-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Brain and Cognitive Sciences
p-ISSN: 2163-1840 e-ISSN: 2163-1867
2015; 4(1): 8-14
doi:10.5923/j.ijbcs.20150401.03
Performance in the Stroop Task and Simultaneously Recorded Heart Rate Variability before and after Meditation, Supine Rest and No - Intervention
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLPailoor Subramanya 1, Shirley Telles 2
1Indian Council of Medical Research, Center for Advanced Research in Yoga and Neurophysiology, SVYASA, Bengaluru, India
2Patanjali Research Foundation, Patanjali Yogpeeth, Haridwar, Uttarakhand, India
Correspondence to: Shirley Telles , Patanjali Research Foundation, Patanjali Yogpeeth, Haridwar, Uttarakhand, India.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
In an earlier study heart rate variability (HRV) recordings after cyclic meditation (CM) suggested a shift towards vagal dominance. In a separate study, CM improved the performance in a task for attention. Generally, attention tasks result in sympathetic activation. The present study was intended to assess whether CM would change the autonomic status when practitioners performed an attention task, with simultaneous HRV recording Methods: Twenty-five male volunteers with group average age ± S.D., 23.9 ± 5.0 years were each assessed on three separate days in three sessions, (i) CM, (ii) supine rest (S R), and (iii) quiet sitting (QS). Each session was for 23 minutes. Simultaneous assessments were made before and after each of the three sessions and included the HRV, respiratory rate and performance in the Stroop task. Results: Following CM the LF power increased and HF power decreased (P < 0.05). There was an increase in the word scores, color scores and color-word scores of the Stroop task (P < 0.001, Repeated measures ANOVA, followed by Bonferroni adjusted post-hoc analyses). Conclusion: The results suggest that there was reduced parasympathetic activity after CM and possibly increased sympathetic activity, when participants simultaneously performed the Stroop task. Their improved performance in the Stroop task suggests better response inhibition, interference resolution, word reading and activation along with reduced physiological arousal based on HF power of the HRV.
Keywords: Stroop, HRV, Yoga
Cite this paper: Pailoor Subramanya , Shirley Telles , Performance in the Stroop Task and Simultaneously Recorded Heart Rate Variability before and after Meditation, Supine Rest and No - Intervention, International Journal of Brain and Cognitive Sciences, Vol. 4 No. 1, 2015, pp. 8-14. doi: 10.5923/j.ijbcs.20150401.03.
1. Background
- Meditation has been described as a state of consciousness in which deep relaxation and increased internalized attention co-exist [1]. Meditation is not always easy for novices to practice, and in yoga texts meditation has been described as the seventh of eight stages required to reach ultimate mental transcendence, called Samadhi, in Sanskrit [2]. A meditation technique called CM, which has its’ origin in ancient yoga texts [3, 4], was derived especially for novices. CM has alternating cycles of practicing yoga postures slowly, with deep awareness, interspersed with periods of SR. CM differs from other meditation techniques as it includes the practice of yoga postures practiced slowly with heightened internal awareness. Tai-Chi-Qui-Gong is a comparable technique and these practices have been called ‘moving meditations’ [5].Despite the fact that CM includes the practice of yoga postures, following twenty-three minutes of the practice there was a reduction in heart rate, as well as in the low frequency power of the HRV, while the HF power increased, suggesting a shift in cardiac autonomic balance towards vagal dominance after the practice (Cohen’s d = 0.87) [6]. The LF band of the HRV is believed to be chiefly but not entirely related to sympathetic activity when expressed in normalized units [7], while efferent vagal activity mainly contributes to the HF band [8].Sympathetic activation is of interest in the present study since it is associated with increased vigilance and hence may be considered essential for performing an attentional task [9]. An early study showed improvement in different aspects of attention in practitioners of Transcendental Meditation [10].More recently studies on practitioners of CM have shown improved performance in tasks requiring attention and other executive functions. In forty-two experienced meditators the P300 was measured before and after a session of CM on one day, and