-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Brain and Cognitive Sciences
p-ISSN: 2163-1840 e-ISSN: 2163-1867
2018; 7(1): 1-8
doi:10.5923/j.ijbcs.20180701.01

The Relationship between Self-esteem and Emotional Intelligence among Undergraduate Medical Students of Imo State University, Owerri, Nigeria
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLEgwurugwu Jude Nnabuife1, Ohamaeme Moses Chukwuemeka2, Ugwuezumba Patrick Chinwendu1, Dike Ephraim I.3, Eberendu Ikechukwu4
1Department of Human Physiology, College of Medicine, Imo Sate University, Owerri, Nigeria
2Department of Community Medicine, Nnamdi Azikiwe University Teaching Hospital, Nnewi, Nigeria
3Department of Obstetric and Gynaecology, Imo State University Teaching Hospital, Orlu, Nigeria
4Department of Paediatrics, Imo State University Teaching Hospital, Orlu, Nigeria
Correspondence to: Egwurugwu Jude Nnabuife, Department of Human Physiology, College of Medicine, Imo Sate University, Owerri, Nigeria.
| Email: |  |
Copyright © 2018 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

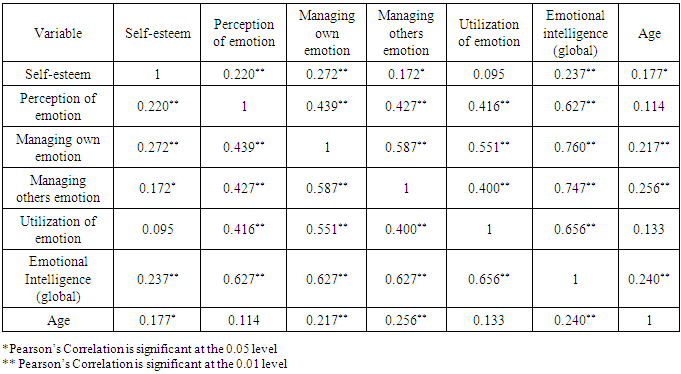
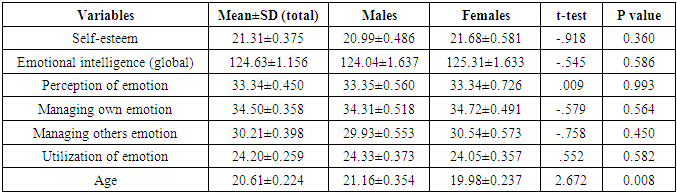
The medical profession requires personnel who most times should be happy, confident, competent, social and a good team player. These good interpersonal behaviours are paramount for effective and productive medical practice. This study was undertaken to assess the relationship between self-esteem and emotional intelligence among undergraduate medical students of Imo State University, Owerri, Nigeria. One hundred and forty students consented to and participated in the study. Rosenberg Self-Esteem scale and Schutte Emotional Intelligence Test were used to assess self-esteem and emotional intelligence respectively. Results showed significant and positive correlation between self-esteem and global emotional intelligence (r = 0.237, p = 0.001), perception of emotion (r= 0.220, p = 0.001), management of own emotion (r = 0.272, p = 0.001), management of others’ emotion (r = 0.172, p = 0.05), and age (r = 0.177, p = 0.05). The medical students also had high levels of self-esteem (21.31±0.375), global emotional intelligence (124.63±1.156), perception of emotion (33.34±0.450), management of own emotion (34.50±0.358), management of others’ emotion (30.21±0.398) and utilization of emotion (24.20±0.259). No gender differences were noted in the variables. In conclusion, respondents exhibited high level of self-esteem and were emotionally intelligent. Self-esteem correlated positively and strongly with emotional intelligence. Medical schools should include self-esteem and emotional intelligence tests as part of their criteria for assessing medical students.
Keywords: Self-esteem, Emotional intelligence, Medical student, Interpersonal behaviour
Cite this paper: Egwurugwu Jude Nnabuife, Ohamaeme Moses Chukwuemeka, Ugwuezumba Patrick Chinwendu, Dike Ephraim I., Eberendu Ikechukwu, The Relationship between Self-esteem and Emotional Intelligence among Undergraduate Medical Students of Imo State University, Owerri, Nigeria, International Journal of Brain and Cognitive Sciences, Vol. 7 No. 1, 2018, pp. 1-8. doi: 10.5923/j.ijbcs.20180701.01.
