table 1. Domains of the questions posed in the parents’ interview and the questionnaire for Therapists and teachers
 |
| |
|
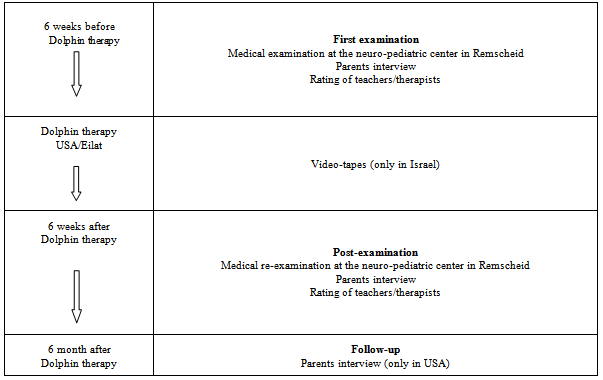
Table 2. Flow-chart of the investigstion
 |
| |
|
At the end of the questionnaire parents indicated how they had found out about dolphin assisted therapy, and described their expectations and the therapeutic expectations about dolphin assisted therapy.The questionnaire was to be submitted three times: before therapy, directly after the therapy and six months later. Based on the responses of the parents or other reference persons the questionnaire prior to therapy includes the “prehistory of the child”, beginning with the personal data such as name, age, address and who fills out the questionnaire, followed by the general description of the impairment, as well as information in reference to when the child began to talk and which therapies and supporting measures have been taken up to that point. The last question specified required information regarding medical procedures, early child development, school history, special developments, therapies in Kindergarten, early support at school and private measures.Parents had to give detailed information how and to which treatments the child has been exposed to in reference to his/her illness. Lastly, they must provide information concerning experiences with animals (e.g. to what extent the child has had experiences with animals and which kind of relationship the child has with the animal), followed by the question whether the child has experience with water (e.g. whether the child fears water or whether it is happy in the water). These questions were skipped in the interview after the therapy. Table 2 shows the flowchart of the longitudinal study.Questionnaires were distributed to the 220 dolphin aid families, who were enrolled at Dolphin Human Therapy (USA). After completion and delivery, a total of 162 pre- and post-interviews, 144 follow-up interview and 99 interviews with therapist/teachers could be collected, corresponding to a return ratio of 83.77 per cent.
2.2. Procedure
The investigation and data collection for this study took place from October 2000 until December 2002. Nicole Kohn conducted the ten video recordings at Dolphin Reef herself, and controlled the distribution and collection of the questionnaires. She organized the recordings in Key Largo as well.Due to the fact that annually only twenty-five children can participate in a dolphin assisted therapy at the Dolphin Reef, and that a certain amount of cancellations must be expected, the author requested mid February 2001 that the organization dolphin aid allow her to contact the parents who enrolled their children to the DHT (Key Largo). It was decided to send an information letter though the organization to inform the parents about the goal and procedure of the study requesting their participation. Furthermore, a declaration of consent was attached.After the declarations of consent had been sent back by the parents, DHT’s program could be included into the study at the beginning of March 2001.In June 2001 Kohn joined DHT (Dolphin Human Therapy) in Key Largo for one week to gain a personal impression of the project and to learn about the exact operational sequence. In order to ensure a continuous and comprehensive data acquisition, dolphin aid supported the research further by providing a research assistant from July through December 2001 whose task was to support parents at DHT on-site to fill out the questionnaires and make the necessary video recordings. For this purpose, shortly before her departure to the USA, the research assistant participated in an application training that lasted several days, and received targeted instructions from Nicole Kohn. After her return she was responsible from January to August 2002 to continue working and handling all incoming questionnaires that had been taken over by Nicole Kohn up to this time.In Israel it took some time at the beginning to build a basis of trust. Nevertheless, cooperation improved continuously and proved to be very productive at the conclusion of the study. Since there were substantial language difficulties with the families that participated in Israel the questionnaire was translated in the course of the time into English, French and Hebrew. The questionnaires returned by the parents were partially incomplete and sometimes very hard to read. Furthermore, the translation into German turned out to be rather difficult.
