-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Brain and Cognitive Sciences
p-ISSN: 2163-1840 e-ISSN: 2163-1867
2012; 1(4): 26-29
doi: 10.5923/j.ijbcs.20120104.01
A Case Report: Using Augmentative and Alternative Communication to Teach a Preschool Student with Autism to Respond and Request Appropriately
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-Text HTML
Full-Text HTMLBrianna Armstrong 1, T. F. McLaughlin 2, Alison Clark 3, Jennifer Neyman 4
1Department of Special Education, Gonzaga University, East 502 Boone Avenue, Spokane, WA, 99258-0025, USA
2Department of Special Education, Gonzaga University, 99258-0025,USA
3West Valley School District#363, Millwood Early Childhood Education Center, 8818 East Grace Avenue, Spokane, WA 99212, USA
4East 502 Boone Avenue, Spokane, WA, 99258-0025, USA
Correspondence to: T. F. McLaughlin , Department of Special Education, Gonzaga University, 99258-0025,USA.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
The purpose of this study was to evaluate the effectiveness of augmentative and alternative communication (AAC), specifically a Flip n’ Talk, with a preschool child thought to be on the autism spectrum. The ability to functionally request assistance and respond appropriately within a daily routine was the focus for this study. A multiple baseline design was employed to evaluate the intervention. The results of this study indicated that the Flip n’ Talk (i.e. AAC) was an effective way to teach functional communication to our participant.
Keywords: Autism, Augmentative and Alternative Communication, ACC, Flip’n Talk, Pre School, ASSIST Program, Developmental Delays, Single Case Research Design, pre-schooler
Cite this paper: Brianna Armstrong , T. F. McLaughlin , Alison Clark , Jennifer Neyman , "A Case Report: Using Augmentative and Alternative Communication to Teach a Preschool Student with Autism to Respond and Request Appropriately", International Journal of Brain and Cognitive Sciences, Vol. 1 No. 4, 2012, pp. 26-29. doi: 10.5923/j.ijbcs.20120104.01.
Article Outline
1. Introduction
- Roughly 9 in 1,000 (0.9%) American children were identified as being on the autism spectrum in 2006[1, 2]. The symptoms of autism include significant difficulties in social interaction, delayed or abnormal functioning in verbal and nonverbal communication, and unusual patterns of behavior[2]. All disorders on the autism spectrum are characterized by communication impairments of some type, although the specific symptoms vary widely[3]. Beukelman and Mirenda[4] indicated that about 50% of people with autism never develop sufficient speech as a means for communication” Simply put, these individuals lack meaningful speech. What is most striking about the language of children with ASD is that many do not talk. Even by the time they reach adulthood, many have minimal or no spoken language[5]. Despite the wide range of language issues that children with ASD display, these children are usually very strong visual learners. Communication between individuals occurs constantly. It is difficult to be successful in life and experience close relationships without communication. Non-speech vocalizations and gestures often mean nothing in particular to others because they can refer to anything. The inability to communicate normally may lead to the development and persistence of nonconventional forms of manding[5]. One major limitation of gestures is that they can refer to only things that are physically present (i.e., things that can be pointed toward, looked at or touched[6]. Whereas verbal communication allows us to give or receive information about needs (e.g. request objects or peer interaction), desires, perceptions, knowledge, or affective states. The inability to communicate has a dramatic impact on an individual’s ability to control many aspects of life[6]. Therefore, it is extremely important to provide individuals whom have language problems with a way to interact with others and successfully communicate in a socially appropriate way [6-9].Alternative and augmentative communication (AAC) devices aim to supplement or replace an individual’s natural speech and/or handwriting through aided or unaided communication approaches[7]. AAC has been reviewed and described as a promising intervention for language in ASD because it alleviates at least some of the confusion, anxiety, and frustration that many individuals with ASDs experience when they encounter unexpected events[4-5]. This is due to the fact that individuals with autism are strong visual learners and most AAC devices rely heavily on symbols. The symbols used have a direct correspondence with a specific referent. It is said that approximately 14-25% of children diagnosed with an ASD rely on AAC to meet their daily communication needs[7]. The use of these devices may be either temporary or permanent. The purpose of this study was to evaluate the effectiveness of augmentative and alternative communication, specifically a Flip ‘n Talk, on a preschool student who was diagnosed as developmentally delayed and thought to be on the autism spectrum. An additional goal of this study was to increase the student’s ability to functionally request assistance and/or respond appropriately within a daily routine. Finally, we wanted to determine if this could be carried out in a functioning preschool public school classroom as part of the first author’s training and as documentation for meeting both state and national standards demonstrating the ability to modify student behavior.