1. Introduction
- Emotional intelligence (EI) is a multi-faceted construct that consists of our ability to perceive, monitor, regulate and use emotions [1-4]. The concept, EI, has been given many definitions and explanations. It was introduced in 1990 by Mayer and Salovey [1] and to them, it is the capacity to process emotional information accurately and effectively, including the ability to monitor one’s own and others’ feelings and emotions, discriminate among them and use this information to guide one’s thinking and actions. EI has also been defined as the ability to correctly understand, evaluate and communicate emotions [5]. EI includes cognition, perception, expression of emotion, emotional facilitation, understanding emotion, management and regulation of emotion in order to improve and develop emotional intelligence [6]. It is now obvious that majority of the conceptualizations of this construct, address one or more of the following basic components: (a) the ability to be aware of and express emotion; (b) the ability to be aware of others’ feelings; (c) the ability to manage and regulate emotions; (d) the ability to realistically and flexibly cope with the immediate situation; and (e) the ability to generate positive affect in order to be sufficiently self-motivated to achieve personal goals [7]. Theoretically, EI refers essentially to the cooperative combination of intelligence and emotion [8-10]. EI connects with several cutting-edge areas of psychological science, such as the neuroscience of emotion, self-regulation theory, studies of meta-cognition, and the search for human abilities beyond ‘traditional’ academic intelligence [11]. Neuro-imaging studies have shown that the various components of EI are supported by separate neural substrates. The Social Cognition Network (SCN) facilitates the understanding of other’s feelings, thoughts or desires [12-14]. The SCN includes the medial Prefrontal Cortex (mPFC) and the Superior Temporal Sulcus (STS), which show altered activity during face recognition and mental state attribution [13], and the Tempo-Parietal Junction (TPJ), which is associated with the process of inferring temporal states such as the goals, intentions, and desires of other people [14]. Furthermore, the Inferior Frontal Gyrus (IFG), amygdale, anterior cingulate cortex, and anterior insular are also important portions of the SCN [13]. Leppanen and Nelson [15] have demonstrated that the neural systems involved in processing emotional signals from faces include the amygdale, Orbito-Frontal Cortex (OFC), fusiform gyrus and posterior STS.Positive emotional intelligence is a strong predictor of better psychological adjustment than high self-esteem whereas negative or low emotional intelligence is significantly related to depression, harmful and distressing behaviors [16]. Studies have shown that sad mood can be attributed to low level of EI [17, 18]. It has also been found that people with high emotional intelligent have ability to mend their pessimist thinking and mood state [19]. EI is related to other mental health variables and is significantly correlated to higher levels of self-esteem and positive mood among individuals [20]. It has also been demonstrated that persons with high level of EI tend to have more positive traits, are happier, and more successful in life than others [21-23]. They have more adaptive ways of coping [24, 25], have better interpersonal relations [26], and tend to achieve better academic results [23, 27]. Hence, EI has been adjudged a strong protective factor in both physical and mental health [28]. The concept of self-esteem cuts across all age brackets, starting from infants to late adulthood; it is the totality of one’s self-evaluation [29]. Self-esteem can be described as the evaluation and experience related to self value, the perception of self ability as well as the acceptance of the whole self, which an individual obtains during the process of socialization [30, 31]. Self-esteem is an individual’s feelings, thoughts and evaluations of his abilities in social, educational, familial and body image domains [32]. Evidences abound that a person with high self-esteem has a high level of mental health and self-harmony [33], feels more competent, more confident, has more active engagement in daily activities, is more productive, tends to exhibit optimistic attitudes and sound psychological health [34-37]. Furthermore such a person has self-direction, non-blaming others, demonstrates personal strength, ability to solve problems and ability to control emotions [29]. On the other hand, a person with low self-esteem often feels desperate, inferior, hopeless, unhappy and may get neurosis, depression and high suicidal ideation [34, 38-40]. It has been shown that self-esteem affects not only present physical and mental health and associated health-related behaviors but also impacts on future health and health-related behaviors during adulthood [41]. Self-esteem is a very useful tool for health care professionals during their interactions with patients, caregivers, other health care team members, hospital management [42, 43] as well as medical students. Baumeister and co-workers [44] also demonstrated that high self esteem leads to healthier performances and remarkable interpersonal success, leading to improved happiness and a healthier way of life. Furthermore, it has been shown that health care professionals with high self-esteem have a tendency to stimulate, influence and induce a positive well-being both in the health care team and in patients [45]. Therefore, strong positive mental health behavior as depicted by high self-esteem and EI are imperative for effective and efficient medical practice. To the best of our knowledge, no work has been done to assess the relationship between self-esteem and emotional intelligence among Nigerian medical students, thus this study.