2.3. Sample
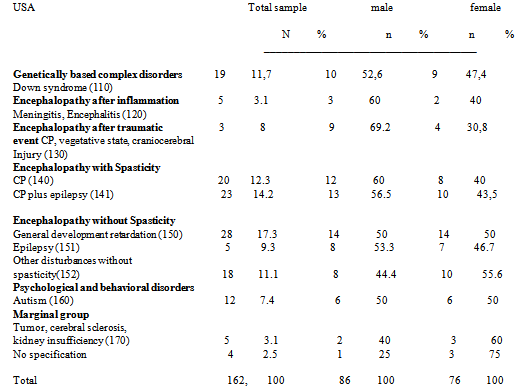
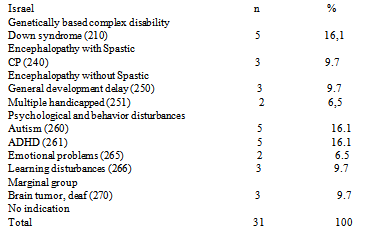
The children and adolescents that underwent the investigation, came from Europe, Israel and USA, one family hailed from the Arab Emirates. Since the participation in dolphin assisted therapy resulted from the parents’ initiative, the medical conditions and the medical diagnoses are collectively inhomogeneous. Therefore, the participants are categorized in groups. Since the data of the medical conditions is based exclusively on information provided by the parents, the indicated medical diagnoses are not subject to an established medical classification like ICD 10, but rather according to disorders with the super ordinate goal of creating a possible comparison chart. Table 3 provides a representation of the grouped disorders from the USA, and table 4 from Israel.The age of the 162 participants in the USA was between two and 30 years at a middle value of nine years (dispersion: 5.09). Participants were most strongly represented in the age of three to ten years (67.8 per cent). In Israel the ages of the 31 participants were between five and 23 years at a middle value of 11.3 years (dispersion: 3.9). Participants were most strongly represented in the age of seven to eleven years (54.84 per cent). The group from the USA consists of 53.1 per cent males and 46.9 per cent females, the Israel sample consists of 71 per cent males and 29 per cent females.Table 3. Distribution of the participants according to disorder from the USA
 |
| |
|
Table 4. Distribution of the participants according to disorders from Israel
 |
| |
|
3. Reliability and Validity of the Data
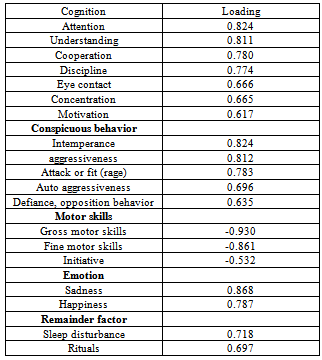
The order of items as shown in table 2 of the six content areas does not ensure that the rater (parents and therapists) arrange the categories in the same manner. a factor revealed “conspicuous behavior” (factor 2), “motor function” (factor 3) and “emotion” (factor 4). However, the dimensions attributed initially to “language” could not be assigned clearly to a factor. Factor 1 consists of items, which had been classified initially under both dimensions “cognition” and “social- emotional behavior”. The fifth factor consists of the items “sleep disturbances” and “rituals”, which were classified before under conspicuous behavior.The total percentage rate of tolerant discrepancy is a satisfactory 64.9 percent, the inter-correlations of the slanted rotating factors is predominantly below .20, only the factors 1 and 4 correlate with .37. Extraction method: Main component analysis; Rotation method: Oblique rotation with Kaiser-normalization; the rotation is convergent in the 7th Iteration.Table 5 represents an overview of the factors that served as a basis for data analysis. Table 5. Loadings of five extracted factors (parents’ ratings before therapy)
 |
| |
|
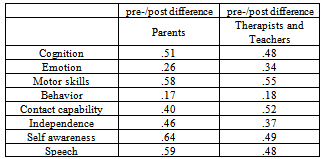
Only the initial four factors will be studied, and thus will be limited to cognition, emotion, and motor and conspicuous behavior. Each time that we refer to the results of these terms, it is concerning the sum of the individual items assigned to the labels, as shown in the above overview.Consistency for the ratings with regard to the grouped items is high. Cronbach’s Alpha lies between .600 and .926. Only the factor “emotion” shows lower values that range between .535 and .767. Re-test reliability between pre- and post-ratings lie over .750 for parents as well as for teachers/therapists. So the scales show satisfying values for consistency of domain-rating and re-test rating.Validity of the ratings is assessed by the comparison of parents’ and TTs’ judgments.The TT-ratings serve as an external criterion for the validity of the parents’ ratings. (External validity). Validity values lie between .411 and .533. Table 6. Pre-/post differences of parents’ and TTs’ rating
 |
| |
|
Thus, the initially stated third question could be positively answered. The judgments are reliable, they can be grouped in four main categories and they are externally valid since TT’s and parents’ ratings show satisfying consistency. Table 6 presents exemplarily results for the factor ‘cognition’
4. Results
4.1. Results I: Therapy Success in the Parents’ Judgments
First we will compare the judgments of the parents before and after the therapy, as well as six months later; thereafter we will compare the TT judgments.For the latter ones, however, only two judgments are available for each case, before and after the therapy. In both instances we rely on the results from the USA, because it represents the largest survey group, and comment on the results from Israel, which are quite similar, and finally, according to the provided individual categories. In case of normal distribution and equivalent error discrepancy we used MW-ANOVA); in case of absent normal distribution and non-equivalent error discrepancy we used the non parameter marginal models (software: www.ams.med.uni-goettingen. de).
4.1.1. Factor Cognition
Figure 1 shows that parents judge the factor of cognition (in which, as described above, co-operation and motivation are included) after the therapy higher than before and six months later still higher. This increase is highly significant (p = 0 .001). The older children lie higher in the success ratings six months later than the younger children.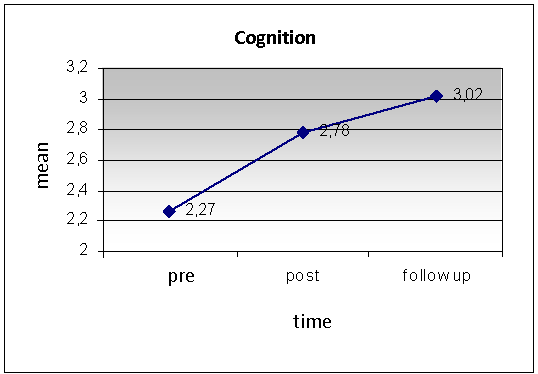 | Figure 1. Parents‘ evaluation of cognition |
Parents positioned their child as very high within the cognition factor after the therapy. This effect aggravate six months later which is remarkable for two reasons: First, six months later parents could not recall their former answers, so a memory effect is unlikely. Second, it seems that the therapy shows its full effect only gradually. We can assume that there are enduring effects of dolphin assisted therapy.In Eilat data exist only before and after the therapy but also here a significant increase of children’s progress was rated by the parents. Although the therapy follows other principles and the child-dolphin contacts are less frequent, the parents judge similarly to the surveys of Key Largo.