2. Method
2.1. Participant and Setting
- The participant was a three-year-old female preschooler. Her parents came from a native Marshall Island, and spoke very little English, if any at all. The student’s eligibility category was Developmentally Delayed. By the end of data collection, she was officially diagnosed with Autism Spectrum Disorders (ASD) by a local pediatrician. The student was chosen for this study because she was almost completely nonverbal at the time of the study. However, she was extremely cooperative and attentive during the study.The study took place in a special education ASSIST (Autism: School Support for Inclusion and Systematic Teaching) preschool classroom in Washington State. The ASSIST room focused on individualized Discrete Trial Training with seven students under the age of six all of which were either diagnosed with ASD or thought to be on the spectrum by the school psychologist or classroom teacher. The basic model of the classroom follows evidence-based procedures for young students with autism[2, 5, 7-9]. The study took place between 10:30am and 11:30am every Monday through Thursday at a workstation located in a corner of the room. The workstation contained a large Rifton chair and desk. This was done and desk which fostered a focused environment. During the time of the study, there was anywhere from zero to three other students and at least two adults in the classroom. Overall the classroom was quiet with few distractions. The study was conducted by first author who was completing her special education student teaching for an endorsement in special education from the State of Washington and Gonzaga University[11].
2.2. Materials
- A variety of materials were used to conduct this study. The main materials needed were data collection sheets and a Flip n’ Talk with icons specific to the participant. These icons included: Help, All Done, More, and Yes. Other materials used were items that would best help teach the use of the Flip n’ Talk (e.g. food items, toys, and jars with lids).
2.3. Dependent Variables and Measurement
- The dependent variable for this study was the number of correct requests the participant made using the Flip n’ Talk. Requests also included the need for assistance (“help”), wants (“more”), and being finished (“all done”). A correct response was defined as the participant appropriately using the Flip n’ Talk by pointing to a specific icon. A single subject multiple baseline design[12] was used to evaluate the efficacy of the Flip n Talk. First baseline data were taken for each set. Then the AAC was introduced using Discrete Trial Training with each specific icon.
2.4. Baseline
- During baseline, the participant was observed at her workstation. Baseline consisted of the presentation of items (e.g. a jar with a lid, food, etc.). The participant was expected to request something (e.g. help, more, or all done) within five seconds, or the request was marked as incorrect. Correct and incorrect responses were marked on the data collection sheet. No feedback or praise was given to the student during baseline. Baseline lasted for 1 session in Set 1 and continued periodically for the other sets until all previous sets had been mastered.
2.5. AAC to Request Assistance
- An AAC device, the Flip n’ Talk, was chosen as the intervention. The Flip n’ Talk allows nonverbal children to have a mode of communication. Each day, during the work session, the participant was introduced to an icon (i.e. requesting icons - help, more, all done) on the Flip n’ Talk and taught how to appropriately use them via Discrete Trial Training. This skill was practiced 10 times per session.
2.6. Reliability
- Reliability of measurement was taken by the classroom teacher (third author) and the second author. A “+” was recorded for a correct performance of requesting anything desired or needed. Interobserver reliability or agreement was conducted four times during intervention. The percent of interobserver agreement was calculated by dividing the number of agreements by the number of agreements plus disagreements and then multiplying by one hundred. The percent of interobserver agreement was 100%.