2. Materials and Methods
- This cross-sectional analytic study using non-probability sampling technique was conducted among pre-clinical undergraduate medical students of Imo State University, Owerri, Nigeria. All the pre-clinical students numbering 170 as at September, 2017 were invited to participate in the research. The aim and objectives of the study were thoroughly explained to the students. Those who agreed to participate, signed the written informed consent forms. Participation was therefore completely voluntary, anonymous and confidentiality of the information generated was ensured. The research was approved by the Ethical Committee of Imo State University, Owerri.Standardized questionnaires of the Rosenberg Self-Esteem scale and Schutte’s Emotional Intelligence scale were used for the study. One hundred and forty pre-clinical medical students out of the 170 recruited for the study, filled and returned their questionnaires (participation rate of 82%). The Rosenberg Self-Esteem scale is one of the most widely used self-esteem instruments. It is a ten-item self –reporting scale that assesses a person’s overall sense of self-esteem. Each statement on the scale is answered on a four point scale (Likert scoring 0-1-2-3) with the scoring ranging from 0 to 30. Rosenberg self-esteem scale has strong internal reliability: test-retest correlations are in the range of 0.76 to 0.88, and Cronbach’s alpha in the range of 0.77 to 0.88 [46-49]. A cronbach alpha of 0.84 and two week test-retest reliability coefficient of 0.76 has been established in a Nigerian study [49]. For the present study, the calculated internal consistency reliability was 0.82.The Schutte Self-Report Emotional Intelligence Test (SSEIT) is a 33-item self-report measure of emotional intelligence developed by Schutte et al [17]. The scale was based on Salovey and Mayer’s (1990) original model of emotional intelligence [1]. The most widely used subscales derived from the 33-item SSEIT are based on factors identified [16, 50, 51]. The four subscales include: perception of emotions, management of own emotion, management of others emotion and utilization of emotion. The items on the scale comprising the subscales are as follows: Perception of emotion (items 5, 9, 15, 18, 19, 22, 25, 29, 32, 33), Managing Own Emotion (items 2, 3, 10, 12, 14, 21, 23, 28, 31), Managing Others’ Emotion (items 1, 4, 11, 13, 16, 24, 26, 30), and Utilization of Emotion (items 6, 7, 8, 17, 20, 27). Respondents rate themselves on the items using a five-point scale. Items 5, 28 and 33 are scored on the reverse order. Total scores can range from 33 to 165 with higher scores indicating higher emotional intelligence. Data generated from the study was entered into Excel spreadsheet, cleaned and coded. It was then exported into SPSS-IBM version 21 and analyzed using descriptive statistics (mean, standard error of mean, frequency, and percentage). Pearson’s product moment correlation method was used to study the association between self-esteem and emotional intelligence. Chi-square and Phi tests were further used to assess the strength of association between self-esteem and emotional intelligence (including the subscales). Student-t test was used to test gender differences on the variables. The statistical level of significance set at p ≤ 0.05.
3. Results
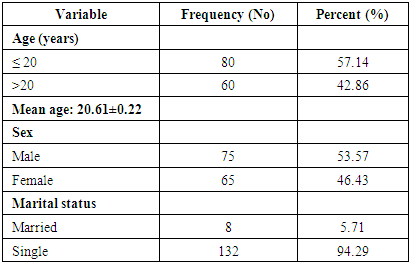
- According to Table 1 below, 75(54%) were males while 65(46%) were females. The mean age of the respondents was 20.61±0.22 years, range of 17-36 years and majority (57.14%) were 20 years or below. Ninety four percent (132) were single while 6% (8) were married.
