-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Brain and Cognitive Sciences
p-ISSN: 2163-1840 e-ISSN: 2163-1867
2017; 6(2): 21-25
doi:10.5923/j.ijbcs.20170602.01

Neurolinguistic Analysis of a Case of Crossed Apraxia of Speech in Arabic
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMohamed Taiebine 1, Saadia Aidi 2, Maria Benabdeljlil 2, Mustapha El Alaoui Faris 2
1University Mohammed V. Faculty of Medecine and Pharmacy-Rabat, Morocco
2Department of Neurology A and Neuropsychology, Rabat Specialty Hospital, Souissi Quarter-Rabat, Morocco
Correspondence to: Mohamed Taiebine , University Mohammed V. Faculty of Medecine and Pharmacy-Rabat, Morocco.
| Email: |  |
Copyright © 2017 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Apraxia of speech (AOS) was studied in various occidental languages. However, no cases have been described in Arabic. In the current study, we present OJ who suffered from crossed apraxia of speech following right hemisphere damage. To our knowledge, until now there are merely three cases of crossed apraxia of speech (CAOS) that have been described in the literature. Therefore, our study will clarify the neurolinguistic symptoms that characterize CAOS and explore the phonetic encoding process. OJ 55-year old right-handed man with a right ischemic infarct on brain MRI. He was diagnosed as having a pure, severe CAOS with no aphasic impairment. He presented the classic triad of apraxia of speech: segmental distorsions, temporal variability errors and finally Suprasegmental distorsion which occurred inconsistently. The neurolinguistic pattern as shown in our patient errors resulted in a loss of phonetic encoding of both words and phrases. Therefore, our patient had (a) a quasi-preserved ability of phonological form of words that he intended to produce them, and (b) in the absence of paresis, ataxia, akinesia, or other problem related to motor control that would prevent the accurate execution of speech articulation.
Keywords: Arabic speech production, Crossed apraxia of speech, Phonetic encoding, Neurolinguistic analysis
Cite this paper: Mohamed Taiebine , Saadia Aidi , Maria Benabdeljlil , Mustapha El Alaoui Faris , Neurolinguistic Analysis of a Case of Crossed Apraxia of Speech in Arabic, International Journal of Brain and Cognitive Sciences, Vol. 6 No. 2, 2017, pp. 21-25. doi: 10.5923/j.ijbcs.20170602.01.
Article Outline
1. Introduction
- Acquired apraxia of speech (AOS) is traditionally viewed as a disorder of speech programming that results from loss or failure to access segmental movement plans, and/or the subsequent assembly of segments to form cohesive syllables. AOS is a disorder that occurs following lesion of the language-dominant hemisphere. The disorder may occur following damage to frontal motor association areas [1] or to parietal regions [2]. It is generally viewed as a disorder at the level of the interface between completed language encoding and the phonetic implementation of the message. AOS is seen as a disorder of motor planning and cannot be explained in terms of failures of primary sensorimotor systems [3, 4]. It is not infrequent and may occur as an isolated disorder or, more usually, in association with aphasia. Despite its frequency, AOS remains poorly understood and a relatively under-researched impairment.We report the fourth case in the literature of CAOS (See table 1), which may be interpreted as a disturbance at the level of the mental syllabary dedicated for phonetic encoding. Our case is interesting, because O.J. presents an impairment at the phonetic encoding process which appears to conform to the theoretical predictions made about phonetic distortions in the context of crossed apraxia of speech [5, 6] and dal-route speech-encoding model [7]. The present study focused on this particular finding in the Arabic speaking.
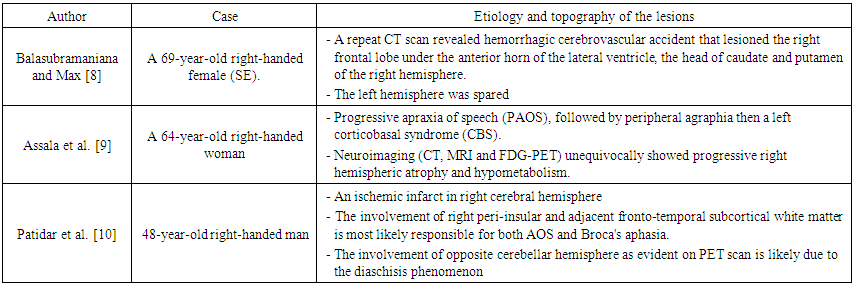 | Table 1. Effect of etiology and lesion topography in three reported cases of CAOS in the literature |
2. Case Report
- OJ 55 years old, right-handed (100%, Edinburgh Handedness Inventory), driver, married, with a high school background. He had an acute left hemiparesis with suspension of speech. The evolution was marked a few hours later by complete recovery of the motor deficit. The brain MRI shows a right peri-sylvian ischemic infartct (see Fig. 1).