similarly before and after a comparable duration of SR on another day (Cohen’s d = 0.85) [11]. The P300 is an event related potential which reflects fundamental cognitive events requiring attentional and immediate memory- processes [12]. Following CM there was a decrease in the P300 peak latency and an increase in the P300 peak amplitude suggesting a greater improvement in cognitive processes after CM compared to SR [11].Similarly the performance in a cancellation task was assessed in sixty-nine volunteers immediately before and after sessions of CM and SR on separate days [13]. Cancellation tasks assess attention, concentration, and visuo-spatial scanning abilities [14]. The net scores improved after both CM (by 24.9 percent) and SR (by 13.6 percent). These results also suggested that CM favorably impacts attention, concentration, visual scanning abilities and a repetitive motor response. It was speculated that the improvement in attention in these studies was related to a reduction in anxiety, as anxiety affects performance in tasks requiring attention [15].However, as already mentioned attention is generally associated with increased sympathetic activity [16], which normally decreases when anxiety levels are low [17]. The association between HRV and trait anxiety was assessed in 92 healthy persons along with self-rating of trait anxiety and perceived emotional stress [18]. In an earlier study on healthy participants there was a shift towards vagal dominance in the HRV after CM [6]. Till now, the HRV has not been recorded in meditators in the same session as the attention task. Hence the present study was designed to record the HRV and respiratory rate before and after the Stroop task, in the same session [19]. The hypothesis being tested was that CM would improve Stroop task performance while reducing sympathetic activity.
2. Methods
- ParticipantsThere were twenty-five self-reported healthy male participants with ages ranging between 18 and 38 years (group mean ± S.D., 23.9 ± 5.0 years). The participants did not report any history of hospitalization or medication in the past six months. The temperature and blood pressure of the subjects were normal on the days of their participation in the study. The sample size was not determined prior to designing the study. However post-hoc analyses based on the effect size showed that the power of the tests used was 0.95 [20]. Participants were staying at a residential yoga c enter located in south India. For inclusion in the study participants had to meet the following criteria: (i) they had to be healthy based on a standard medical examination, (ii) literate and able to understand and perform the Stroop task, and (iii) have adequate experience of both CM and relaxation while supine i.e., 3 to 6 months. Exclusion criteria included: (i) color blindness based on the Ishihara charts, (ii) consumption of caffeine, nicotine containing substance s or any medicine which could influence cognition or autonomic function, and (iii) presence of extra systoles in the EKG. Participants were recruited by flyers on the notice board of the institution. The method of the study was explained to the participants, but not the hypothesis. No incentive was given to the participants for participation in the study. None of the participants was involved in any other ongoing yoga research at the center.DesignEvery participant was assessed in three types of practice sessions (CM, S R and QS sessions). The assessments were made on three different days for every participant. The sequence of practice was randomly allocated to balance the effect of the order of the sessions. The study design was explained to the participants and their signed informed consent was obtained. The study had the approval of the institutional ethics committee.Time allocation within the sessionsThe Stroop task, HRV and respiratory rate were measured ‘before’ and ‘after’ the interventions. The first 5 minutes of the ‘before’ period was in the sitting position, followed by 23 minutes of the ‘d uring’ period, where participants were given (i) CM practice using taped instructions, or (ii) SR in the corpse posture (= shavasana, in Sanskrit) without instructions or (iii) in the QS session participants were seated at ease. This was followed by 5 minutes of the ‘after’ period. In (i) ‘d uring’ periods of S R and QS session and (ii) ‘before’ and ‘after’ periods of all 3 sessions the participants were not given any specific instructions. The study design and assessment schedule are given schematically in Figure 1.