|
|

|
|
|
4. Discussion
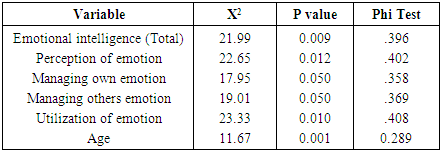
- Self-esteem and emotional intelligence are essential tools for effective and quality medical practice. Therefore, their perception and management are critical and pertinent ingredients for the successful career of a doctor and the future doctors. The patients, care givers, other members of the health team, stakeholders and health policy makers will ultimately prefer an emotionally intelligent doctor with high self-esteem. These also apply to a medical student with high self-esteem and emotionally intelligent. This study showed that the undergraduate medical students exhibited high levels of self-esteem, emotional intelligence and all the components of emotional intelligence. An emotionally intelligent doctor will better head and manage the healthcare team, perceive the needs of his/her patients, provide better healthcare, improve patient satisfaction [52-54]. Efficient and satisfactory performance in healthcare services brings joy and happiness to all stakeholders. Evidences abound that people of higher self-esteem perform better in the academic environment, at work places and more frequently achieve professional success [55-57]. Furthermore, emotional intelligence helps one build stronger relationships, succeed at work, and achieve career and personal goals [58, 59]. Persons with high emotional intelligence tend to have better social skills, are perceived as more pro-social and less prone to conflict, better physician-patient relationship, better patients’ trust and better patient outcomes [60-63]. Emotionally intelligent person is usually better equipped to deal with effects of stress and better adjusted than one with low emotional intelligence [8]. EI has also been associated with physician wellness, decreasing burnout and better motivation [58, 64]. In general, it has also been agreed that persons with a high level of EI tend to have more positive interpersonal behaviours befitting of the medical profession [65-68] and have more adaptive ways of coping [6, 25].Whereas positive emotional intelligence is a strong predictor of better psychological adjustment, negative or low emotional intelligence is significantly related to depression, harmful and distressing behavior [16]. Researches have also shown that sad mood can be attributed to low level of EI [17, 18].Self-esteem is another important tool for health care professionals during their interactions with patients, caregivers, other health care team members and even hospital management [42, 43]. Self-esteem affects both present and future physical and mental health and health-related behavior [47]. It has been demonstrated that an individual with a high self-esteem has a better level of mental health and self-harmony [33], feels more confident and more competent, exhibits optimistic attitudes [34-37], has strong personal strength and ability to solve problems and ability to control emotions [29]. Health care professionals with good self-esteem have the potentials to stimulate, influence and induce a positive well-being both in the health care team and in patients [45]. Conversely, low self-esteem is associated with desperation, inferiority, sadness, depression and high suicidal tendencies [34, 38-40]. This study found a strong and positive correlation between self-esteem and global emotional intelligence (r = 0.237, p = 0.001) (including all the components of EI, except utilization of emotion) among the medical students. This means, as they grow in self-esteem, they become more emotionally intelligent. A medical student imbibed with high self-esteem and at the same time, highly emotionally intelligent, is most likely going to be a good and functional medical practitioner. He/she will invariably be happy, confident, competent, a good team leader, liked by patients and other health team members, and also have good interpersonal behaviors, patient-physician relationship and patient outcomes [29, 5, 66-68].This research also indicated strong and positive correlation between age and self-esteem and emotional intelligence. That is, as the respondents get older, they become more emotionally intelligent (r = 0.240, p = 0.001) and develop high self-esteem (r = 0.177, p = 0.05). Probably, in agreement with the dictum “experience is the best teacher”, life experiences of the students increase with their age, and as they mature, they become sensitive to their own feelings and those of others. The positive correlation of age and emotional intelligences in this work agrees with earlier findings of McKinley, 2014; Faye et al, 2011; Weng et al, 2008 and Zeidner et al, 2013 [52, 54, 60, 69]. Our result also indicated that there is no significant gender difference in the assessment of self-esteem and emotional intelligence among the respondents. Koleoso et al, [47] have also found no significant difference between male and female students on self-esteem. This finding corroborates earlier studies which found no gender differences in self-esteem [70-74]. However, other studies have found significant gender differences in self-esteem, that males have high self-esteem than females [75-77]. In relation to EI, no significant gender differences among the students in this study. This finding agrees with the work done by Cakan and Altun [78] in which they found no significant gender difference. Conversely, other studies [17, 50, 85] have found significant gender differences and noted that males scored significantly higher on cognitive, physical and self aspect, while females scored higher on somatic symptoms, expression of affect and spiritual aspects. Furthermore, a study in South Africa [80], found that females compared to males, exhibited higher levels of understanding of emotions of other people while it was also buttressed in another study [5] that females had higher mean scores compared to males on impulse control and empathy.In conclusion, this study showed that the medical undergraduates had high levels of self-esteem and emotional intelligence. Self-esteem correlated positively and significantly with age, global emotional intelligence, perception of emotion, management of own emotion and management of others emotion. The association between self-esteem, age, global emotional intelligence and its components are strong and statistically significant (p< 0.05). Universities should consider including emotional intelligence and self-esteem tests among selection criteria in medical school enrollees.