4.1.2. Factor ‘Emotion’
The assessment of emotion improves continuously after the therapy. This increase (see also figure 2) is also highly significant (p = .001). In Israel we have an analogous result. Within the factor of emotion the assessment of children’s evaluations was significantly more positive after the therapy.There were also gender and age differences. From the parents’ point of view, contrary to the older girls, the younger girls profit stronger from the therapy. In the group of boys there were no such age differences, they all showed improvement in the parent’s rating.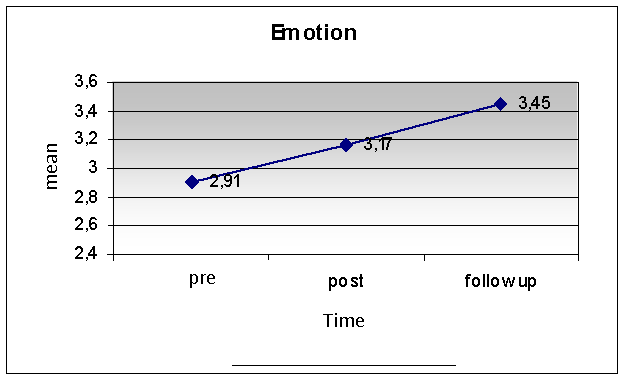 | Figure 2. Parents’ evaluation of emotion |
4.1.3. Factor ‘Motor Function’
In the factor Motor the results are the same as before: a highly significant increase is shown after the therapy, which still continues after six months. Compared to the younger children, the older children still showed a strong increase six months after the therapy. The results in Israel were similar, and showed an increase in parents’ assessment, which was, however, flatter than the American group. Age or gender differences were not found.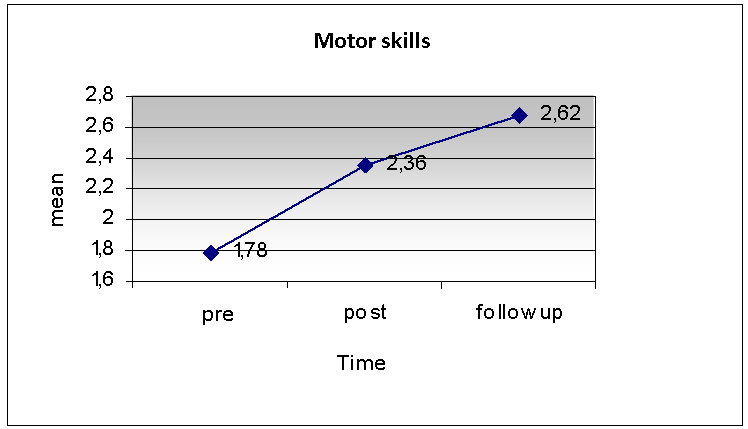 | Figure 3. Parents’ evaluation of motor skills |
4.1.4. Conspicuous Behavior Factor
As can be shown in figure 4, the reported conspicuous behavior decreases, and the curve is descending. Thus, the factor of conspicuous behavior also shows continuous improvement. However, there are remarkable differences between subgroups (see figure 5). According to the opinion of the parents the older male clients did not benefit from the therapy, whereas the younger male clients did. The opposite happened in the group of girls: The younger did not benefit from the therapy, whereas the older clearly did. These results are also statistically significant.The parents’ judgment of the patients from Israel showed a remarkable decrease of conspicuous behavior. The girls benefited stronger than the boys from the therapy, but both sexes