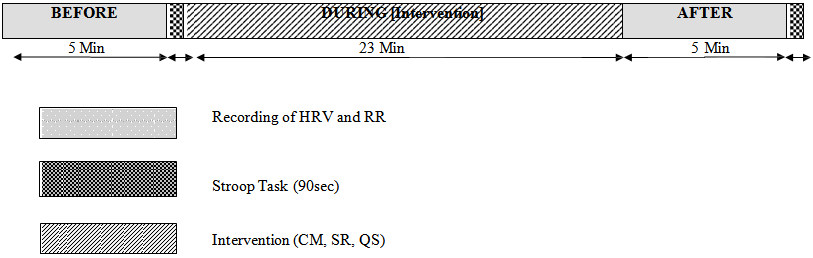 | Figure 1. Schematic representation of the design of the study and assessment schedule |
3. Results
- The group means and standard deviations for scores obtained in the HRV and respiratory rate are shown in Table 1, Stroop task [i.e., word task, color task, and color-word task scores] taken before and after CM, S R, and QS sessions are shown in Table 2.
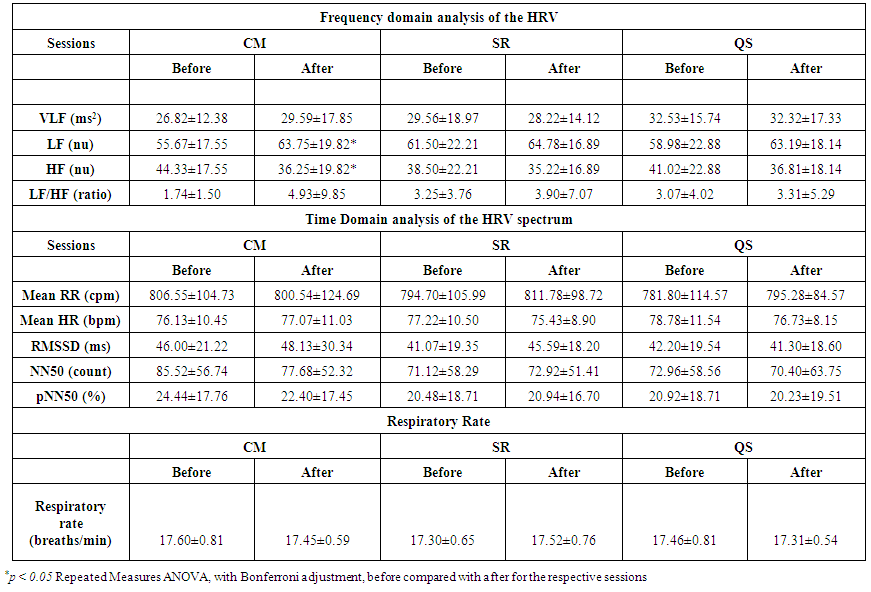 | Table 1. Group mean values ± S.D. of Frequency domain, Time domain analyses of the HRV and Respiratory rate recorded before and after, sessions of Cyclic Meditation (CM), Supine Rest (SR) and Quiet Sitting (QS) |
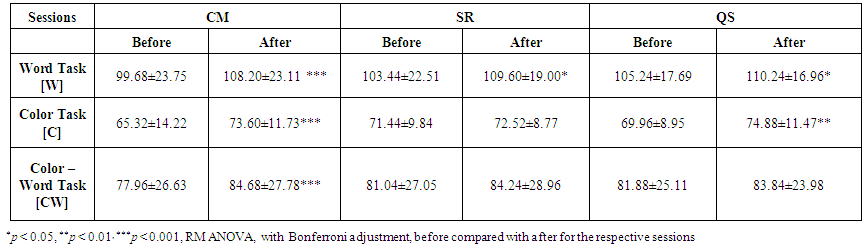 | Table 2. Group mean values ± S.D. for the Stroop Task recorded before and after sessions of Cyclic Meditation (CM), Supine Rest (SR), and Quiet Sitting (QS) |
4. Discussion
- Participants performed better in the Stroop task with increased color-word scores after CM but not after SR or QS. However the better performance was accompanied by an increased power in the LF component of the HRV, with a decrease in the HF component.As already mentioned in the introduction the LF band of the HRV is believed to be chiefly but not exclusively due to sympathetic activity when expressed in normalized units [7], while efferent vagal activity contributes mainly to the HF band of the HRV [8]. The breath rate did not change after either of the interventions. This is relevant as it is known that there is an acute increase in LF, total spectrum HRV and in vagal baroreflex gain during slow breathing [24]. Training to increase the amplitude of respiratory sinus arrhythmia maximally increases the amplitude of heart rate oscillations at approximately 0.1 Hz [25]. However, considering that breath rate did not change in the present study, the breath frequency could not have influ enced the HRV. Hence the results suggest that after CM there was a shift in the autonomic balance towards parasympathetic decrease with a possible increase in sympathetic activity. As was already mentioned sympathetic activation is associated with increased vigilance considered necessary to perform an attentional task [6].In an earlier study the LF band of the HRV reduced after CM, while the HF power increased [6]. However there were the following differences between that study and the present one: (i) in the earlier study participants were asked to practice CM and SR on two different days and the HRV and respiration were recorded. They were not given any task. In the present study participants were given the Stroop task to perform before and after the prac tice of CM or SR or QS, and the HRV and the respiration were recorded after the task. Hence, the earlier studies assessed practitioners of CM when they were doing the meditation without any task. The present results suggest that when given a task the physiologically relaxing effects of CM were not sufficient to reduce the sympathetic arousal associated with vigilance and performance of a task requiring attention in addition to other cognitive processes.The absence of change in time domain measures which generally reflect parasympathetic tone, may be explained as follows: the sympathovagal balance is tonically and phasically modulated by at least three main factors, (i) central neural integration, (ii) peripheral inhibitory reflex mechanisms, and (iii) peripheral excitatory reflex