-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Brain and Cognitive Sciences
p-ISSN: 2163-1840 e-ISSN: 2163-1867
2020; 9(2): 25-28
doi:10.5923/j.ijbcs.20200902.01

Using the Numicon Program and Evaluating Intellectual Development in Children with Down Syndrome
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSalikhova Saodatkhon Mukhamadkhanovna1, Madjidova Yakutkhon Nabiyevna1, Salikhova Kamola Shavkatovna2
1Department of Neurology, Pediatric Neurology and Medical Genetics, Tashkent Pediatric Medical Institute, Tashkent, Uzbekistan
2Republican Specialized Scientific and Practical Medical Center of Pediatrics, Tashkent, Uzbekistan
Correspondence to: Salikhova Saodatkhon Mukhamadkhanovna, Department of Neurology, Pediatric Neurology and Medical Genetics, Tashkent Pediatric Medical Institute, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2020 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Down syndrome is a genetic disorder that can lead to mental retardation of varying degrees. It is one of the most prevalent neurodevelopmental disorders, occurring in about 1 of 800 live births throughout the world. The Stanford Binet scale is the most applicable for studying the intellectual development of children aged from 3 to 5 years. The study involved 30 children with Down syndrome aged from 3 to 6 years, brought up in a non-governmental educational institution “Umnichka” in Tashkent, Uzbekistan. This article presents results of using multi-sensory Numicon scheme which is an indispensable and valuable tool to help how to count for children with Down syndrome.
Keywords: Down syndrome, Mental retardation, the Stanford Binet scale, Intellectual development, Numicon program, Children, Uzbekistan
Cite this paper: Salikhova Saodatkhon Mukhamadkhanovna, Madjidova Yakutkhon Nabiyevna, Salikhova Kamola Shavkatovna, Using the Numicon Program and Evaluating Intellectual Development in Children with Down Syndrome, International Journal of Brain and Cognitive Sciences, Vol. 9 No. 2, 2020, pp. 25-28. doi: 10.5923/j.ijbcs.20200902.01.
Article Outline
1. Introduction.
- Down syndrome (trisomy on chromosome 21) is the most common genetic abnormality. People with Down syndrome (DS) have 47 chromosomes (instead of the usual 46); since the chromosomes of the 21st pair are represented by three copies instead of the normal two (hence the name Trisomy is one of the names of Down syndrome). According to the World Health Organization statistics, 1 in 600-800 newborns are born with DS. This ratio is the same in different countries, climatic zones and social strata [1,2]. The presence of an additional chromosome leads to appear a number of features, as a result of which the child will develop more slowly than his peers. It is more difficult to the children with DS to learn, walk, eat, talk, play and make friends, go to school and play sports. Individuals with DS probably comprise the majority of infants and children with mental retardation [2-4].The risk of having a child with trisomy 21 is the highest in women who conceive after age 35 year. Even though younger women have a lower risk, they represent half of all mothers with babies with DS because of their higher overall birth rate. For that, all women should be offered screening for DS in their 2nd trimester by means of 4 maternal serum tests (free β-human chorionic gonadotropin [β-hCG], unconjugated estriol, inhibin, and α-fetoprotein) [5].Among the features of the neuroanatomical structure of children with DS, one can note a reduced total mass of the brain, a reduced size of the cerebellum and brain stem, which complicates the formation of equilibrium reactions and the implementation of activities that require coordination. The number of convolutions and neurons in the cerebral cortex is also less than normal; myelination is insufficient [4-7]. Due to the lower frequency of arrangement of neurons and long distance between synapses, the integration of the flow of stimuli is slower, the response is also slowed down and a reduced sensitivity to temperature, pressure on the surface of the body (violation of tactile functions) is possible [5,8-10]. The brains of individuals with DS are typically smaller than those of age‐matched controls, at least after 6 months of age. One possibility that has been given insufficient attention in the past is that this difference is a consequence of the fact that DS individuals have smaller bodies [3,10]. Fortunately, in these children hand-eye centers (parietal lobes) are better developed, therefore training based on hand-eye perception (hand-eye) is the most successful [1,2,11].Choosing a strategy and tactics for teaching children with DS, it should be borne in mind that they succeed best if the maximum number of sensory channels (vision, hearing, touch, smell) is involved [12,13]. It is also important to note the presence in children with DS of specific sensory interests associated with low tactile and proprioceptive sensitivity.When studying mathematics, children with DS face the greatest difficulties. This is due to the fact that mathematical operations require a rather high level of abstract thinking, good short-term memory and the ability to operate with several concepts at the same time. Understanding of cause and effect relationships, relativity of concepts, comparison, as well as the use of the “mathematical language” is required - with which children with DS have problems [13-15].For children with DS, Numicon is an indispensable and valuable tool to help how to count. Numicon is a program and a set of visual material created in England in 1996-1998 years for those children who have difficulty learning math. Numicon is a multi-sensory scheme designed to teach number to typically developing pre-school and primary school children [6,9,16]. One of the key features of the scheme is that it provides children with visual representations of whole numbers which help to develop a mental imagery for numbers, which in turn supports mental arithmetic. This is done by using the structured materials in multisensory play activities. Given the visual strengths of many children with DS [17,18] it is thought that Numicon can be an effective aid for them in learning number of skills.