showed a decrease of the conspicuous behavior according to the opinion of the parents. No age differences could be noted. That is however possibly due to the lower number of participants (n = 31). The results of some important individual items are presented as follows: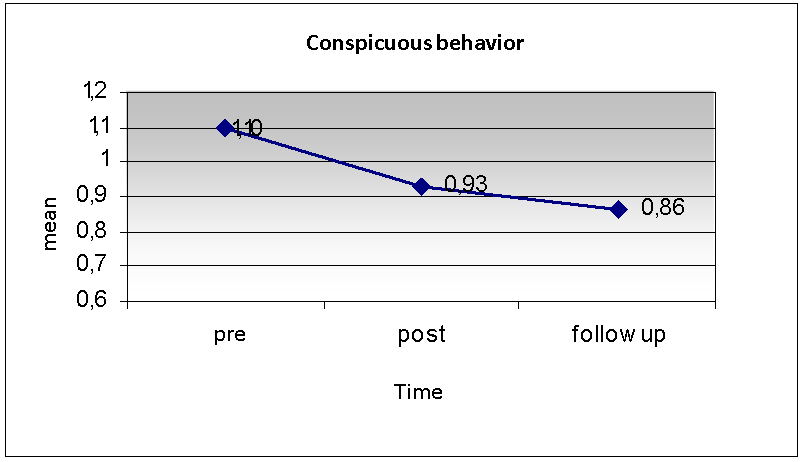 | Figure 4. Parents‘ evaluatin of conspicuous behavior |
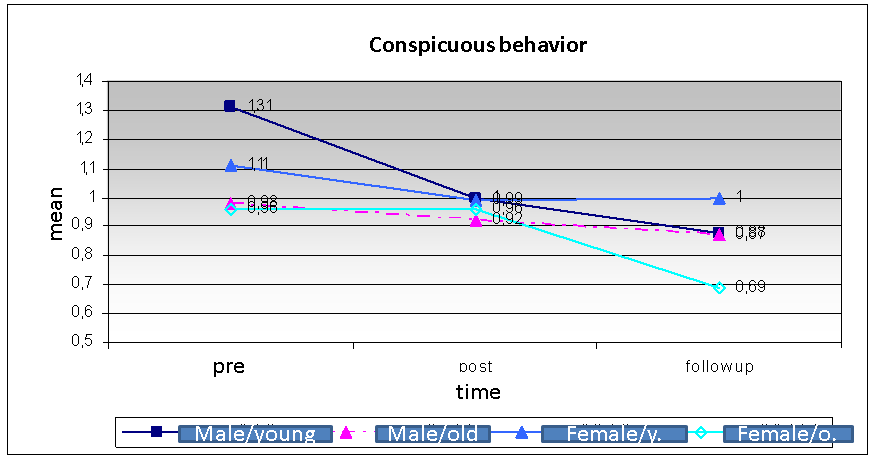 | Figure 5. Dfferences in parents‘ evaluation of younger and older males and females |
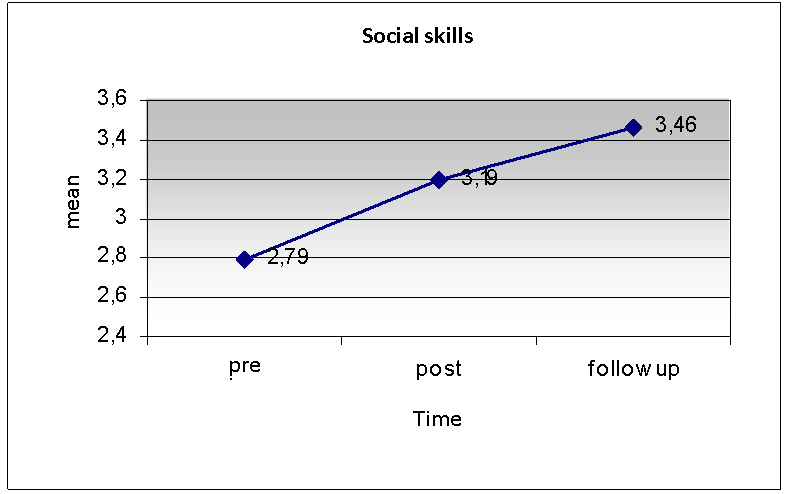 | Figure 6. Parents‘ evaluation of social skills |
4.1.5. Contact Skill
While significant improvements of the contact skills could be certified in the USA, no significant effects of contact skills could be noted in the children in Israel. Figure 6 shows for the US data that the increase continues even after six months.
4.1.6. Independence
Parents assess a continuous improvement of independence for the US sample.Israel showed the same results. Parents evaluated the independence of their children higher after the therapy than before. Like in the USA there were no further effects concerning age and gender.
4.1.7. Self-confidence
The main effect is shown here in the steady increase of the self-confidence curve for the evaluation of the parents. Furthermore, the older children benefited again more than the younger ones, and six months later the increase in the measurement is higher for the older ones than for the younger ones.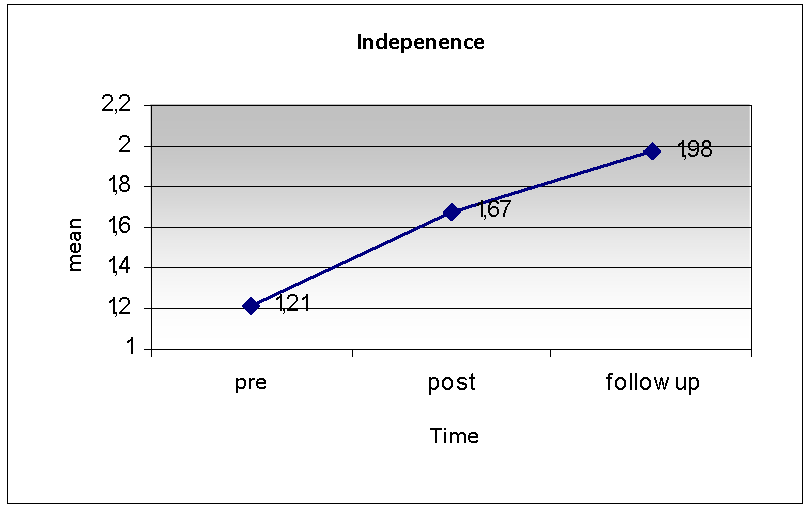 | Figure 7. Parents‘ evaluation of independence |
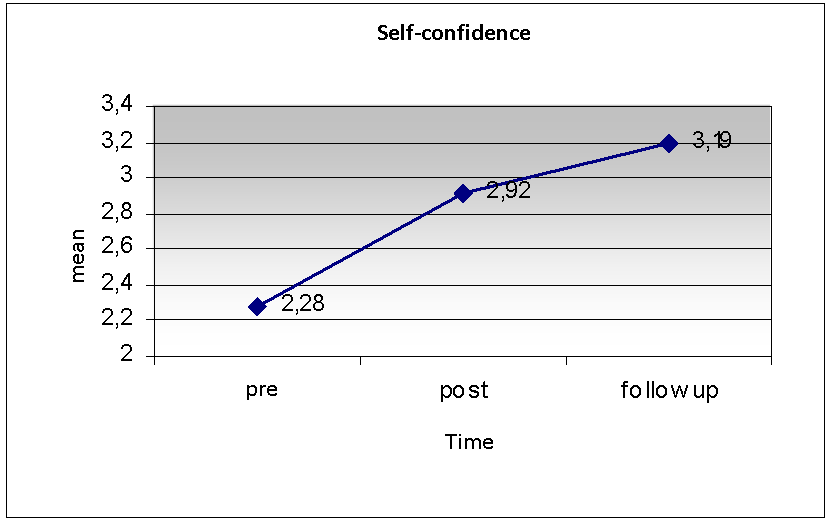 | Figure 8. Parents‘ evaluation of self-confidence |
Once again, the same change was observed in Israel. The self-confidence increased after the therapy according to the evaluation of the parents. It seems that age and gender play an important role. In accordance with the analysis of the statistics the younger girls and the older boys benefited most, whereas the older girls showed no changes in self-confidence.