mechanisms [26, 27]. While, variable phenomena such as the heart rate (recorded as the HRV) can be described as a function of time they may be better described as the sum of elementary oscillatory components [28]. Hence, the frequency domain may reflect those changes in the sympathovagal balance which are not detected by time domain analysis.The S troop task requires the participant to suppress a habitual response and respond to an unusual one, in this case naming the color of the ink in which incongruously named color-words were printed [29]. The cognitive processes required to perform the Stroop task are complex. They include response inhibition, interference resolution, behavioral conflict resolution, word reading and production, and visual attention [30]. The present results suggest a possible benefit of practicing CM to improve abilities required to perform the Stroop task. Participants did not have any additional benefit of reduced sympathetic activation after performing CM and while doing the Stroop task. These results resemble those of a recent study in which Vipassana expert meditators showed greater P3b amplitudes to the target tones after meditation than they did both before meditation and after the no- meditation sessio n. They also simultaneously showed a larger LF/HF ratio during Vipassana meditation [31]. Hence Vipassana meditation was associated with better P3 potentials (suggestive of improved attention) along with increased sympathetic activity.The limitations of the study are as follows: (i) in earlier studies [13, 32] the tasks used to assess performance before and after CM were different from the Stroop task used in the present study. The reason for this difference is that the participants in the present study had taken part in other studies in the residential yoga institution which used the tasks which were previously assessed. Hence, they would have approached the earlier tasks with a certain degree of familiarity and monotony. However in introducing a new task the results of the previous studies cannot be directly compared with the present results. (ii) All twenty- five participants were assessed in three types of sessions. Even though the order of the sessions was randomized the participants might have performed better after CM not merely because of the effects of CM per se, but because the CM session kept them busy and engaged while the other sessions did not. (iii) The sample size (n=25) in the present study was smaller than the sample sizes in the previous studies o n cancellation task performance (n=47), memory task performance (n=57) and HRV and respiration (n=47).Despite these limitations the present results showed that when participants were given a task to perform following meditation, their perfor mance in the task which required focused attention was better, however there was also a shift in the autonomic balance towards decreased parasympathetic activity and possibly increased sympathetic activity.
ACKNOWLEDGEMENTS
- The authors gratefully acknowledge the funding from the Department of Science and Technology (DS T), Government of India, as part of a grant (Project No. SR/CSI/22/2009) under Cognitive Science Research Initiative (CSI). The authors also acknowledge H.R. Nagendra P h.D. who derived the Cyclic Meditation technique from an ancient yoga text and Naveen K.V., P h.D., Co-P.I. of the project for his suggestions at different stages.