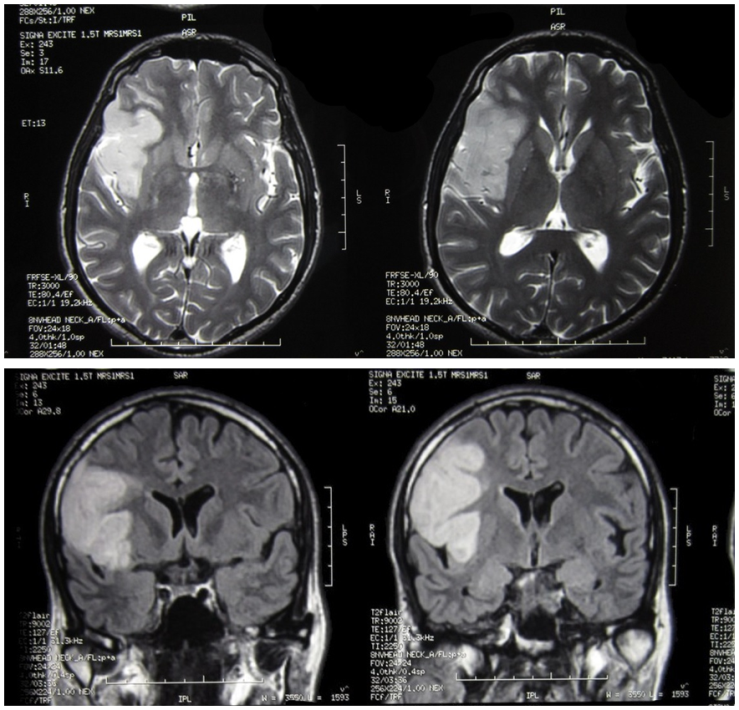 | Figure 1. Brain MRI in axial, T1 (with gadolinium) and T2 sequences |
2.1. Neurolinguistic Assessment
- The linguistic assessment was performed with the Moroccan version of MT86 which is the Protocole d’examen linguistique de l’aphasie [11]. The spontaneous speech is almost fluent, full of many phonetic and phonemic distortions. We noticed no agrammatism nor anomia. Repetition is better than the naming task, insofar as the phonetic and phonemic distortions are few. In the writing assessment, the different graphic transpositions in spontaneous writing, copying and dictation are successful. Reading comprehension is preserved. At the administration of the Moroccan Alexia-Agraphia Protocol [12] that consists of corpus of 113 words in Arabic and 20 non-words, the patient showed phonological alexia and agraphia. In writing words, he produced non-words and while he read non-words, he produced lexicalizations (See table 2). Neuropsychological assessment has not objectified acalculia, homonymous hemianopia or visuo-constructive apraxia. However, he had a left ideo-motor apraxia. The upper and lower face apraxia test [13] allowed objectifying a moderate bucco-lingual apraxia with the presence of left buccal and lingual hypotonia. Perceptual Evaluation of the patient's voice showed a monotonous voice with a slight bitonality without tremor. The intensity is decreased with rapid vocal termination (release). There is a loss of modulation in intensity. The tone of voice is rather hazy. A closed rhinolalia is observed (hyponasality). We find a significant alteration of prosody with fluctuations in speech rate. At the phonetic level, there is an inaccuracy in production of consonants and vowels in the absence of palilalia. The patient is unintelligible in spontaneous speech due to the phonetic and acoustic impairment.