4.1.8. Language
The linguistic talents improve gradually among the patients from the USA, whereby the main increase lies between the measurement before and after the therapy. Influences of age and gender could not be found. In Israel parents judged similarly. The language competency of the children lie according to their opinion after the therapy higher than before.
4.2. Results II: Teacher/therapist-assessment (TT)
The TT-evaluation took place, as already noted, only twice: before and after the therapy. The post evaluation six months later could not be accomplished, because the therapists and/or other care persons of many patients had changed.We present the results of the four areas cognition, emotion, motor, and conspicuous behavior once more visually in short version.
4.2.1. Cognition, Emotion, Motor Function
In all three areas we find a higher classification after the therapy analogous to the evaluation of the parents. However, the scale values are lower than those of the parent’s judgment. The reason might be that TT judged more carefully on the one hand, and therefore assigned lower values in general, and on the other hand they have the comparison with many patients, while such a reference system is not available to the parents. Generally speaking however, the similarity of the assessment of the therapy success is astonishing. Figure 10 summarizes the results of cognition, emotion and motor skills.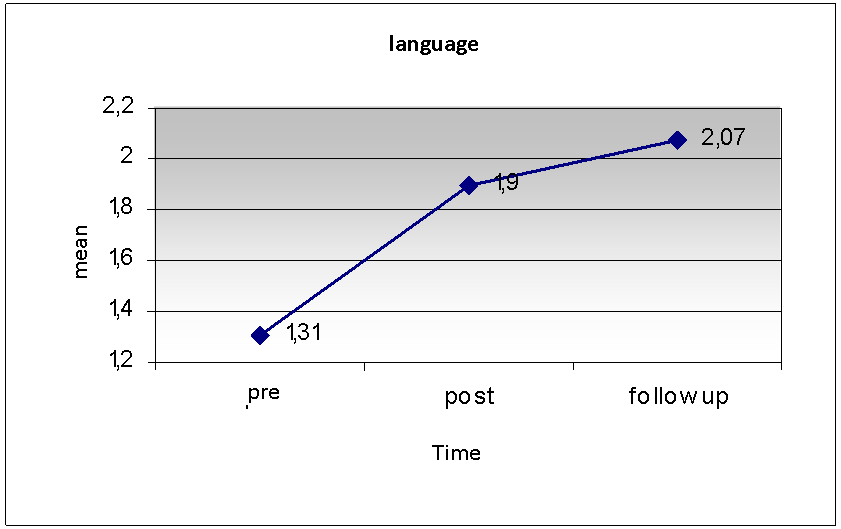 | Figure 9. Parents‘ evaluation of language skills |
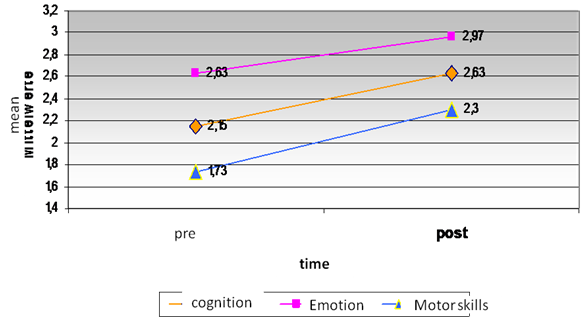 | Figure 10. Ratings of therapists and teachers for cognition, emotion and motor skills |
4.2.2. Conspicuous Behavior
The conspicuous behavior also shows a parallel course compared with parents’ evaluation. The evaluated decrease of the conspicuous behavior is again highly significant.
4.3. Results III: Comparison of the Disorder Groups
In the following we concentrate on the differences between disorder groups. As already initially mentioned, the treated children form an extraordinarily heterogeneous group. It is naturally of high interest whether dolphin assisted therapy helps for all groups, or whether it is inappropriate for some types of disturbances. Furthermore, one must take into consideration that the initial level of disorder varies according to the type of disturbance. Consider the contact skills of autistic people, which lie in general lower than many other types of disturbances. The motor function is for instance substantially better for children with Down syndrome than for children that suffer from cerebral palsy.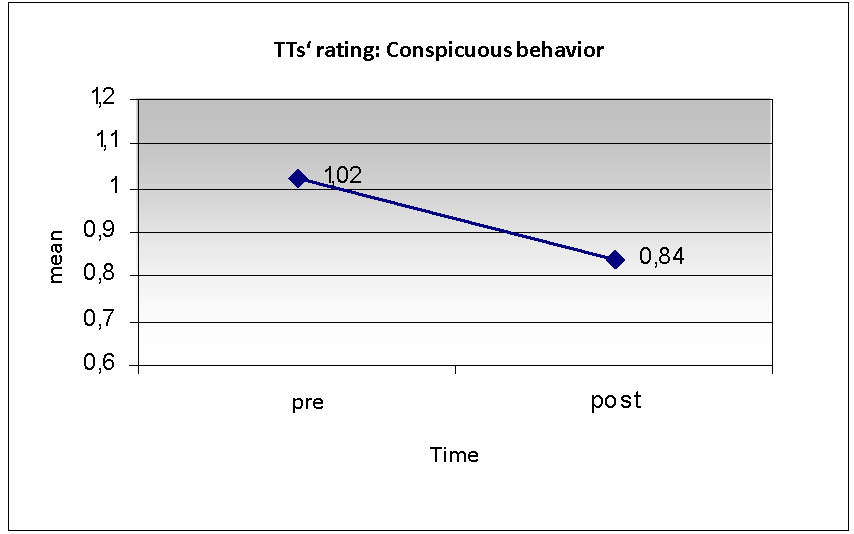 | Figure 11. Ratings of therapists and teachers for conspicuous behavior |
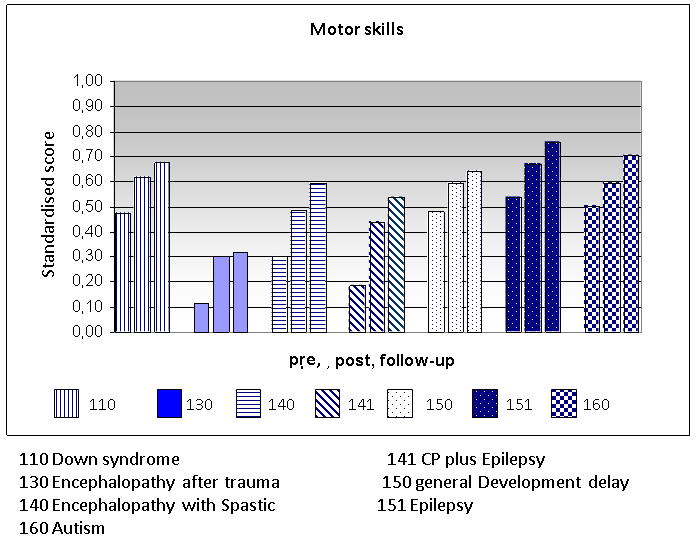 | Figure 13. Comparison between disorder groups for the domain ‚motor skills‘ |