3. Results
- Results for the number of requests successfully made during baseline and intervention across four sets can be seen in Figure 1
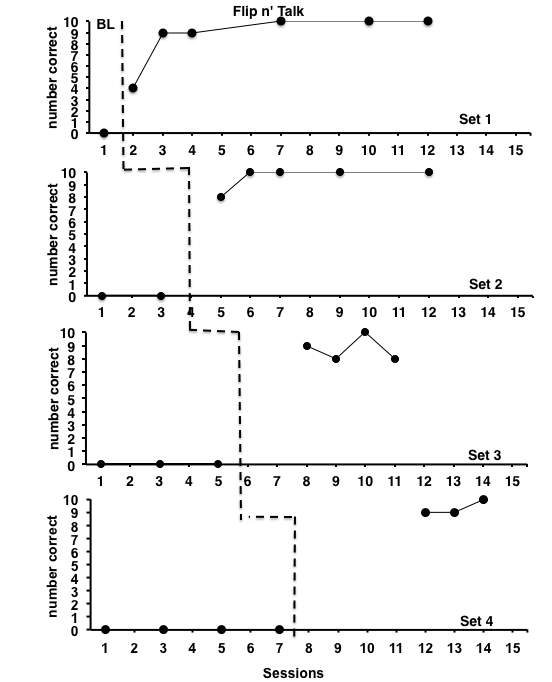 | Figure 1. The number of correct requests for assistance during baseline and Flip n’ Talk |
3.1. Baseline
- The data to the left of the dotted line shows the participants number of correct requests out of ten opportunities prior to the implementation of the AAC. During baseline for all 4 sets, the participant had zero attempts to request any sort of assistance. Therefore, the decision was made to immediately start intervention.
3.2. AAC to Request Assistance
- With intervention, the participant’s requests for “help” (i.e. Set 1) increased from 0% to 90% within 3 sessions and remained high throughout the rest of the study. For Set 2 (i.e. requesting to be “All Done”) a dramatic increase was observed with a mastery of 100% reached and maintained for 4 sessions. For Set 3 (i.e. requesting “more”), the participant increased from 0% to an average of 87.5%. On Set 4 (i.e. “yes”), she averaged 93.3% mastery during intervention. Results for all sets demonstrate a mastery of the skill.
4. Discussion
- The Flip n’ Talk paired with discrete trial training[10] had a positive impact on the participant. The increase in requests made directly correlated with the implementation of an AAC. The data shows a huge increase in number of requests made across all sessions while the Flip n’ Talk was used. The mastery of these requests will allow the child to more easily and efficiently communicate with adults and peers. She will also have more of her needs met. The case study had many strengths and weaknesses. Discrete Trial Training allowed for frequent examples, repetition, and structure and the Flip n’ Talk was a simple and effective communication tool. Previous research employing AAC was replicated with this project. Another strength was that the participant seemed to enjoy the one on one time with the researcher. She was always eager to come to work. However, the student was periodically absent. This caused the intervention to proceed slowly at times and require more review than necessary. In the end, the data never fell below 80% accuracy; therefore the strengths outweighed the weaknesses. In the future, the researcher would continue the study, implementing more sets that include more than requesting icons so the participant could expand her use of the Flip n’ Talk and communicate frequently. The researcher left the communication device with the lead teacher to provide an opportunity to continue practicing the use of the AAC with the participant. The researchers found the method to be effective at improving communication of wants and needs. Therefore, the researchers would use an AAC, more specifically the Flip n’ Talk, again with students that are non-verbal.
ACKNOWLEDGEMENTS
- This research was completed in partial fulfillment for the Degree in Special Education from Gonzaga University and the State of Washington. The first author would like to thank the participant for her cooperation during the study, as well as the cooperating teacher for her assistance during the study. Portions of these data were presented at the Spokane Intercollegiate Research Conference and at the Gonzaga University Symposium on Service Learning in April 2012. Requests for reprints should be addressed to T. F. McLaughlin, Department of Special Education, Gonzaga University, Spokane, WA 99258-0025 or via email at bri_armstrong@yahoo.com or mclaughlin@gonzaga.edu