2. The Purpose of This Study
- The purpose of this study was to evaluate the impact of the Numicon program on the intellectual development of children with DS.
3. Research Methods
- The study involved 30 children with DS aged from 3 to 6 years, brought up in a non-governmental educational institution “Umnichka” in Tashkent, Uzbekistan. First, our research studied maternal age at the time of birth proband. Second, considering that the children with DS examined by us had signs of mental retardation, we used the Stanford Binet scale for a more objective assessment. The scale is designed to measure IQ from 3 to 5 years, which consisted of six questions for each age level. It took 30 minutes to evaluate an intellectual status of a person with DS.The ICD-10 criteria for intellectual disability include adaptive behavior in addition to cognitive abilities. The severity of intellectual disability was scored from 1 to 4 according to the best level achieved by each individual as follows: mild (IQ 50-69) 1, moderate (IQ 35-49) 2, severe (IQ 20-34) 3, profound intellectual disability (IQ < 20) 4.For each child we used the Numicon program during 10 months. In Numicon, numbers from 1 to 10 are represented by plastic forms-templates of different colors, so that the numbers become available for visual and tactile perception. Numicon’s forms are designed so that children can manipulate them, learn to recognize patterns and relate them to the corresponding numbers. Moreover, all cases had confirmed genetically; all had complete trisomy on chromosome 21 (karyotype analyzes had performed at the Republican Screening Center).
4. Study Results
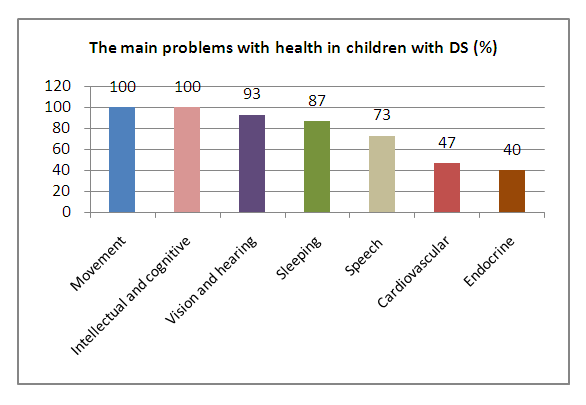
- The average age of the observed children was 4.5 ± 1.04 years. All registered children with DS experienced various difficulties with nutrition, swallowing and speech due to the high arched sky, small upper jaw, as well as low muscle tone in the tongue and weak muscles of the mouth. The main neurological, cardio-vascular and endocrine problems were showed in the first graph.
 | Graph 1 |
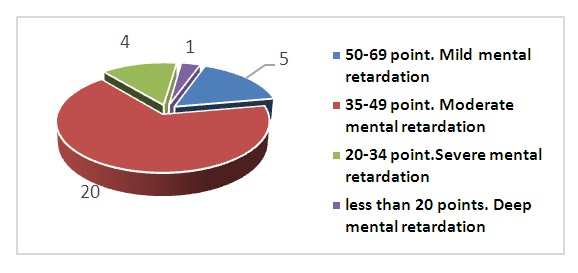 | Diagram 2. Distribution of children with Down syndrome according to the level of intellectual development based on the results of the Stanford-Binet scale (according to ICD-10) |
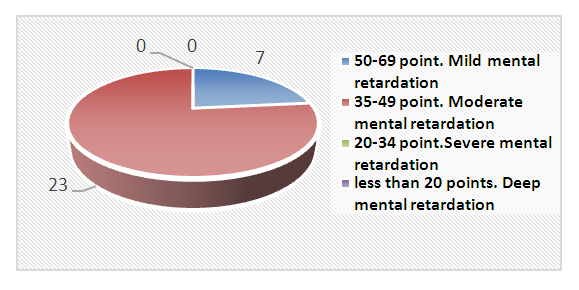 | Diagram 3. Results of mental development (after a year) |
5. Conclusions
- Almost all children observed varying neurological changes such as muscle hypotension, speech and mental deficits. From the speech disorders: dysarthria prevailed in the examined children. Analysis of the distribution of mothers by age revealed the birth of proband more often in women aged 26-35 years. Well under a half of children with DS (47%) had pathology of the cardiovascular system. In children with DS, the amount of short-term memory is limited, so, it is difficult for them to keep intermediate results of calculations in their minds, which means that additional visual support is needed. The Numicon technique allows children to develop fine motor skills, the psyche, helps to approach the implementation of elementary counting operations in the mind, focusing on images of forms that indicate quantities, which means that oral counting becomes more accessible. Numicon was only part of the child's experience with numbers, so on each of the activity cards there were suggestions for making connections with other activities that reinforce the learning and help the child to use and apply the new understanding. Importantly, from the very beginning, children needed to be learning and practicing their counting alongside all Numicon activities.