The comparisons that follow are taken from judgments of the parents in the USA, because we dispose of three values (pre, post, follow-up).Let’s look again at the evaluation of cognition. All the seven types of listed disturbances show a gradual increase even at the third point of evaluation (six months later) (figure12).On the other hand, the motor function shows clear differences between the groups. As figure 13 shows, the values of children with encephalopathy after trauma do not increase after six months. The drastic increases of ratings for patients with encephalopathy with Spastic and of patients with cerebral palsy plus epilepsy are remarkable.The consistent picture clearly changes with conspicuous behavior. Children with encephalopathy after trauma and with encephalopathy with spastic do not show a lasting success. The final values after six months are practically identical to the initial values. All remaining groups show the typical gradual steps, only this time reversed as the values of the conspicuous behavior decrease (figure 14).From the numerous specific results again three are selected: the assessment of contact skills, independence and language.With regard to contact ability and independence factors the values for all groups of disturbances increase gradually, a result that corresponds totally to the earlier reported results (figure 15 and 16). The assessment of linguistic achievements however does not follow this scheme. Mainly, there is no increase in the majority of the disturbance cases after six months. Children with Down syndrome are classified equal as before the therapy. This result is one of the few that does not correspond to the general picture of constant progress half a year later (figure 17).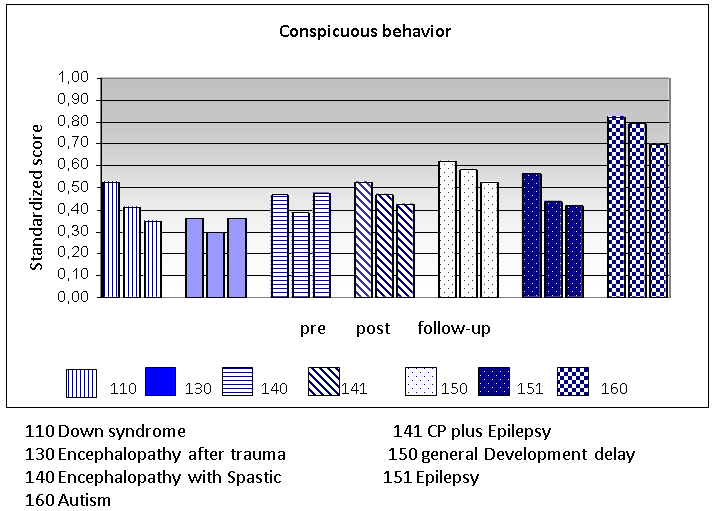 | Figure 14. Comparison of disorder groups for conspicuous behavior |
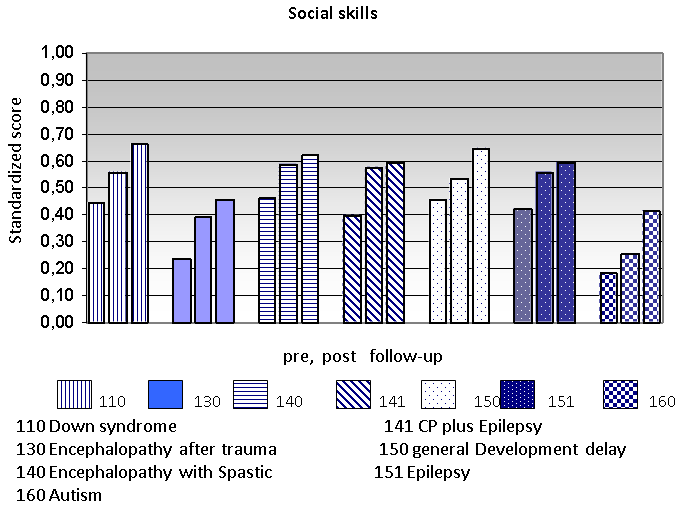 | Figures 15. Comparison of disorder groups for social skills |
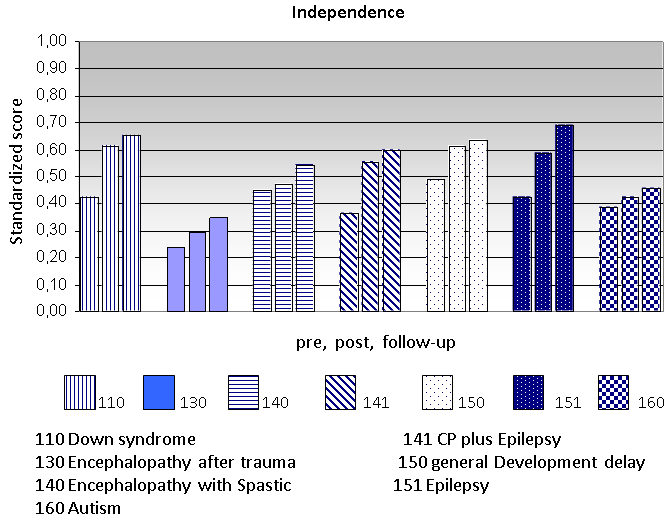 | Figure 16. Comparison of disorder groups for independence |
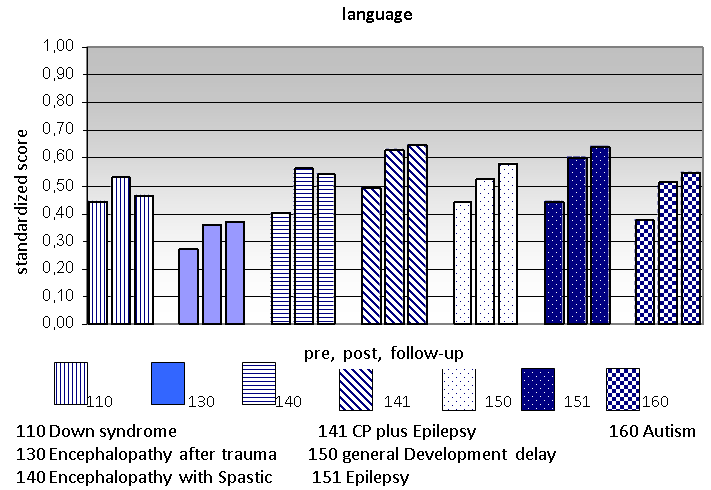 | Figure 17. Comparison beetween disorder groups for language skills |
5. Discussion: How does Dolphin Therapy Work?
Now we are in the position to answer the initially asked questions, and furthermore, to try a general evaluation of the efficiency of dolphin assisted therapy.
5.1. Different Forms of Dolphin Assisted Therapy Show Similar Results
The comparison between Eilat (Israel) and Key Largo (USA) demonstrate in an impressive way the similarity between the outcomes of the therapies. However, since the concepts clearly differ in detail, the success cannot be ascribed to general conditions like supporting social measures, the landscape and the water as a wellness medium, but by the dolphin himself, because he is, to a certain extent, the only constant factor in the therapy. For example, in Eilat there is no additional systematic program for the children as it is the case in Key Largo. The water in Eilat is rather cool compare with the warm water in Key Largo. So it seems at least preliminary plausible that hypothesis 1 is confirmed.