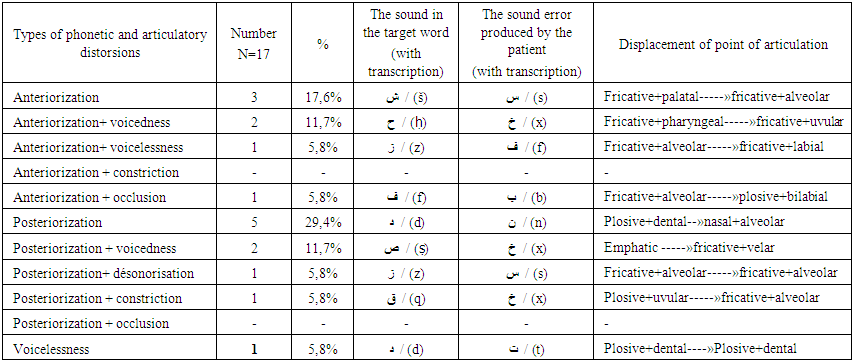 | Table 2. Type, number and percentage of articulatory distortions in J.O speech |
3. Discussion
- We report the fourth case in the literature of crossed apraxia of speech (CAOS) with selective damage to the phonetic encoding process, which the mean features as described by Ziegler [14]:-Segmental distorsions, -Temporal variability errors -Suprasegmental distorsion which occurred inconsistently. Furthermoure, the typology for CAOS contains the additional following features:-Prolongations of steady-state components of segments, and intersyllabic pauses [15].-Reduced coarticulation [6],-Initiation difficulties, as indicated by articulatory groping and struggle [16].The neurolinguistic pattern as shown in our patient errors resulted in a loss of phonetic encoding of both words and phrases. Therefore, our patient had (a) a quasi-preserved ability of phonological form of words that he intended to produce them, and (b) in the absence of paresis, ataxia, akinesia, or other problem related to motor control that would prevent the accurate execution of speech articulation. The issue is thus to transform the abstract representations of words into motor commands that guide the articulators parts of speech and program its position and the sequences of it as described by Darley et al [16].The cardinal signs of apraxia of speech are a dysfluency associated with phonetic and phonemic distortions. The presence of such symptoms indicates that the patient is struggling for the realization of a stable target word at the phonetic l level, and the fact that the symptoms are variable, is regarded as evidence in differential diagnosis in comparison with the most basic mechanisms within the motor speech framework such as dysarthria, paresis, ataxia, akinesia, dyskinesia / dystonia, etc.Our patient has at least a severe crossed apraxia of speech because he is able to pronounce syllables or single words or even short phrases. He produces both phonemic and phonetic errors. The phonological errors refer to substitutions, omissions or additions of phonemes. Another type of error is phonemic addition of consonant or consonant clusters, usually at the beginning of a word or syllable. The mechanism causing these errors has often been described as an articulatory or speech simplification. A dual-route model of speech encoding proposes that high-frequency units are stored as movement gestalts, and are not assembled afresh each time that they are used. In the model proposed by Levelt [17-19], high-frequency syllables are stored in a mental syllabary. Levelt suggests that, because the form is retrieved directly from storage and without mediating assembly from sub-syllabic processes, it will differ in phonetic characteristics from forms that do require greater recourse to sub-syllabic computational processes. The dual-route speech-encoding hypothesis is a potentially fruitful one for speech pathology in general and in re-evaluating the underlying impairment in disorders such as AOS in particular. Whiteside and Varley [20] reviewed the characteristics of AOS and proposed that the underlying impairment in the disorder might be reconceptualised as damage to direct-route speech encoding, and a subsequent reliance on indirect-route encoding (see Figure 2).
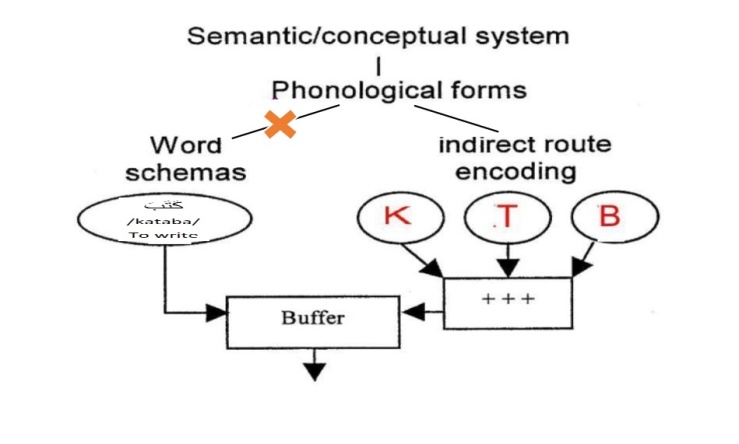 | Figure 2. Dual-route speech-encoding model. The hypothesized impairment of the direct route in CAOS is indicated by the cross on the route between phonological form and word schemas |
4. Conclusions
- We report the fourth case in the literature of crossed apraxia of speech (CAOS) with selective damage to the phonetic encoding process. Our case study confirms the hypothesis that apraxia of speech can occur after injury to the right hemisphere in right-handed individuals. OJ speech was characterized by a moderate to severe crossed apraxia of speech. This study also indicates the need for further clinical data of patients and analysis of production of motor components of speech due to lesions of the right hemisphere. It is important to develop cognitive models of speech production in Arabic and to clarify the role of the right hemisphere in regulating phonetic and verbo-encoding process at segmental and suprasegmental level.
ACKNOWLEDGEMENTS
- The authors are grateful to the patient who participated in this study.