5.2. The Result of Dolphin Assisted Therapy is Similar in Different Groups of Disabilities
Particularly remarkable and favorable are the findings about the effect on different groups of disabilities. Surprisingly, the effects in the improvement of cognition, emotion, motor skills and behavior disorder, as well as in other individual areas (independence, language, self-awareness, contact ability, social and daily living skills) can be shown more or less among all groups of disabilities included in the study. This means that dolphin therapy works “nonspecifically“, i.e., the promoting influence goes back less to specific effects, but can be generally observed on the diverse degrees and types of impairments. It is therefore no miracle that the interaction with dolphins shows also positive effects on healthy people who suffer under stress, as is a longer lastin effect of repeatedly reported.Of course, this statistically valid general effect does not mean that success can be recorded for each individual case. Our results are based upon average group values and the dispersions. Since mean differences are significant in spite of high individual variance, the overwhelming majority of subjects profits from the therapy.So, Hypothesis 2 could not be confirmed. It seems that dolphin therapy works nonspecifically.
5.3. Dolphin Assisted Therapy has a Long Term Effect
Perhaps the most important findings of our data lie in the proof that between the evaluations of the competencies a thorough increase takes place even six months after the therapy. The new updated higher evaluation results of the progress cannot be reduced to a memory effect, because the parents surely do not remember their assessment six months earlier.The increased values in the evaluation half a year later confirm the past sporadically gained knowledge that dolphin assisted therapy does not show its main effect immediately, but that it rather increases within a longer term after the therapy.Since the first evaluation was performed six weeks after conclusion of the therapy, the given values do not derive from an instant impression either. Parents have gained distance, have returned to their normal domestic chores, and have already forgotten the values that they gave their child before the therapy.It would be interesting to follow-up the development of the treated patients in order to find out whether the past long-term effect still continues. Certainly there will be many other influences (school, other therapies, family changes) that might make it difficult to isolate the effects of dolphin assisted therapy. For the time being we can assume that dolphin assisted therapy shows its effect over a longer period of time.With regard to our hypothesis 3, one should expect that further research will confirm a longer lasting effect of dolphin therapy at least for half a year.
5.4. Therapists and Teachers Rate Lower than the Parents but Concordant with Them
Since most values of the TT ratings lie lower than the parent’s judgment, one could assume that the TTs judge the success of the therapy lower than the parents. We already stated the fact that TTs have another reference system of assessment than the parents. Therefore, lower values themselves do not necessarily reflect a lower success rate. What really counts is the difference between pre and post evaluation. If the differences between parents and TTs are more or less alike, then both groups rate success of the therapy similarly. Table 6 shows the increase (pre-/post assessment differences) for the different domains.As the table shows, the estimated differences are quite similar, i.e. TTs and parents rate the positive effects of dolphin assisted therapy in a similar way. Only the domains of self awareness and language show that the two groups lie apart by more than 0,10 points. The TTs evaluate the progress within the range emotion and contact capability higher than the parents. This result is remarkable, since when using a more careful (here lower) system of evaluation it is actually expected that the estimated success factor should also be lower. The similarity of TTs’ and parents’ rating is an important argument for the validity of the findings. Hypothesis 4 is confirmed, there as a concordance between parents’ and TTs’ ratings. The lower level of values given by the TTs fits this assumption because there frame of reference (many handicapped children) is broad whereas the Parents have only experience with one child and usually no opportunity of comparision.
6. Concluding Remarks
The results presented above demonstrate an impressive positive effect of dolphin assisted therapy. Parents’ ratings are highly reliable with regard to internal consistency (Cronbach’s alpha) and re-test reliability. The data are valid if one put the TTs’ judgments as external criterion. Since positive effects occur under very different conditions (Eilat versus Key Largo) and the dolphin is the only constant condition, the therapeutic success indeed seems mainly to depend on the interaction between dolphin and patent. Nevertheless, we assume a systemic effect beyond this human-animal interaction. The combination of many factors, as for instance the new environment, the water that gives the sense of weightlessness, the new therapists and care persons and last not the least the parents, who experience a different connection during the journey and on site may contribute to the success. The main source of the positive effect of the therapy still seems to be the dolphin.Three studies provide evidence how the interaction between Dolphin and patient works (Stenczel,[10]; Beeck,[11]). These studies analyzed tens of thousands video-taped interactions between dolphin and patient and provide evidence about the quality of animal-human interaction. Further studies should include objective tests and neurological measurements during dolphin therapy in order to receive data about what happens in interaction between dolphin and child.Statement: The study was funded by the University of Munich and by the organization “dolphin aid” which wanted to know whether its engagement in dolphin therapy is justified.
References
| [1] | Nathanson, D. E. (1998). Long-term Effectiveness of Dolphin-assisted Therapy for Children with Severe Disabilities. Anthrozoös 11(1), 22. |
| [2] | Dilts, R. (2008). A summative evaluation of a dolphin assisted therapy Program for children with special needs. Unv. Dissertation. Oregon State University. |
| [3] | Humphries, T.L. (2003). Effectiveness of dolphin-assisted therapy as a behavioral intervention for young children with disabilities. Bridges: Practice-Based Research Synthesis 1(6), 1-9. |
| [4] | Likura, Y., Sakamotoa, Y., Imaia, T. , Akaia, L., Matsuokaa, T., Sugiharaa, K., Utumib, M. & Tomikawac, M. (2001). Dolphin-Assisted Seawater Therapy for Severe Atopic Dermatitis: An Immunological and Psychological Study. International Archives of Allergy and Immunology, 124, 389–390. |
| [5] | Lukina, L. (1999). Influence of dolphin-assisted therapy sessions on the functional state of children with psychoneurological symptoms of diseases. Human Physiology, 25, 676-679. |
| [6] | Kohn, N. (2004). Delphin-Therapie. Untersuchungen zur therapeutischen Wirksamkeit. Frankfurt: Lang. |
| [7] | Dilts, R., Trompisch, N & Bergquist, T. (2011). Dolphin assisted therapy for children with special needs: A pilot study. Journal of Creativity in Mental Health (6), 56-58. |
| [8] | Breitenbach, E., von Fersen, L., Stumpf, E. & Ebert, H. (2006). Delfin-Therapie für Kinder mit Behinderungen. Analyse und Erklärung der Wirksamkeit. Edition Bentheim/Würzburg. |
| [9] | Poizat, S. (2003). Contribution a l´étude des interactions comportementales entre l´homme et le dauphin (tursiops truncatus) au dolphin reef d´Eilat, Israel. Unv. Dissertation. École Nationale Veterinaire de Lyon. |
| [10] | Stenczel, Z. (2004). Kommunikation zwischen Delphin und Kind. In: K. Kuhnert (ed.). Delphintherapie – Beweis eines Wunders (S. 143-2158. München: Ariston. |
| [11] | Beeck, F. (2004). Erfolgserlebnis und Selbstwirksamkeits wahrnehmung in der Delphintherapie. In: K. Kuhnert (ed.). Delphintherapie – Beweis eines Wunders (S. 184-200). München: Ariston. |
| [12] | Kruger, K.A. & Serpell, J.A. (2006). Animal-assisted interventions in mental health: Definitions and theoretical foundations, In A.H. Fine, (Ed.), Handbook on animal-assisted therapy: Theoretical foundations and guidelines for practice. (pp. 21-38), Academic Press, San Diego, CA. |
| [13] | Prothman, A. (2006). Tiergestützte Kinderpsychotherapie. Frankfurt, Lang |
| [14] | Serpell, J.A., Coppinger, R., Fine, A.H., Peralta, J.M. (2010). Welfare considerations in therapy and assistance animals. A.H. Fine (Hrsg.), Handbook on Animal-Assisted Therapy. (481-503). Amsterdam: Elsevier. |
| [15] | Scheer, M. (2005). Können Delfine heilen? Neue wissenschaftliche Befunde zum Thema „delfinassistierte Therapie“. Krankendienst 7, 208-211. |
| [16] | Marino, L. & Lilienfeld, S. (2007). Dolphin-Assisted Therapy: More Flawed Data and More Flawed Conclusions, Anthrozoös, 20 (3), S. 239 – 249. |
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML