-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Applied Sociology
p-ISSN: 2169-9704 e-ISSN: 2169-9739
2021; 11(1): 1-10
doi:10.5923/j.ijas.20211101.01
Received: Feb. 23, 2021; Accepted: Mar. 20, 2021; Published: Mar. 28, 2021

Effects of COVID-19 Restrictions on Social and Psychological Behaviours in South Korea
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML1MBA Graduate Class of 2017, Graduate School of Business, Seoul National University, Republic of Korea
2M.Com., MPA (Master of Professional Accounting) Graduate Class of 2009, University of Sydney Business School, Sydney NSW, Australia
Correspondence to: Seunghoon Lee, MBA Graduate Class of 2017, Graduate School of Business, Seoul National University, Republic of Korea.
| Email: |  |
Copyright © 2021 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Research objectives: This study aimed to assess the effects of Covid-19 restrictions on social and psychological behaviour change on long-term and short-term disease spread. The key research objectives included determining how South Koreans perceived and acted in response to threats of exposure to Covid-19 infections, investigating the the downstream effects of intergroup relations and risk perception. Methodology: In this quantitative survey, participants from in South Korea were approached through social media and invited to take part in an online survey. The questions were framed to reflect the non-pharmaceutical measures that the South Korean government put into place, such as restricted movements, closure of schools and public campaigns to institute social distancing and behaviour change. Up to 1021 participants took part in the study. Setting and location: Republic of Korea. Conclusion: South Korean restrictive measures restricted individuals’ freedoms by encouraging the adoption of coping behaviours that positively contributed to extensive health benefits with respect to curtailing the spread of the virus. In this way, the restrictive measures reduced the rapidity and prevalence of an epidemic. Findings also suggest that restrictive measures have a positive relationship with collective efficacy behaviours. Therefore, measures of social restrictions also influenced people to pursue long-term collective interest in consideration of the greater good of the society, rather than short-term self-interest in consideration of individuals’ interests. However, restrictive measures are found to lead to cooperative behaviours only in circumstances where there is either effective communication of fear or higher perception of risk. Therefore, restrictive measures put forth by the South Korean government seem to have aligned wirg individual and collective interests by causing fear and contributing to higher risk perception.
Keywords: Covid-19, Covid-19 restrictions, South Korean restrictions, Risk avoidance coping behaviours, Cooperative behaviours
Cite this paper: Seunghoon Lee, Effects of COVID-19 Restrictions on Social and Psychological Behaviours in South Korea, International Journal of Applied Sociology, Vol. 11 No. 1, 2021, pp. 1-10. doi: 10.5923/j.ijas.20211101.01.
Article Outline
1. Introduction
- In December 2019, a novel acute respiratory syndrome coronavirus 2 (SARS-CoV-2 or Covid-19) broke out in Wuhan, China (Prem, Liu, Russel, Kucharski, Eggo & Davise, 2020). Over time, the intensification of Covid-19 infections fundamentally shaped societal behaviours (Bellato 2020; You, 2020). Being a trans-boundary epidemic, Covid-19 pandemic has had far-reaching effects on human behaviours. Many of the effects cannot be restricted to changes in social behaviours or roles within any specific national boundary (Bavel, Baicker & Willer, 2020; Tabernero, Castillo-Mayen, Luquo, & Cuadrado, 2020; Weston, Ip & Amlôt, 2020). Across public health research published in 2020, there are convincing indications that the Covid-19 pandemic substantially affected societies globally, triggering considerable investment in behaviour control measures by governments (Weible, Nohrstedt, Cairney, Carter, Crow, Durnová, & Stone, 2020; Zhang, Jia, Lei, Wang, Zhao, & Guo, 2020).The very first case of Covid-18 infection in South Korea was recorded on January 20, 2020. Exactly 30 days later, the first death from the infection was reported. A surge in infections over time – to at least 10,591 as of April 15, 2020 – forced the government to evaluate and update its policies to prompt behaviour changes that could help curtail the spread of the virus (Prem et al., 2020). The very first case of Covid-18 infection in South Korea was recorded on January 20, 2020. A surge in infections over time – to at least 3,000 by March and to 10,591 as of April 15, 2020 – forced the government to evaluate and update its policies to prompt behaviour changes that could help curtail the spread of the virus (Dighe, Cattarinpo & Riley, 2020; Prem et al., 2020). Incidentally, South Korea had the highest rates of infections globally, second only to China. Such emerging realities forced the South Korean government to describe and make public its response through a report dubbed “Tackling Covid-19: Health, Quarantine, and Economic Measures of South Korea.” The report pointed out the government’s multifaceted approach to the pandemic, such as the implementation of a walk-through screening stations, drive-through screening centers, community treatment centers, and self-diagnosis application (Prem et al., 2020).After recording an acute rise in COVID-19 infections in April 2020, the South Korean government amended its policies to speedily control transmissions. It also put into force less rigorous nationwide social distancing measures (Dighe et al., 2020). This has led to substantial interest in their “test, trace, isolate” strategy, which brought the transmissions under total control owing to its pervasive effects on social behaviours and roles (Dighe et al., 2020).However, there is a clear dearth of research on the effects of both coercive and non-coercive effects of social restrictions during the Covid-19 pandemic on human behaviours (Dighe et al., 2020; Prem et al., 2020). Therefore, the attempt to model the relationship between human behaviours during the pandemic and the spread of Covid-19 virus remains a topic of significant interest.The aim of this study was to assess the effects of Covid-19 restriction on social and psychological behaviours and their effects on long-term and short-term disease spread. Correspondingly, this study investigated the effects of restrictive measures on the epidemic dynamics, with focus on the effectiveness of restrictive measures set up by the South Korean government in response to Covid-19 epidemic.The key research objectives included determining how South Koreans perceived and acted in response to threats and risk of exposure to Covid-19 pandemic, and investigating the downstream effects of intergroup relations and risk perception. The study also sought to examine how targeting fears with restrictive measures can be significant during the Covid-19 pandemic.
2. Literature Review
- To curtail local transmissions, South Korean government introduced non-pharmaceutical measures like restricted movements, closure of schools and public campaigns to cause changes in social behaviours (Bellato 2020). Such measures reduced the number of new confirmed cases and delayed a peak of the virulent disease. Critically, the restrictive measures had far-reaching effects on social behaviour change. Already, a number of mathematical modelling and simulation researches have attempted to predict the dynamics of emergent diseases (Zhang et al., 2020). In their study, Kucharski, Russel, Diamonds, Liu, Edmunds, Funk (2020) used stochastic modeling of data collected from Wuhan, China, and indicated that the median daily reproduction number fell to 1.05 from 2.35 after the introduction of travel restrictions (Kucharski et al., 2020). They found that Covid-19 transmissions significantly declined in Wuhan due to travel control measures. In a related study, Prem et al. (2020) investigated the effects of measures like closure of schools or distancing at workplaces, which in turn indicated the positive effects of social distancing on reducing the rapidity and prevalence of an epidemic. Of particular concern in their study was the materialization of physical social distancing measure, like closure of workplaces and schools and social distancing in Wuhan. Prem et al. (2020) found that such restrictive measures reduced the effects of Covid-19 outbreak in Wuhan. The measures also significantly altered age-specific mixing patterns in the population in preceding outbreak response measure for virulent diseases. While travel restrictions indisputably played a crucial role in curtailing the spread of the infections beyond Wuhan and contributed to a delay in the onset of outbreaks across Asia (Prem et al., 2020).A related study by Kim, Kim and Jung (2020) also found that social distancing and social behaviour change measures are essential for curtailing the spread of Covid-19, even though such measures may not necessarily eliminate the disease. Their research findings indicated that highly vulnerable people should be vigilant regarding the likelihood of reoccurrence of the epidemic. They should as well uphold a high degree of personal hygiene. At the same time, governments should come up with policies that reinforce social distancing to alleviate the second wave of this epidemic (Kim et al., 2020). Kim et al. (2020) found social distancing to have been effective in curtailing the spread of Covid-19 pandemic when pharmaceutical interventions were not available. In which case, proactive partaking of the general public and pertinent policy measures could curtail the spread of viral infections. In their study, Paradya et al. (2020) examined the factors that changed travel behaviours in the onset of Covid-19 infections in Japan, with respect to calls for voluntary restriction of movements. They mainly focused on the contributions of social influence and risk perception. Paradya et al. (2020) performed a panel web-survey of residents of the Kanto Region, particularly Tokyo Metropolis. Besides discussing the observable patterns in behavioral shifts, they modelled behavioural changes of four non-work-related activities. These include leisure, shopping, grocery shopping, and eating out. As regards leisure and eating out, the researchers differentiated between going out in groups and individually. From observing the distributions of leisure and eating, regression models of “going-out” frequency were carried out for shopping. On the other hand, a discrete choice approach was used for “leisure” and “eating-out,” which indicated significantly smaller frequencies. In the end, Paradya et al. (2020) found that the perception of degree of self-restriction of others, as a measure of social influence was related to a moderate reduction of shopping frequencies. Conversely, there was a moderate increase in “going-out self-restriction probability for eating-out and leisure activities.” Paradya et al. (2020) also observed an association between risk perception of the virus and “higher probabilities of going-out self-restriction for eating-out and leisure.” Paradya et al. (2020) concluded that less restrictive policy measures like campaigns for encouraging reduced levels of non-essential travel could effectively express the seriousness of threats brought about by Covid-19 and mechanisms for coping.Fischer, Avrashi, Oz, Fadul, and Gutman (2020) also investigated challenges to human behaviour during the Covid-19 pandemic. In effect, to curb virus infections, governments implemented a number of restrictive emergency regulations, whereby people were asked to assume constraining behaviours, like working from home, staying at home, avoiding unrestricted physical interaction with highly vulnerable persons like the elderly, using hand sanitizers regularly, and washing hands frequently (Fischer et al., 2020). While such behaviours restricted individuals’ freedoms, they contributed to significant health benefits in terms of curbing the spread of the virus. Fischer et al. (2020) explain that the measures to limit or avoid physical contact with vulnerable persons, such as the elderly or individuals with compromised immune system triggered restrictive behaviours that prevented hospitals from being overwhelmed with admissions, flattened the infection curve, and delayed the peaks of the infections. Yet, their study also indicated that likely interactions among people who may have been affected and those who were free from the infection led to social dilemma, particularly among members of a family. Unawareness of others’ status and inevitability of certain interactions at home also helped to violate the restrictions (Bellato 2020). They study found that people’s behaviours were only a fraction of the difficulties that hindered the implementation of restrictive measures by the government. Among other difficulties included the type of interventions and whether such interventions were capable of facilitating cooperative behaviours in populations by enabling them to develop positive perceptions and attitudes towards the restrictive measures. From their findings, Fischer et al. (2020) discussed that the restrictive measures set up to curtail the spread of Covid-19 should not be coerced as well as be perceived as interfering with people’s free will, otherwise it may trigger widespread protests. In which case, interventions put in place should be able to assess risk perceptions and health attitudes of affected populations, recognise their weak points, and provide a variety of behavioural tools that are capable of inducing compliance with health-promoting regulations (Bavel et al., 2020). The mitigation measures for Covid-19, such as self-isolation, quarantine, and social distancing were implemented globally. While a majority of people complied with the requirements of these measures, there were a number of incidences of breach (Buonomo & Marca, 2020). In the UK, local authorities had to continually monitor adherence to mitigation measures. Fundamentally, human behaviours were primarily shaped by costs that those affected by the pandemic control measures paid with respect to health, such as psychological pressures, diminished social interaction, increased pressures, and health risks associated with significant damage to the wellbeing of human population (Buonomo & Marca, 2020). Accordingly, the attempt to model the relationship between human behaviours during the pandemic and the spread of Covid-19 virus remains a topic of significant interest.A research by Tabernero et al. (2020) examined some of the practical guidance generated by the World Health Organization and identifies some of the practical measures that countries had tended to adopt as having focused on normative behaviours, depending on social isolation and lockdown, and social isolation. Other measures concentrated on individuals’ self-protection behaviours such as washing hands and wearing masks. Globally, the measures instituted by governments led to social dilemma. Such scenarios of social dilemma were examined in a study by Kollock (1998), which investigated collective behaviours and individual behaviours in the event of scarcity of resources during a pandemic. Kollock (1998) discussed that in social dilemma individuals may often use selfish strategies to amass more resources. Another study on events of uncertainty, such as during Ebola pandemic, observed that seeking for risk-information and risk perception are important variables that may assist in the adoption of coping behaviours in the face of susceptibility to a disease (Kahlor, 2010). Overall, risk perception was linked with the pursuit for related subjective norms. In turn, perception leads individuals to constantly search for information on the pandemic in order to adopt pertinent risk avoidance behaviours. Consequently, individuals with risk information seeking behaviours are likely to develop coping behaviours (Hubner and Hovick, 2020). Self-efficacy beliefs have also been found to predict human behaviours (Bandura, 1997). When it comes to pandemic scenarios whereby focus has to be placed on the public to encourage self-care behaviours, then variables like self-care self-efficacy beliefs become of particular interest (Callaghan, 2015). The concept of self-care self-efficacy refers to the self-assurance that an individual demonstrates in his capacity to carry out relevant self-care activities (Mak et al., 2009). Therefore, self-care self-efficacy is linked to the extent to which individuals – particularly patients or highly vulnerable populations – have the confidence to comply with the norms or interventionist measures (Buonomo & Marca, 2020; Tabernero et al., 2020). In pandemic scenarios, self-care self-efficacy are basically self-management linked to the degree to which individuals have the confidence to comply with the norms or interventionist measures set up in health policy directives (Tabernero et al., 2020).Similarly, when it comes to collective behaviour, trust in fellow members of a population is emphasised, along with the collective efficacy in complying the rules need to curb or curtail the spread of a virus. Studies have found collective efficacy to be related to community safety during pandemics (Sampson, 2009). Fong and Chang (2011) established the significance of collective efficacy in ensuring the safety of vulnerable populations during the severe acute respiratory syndrome (SARS) pandemic in 2003. Their study established that trustful cooperative or community actions associated with the degree of collective efficacy. In turn, the degree of collective efficacy can be measured by examining the level of trust in cooperative actions intended to cause coping behaviours during a pandemic (Tabernero et al., 2020; Weston et al., 2020).
3. Methodology
- In this quantitative survey, a correlational research design was used to evaluate the link between variables such as self-care efficacy and collective efficacy, and self-care efficacy and risk perception using statistical data. A correlational research design helped to determine trends of behaviours in relation to restrictive measures put up by the government during the Covid-19 pandemic, rather than the cause and effects of behaviours.A snowball sampling method was used, as Facebook users in South Korea were asked to invite their friends to take part in the research. This was necessary for hidden populations that were difficult to access during the Covid-19 pandemic. As enough participants invited their friend to take part in the study, a positive feedback loop led to a self-sustaining study that witnessed a rapidly growing sample size. Participants from in South Korea were approached through Facebook, and requested to take part in a small survey. The participants were asked to click on a sponsored link, which directed them to SurveyMonkey, an online survey development website. They were asked to share the link online to their Friends in South Korea. The link directed the participants to a short questionnaire that was expected to take at least 8 minutes. To measure participants’ behaviour and attitudes in light of the restrictions that accompanied Covid-19 pandemic, participants were asked to answer two sets of questions that relate to health regulations. The questions were framed to reflect the non-pharmaceutical measures that the South Korean government put into place, such as restricted movements, closure of schools, and public campaigns to institute social distancing and behaviour change.Coding of the questions was then performed and results entered into a statistical system package called PASW Statistics 18 for data analysis. Overall, 1021 questionnaires were received, despite the target sample being 1300, giving in a response rate· of 78.5%. The questionnaire was designed in keeping with the reviewed literature to acquire information required to answer the research questions. To develop variable measurement scales, the reviewed literature also provide information to adapt the variables to the research problems.The survey comprised 20 items, whereby 16 were put on a 4-point Likert scale to determine from participants their views on the effects of restrictive measures on human behaviours during the period of the Covid-19 pandemic. The remaining four items were designed to collect demographic data like gender, age, and job status. The sample was made up of 42% (n=429) women and 58% (n-592) men. In addition, 63% (n=643) of the participants were in the age range 18-50 years, while 37% (n=378) of the participants were aged 51 years and beyond.To test the survey instruments used in this research, its reliability measures had to be constructed. For this research, Chronbach's Alpha test of reliability was used to establish the internal reliability of the scaled variables. Overall, a score of 0.916 was generated (see Table 1). Guttman Split-half Reliability Coefficient Statistic was as well applied as a reliability measure purposely to confirm the consistency of the scale items. It made it possible to compare the items in the first and second half of the scale. A value of 0.814 was generated. This indicated that the instrument is strongly reliable.
4. Hypothesis Development
- Instrument validity tests were carried out to test two hypotheses that were developed in line with the research problem. The two were afterwards tested using Gamma distribution, specifically ChiSquare. Gamma distribution was needed for this research to model continuous variables like restrictive measures and self-care efficacy, collective efficacy, and risk perception, which were expected to remain positive, yet demonstrate skewed distributions. Gamma was needed for this research, because wait time between events was relevant.Hypothesis 1 (HI): Restrictive measures have a positive relationship with self-care self-efficacy.Hypothesis 2 (H2): Restrictive measures have a positive relationship with collective efficacy behaviours.Hypothesis 3 (H3): Restrictive measures lead to improved coping and cooperative behaviours when there is effective government communication of fear and higher risk perception.Hypothesis 4 (H4): It was also hypothesised that restrictive measures tend to be more effective in vulnerable social groups due to their higher risk perception.Independent and Dependent VariablesTo determine the effects of demographic factors on the role of restrictive measures in shaping people’s behaviours during the pandemic, variables like health status, age, level of education, and gender were positively analysed in relation to dependent variables. It was also necessary to identify single survey items that had the potential to affect participants’ perspectives on the perceived effects of restrictive measures on human behaviours. The independent variables were mainly restrictive emergency regulations, such as closure of schools, wearing masks, social distancing at workplaces, travel restrictions, working from home, and staying at home. The dependent variables included risk avoidance behaviours (such as self-efficacy, and collective efficacy), coping behaviours, and cooperative behaviours.
5. Results
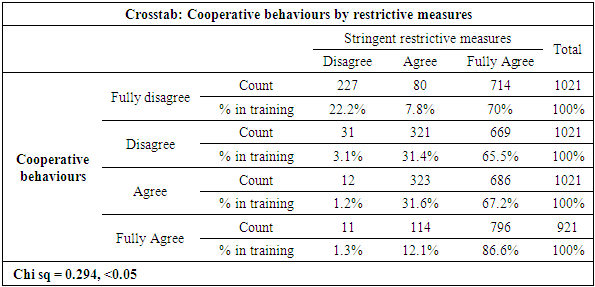
- It had been hypothesised that restrictive measures have a positive relationship with self-efficacy (H1). Table 1, on improved self-efficacy behaviours (SEB) as a result of restrictive measures (RM), demonstrates a fairly strong Gamma score of 0.294. It is also significant statistically at p < .05, for the first hypothesis.
|

|
|
|
|
|
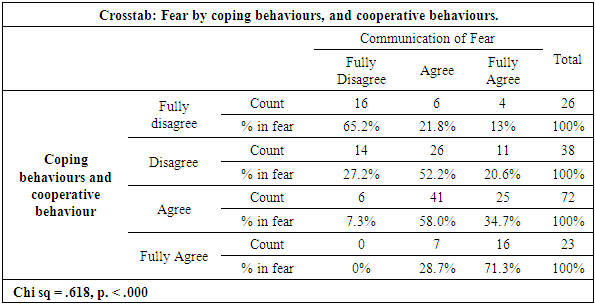
6. Discussion
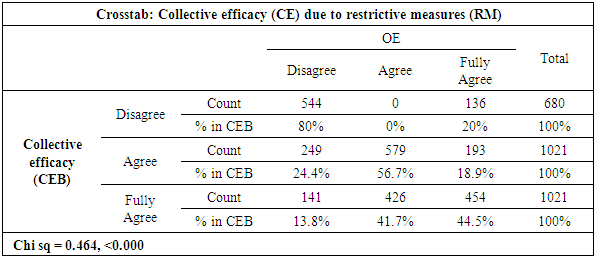
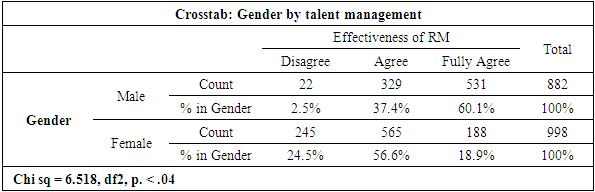
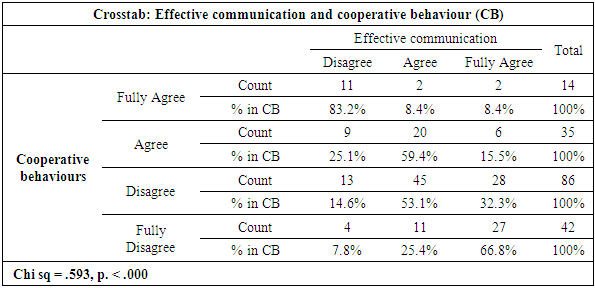
- All the proposed research hypotheses were confirmed. With respect to H1, findings suggest that restrictive measures have a positive relationship with self-care self-efficacy. Regarding H2, it is established that restrictive measures have a positive relationship with collective efficacy behaviours. When it comes to H3, restrictive measures are found to only lead to cooperative behaviours when there is effective communication of fear and higher risk perception. As regards H4, it is found that restrictive measures also tend to be more effective in vulnerable social groups like the elderly, women, and individuals with underlying health conditions because of their higher risk perception.For this reason, the research objectives were sufficiently met with respect to determining how South Koreans perceived and acted in response to threats and risk of exposure to Covid-19 pandemic, and the downstream effects of intergroup relations and risk perception. It can also be understood how targeting fears with restrictive measures can be significant during the Covid-19 pandemic, by leading individuals to change their behaviours if they feel they can deal with the threat, or whether it led to defensive reactions whenever they felt they were helpless to act.With respect to self-efficacy behaviours, results indicate a strong significant statistical relationship between restrictive measures and self-efficacy behaviours. Towards this end, people who positively viewed restrictive measures are likely to engage in self-efficacy behaviours. This appeared to be particularly the case for self-restriction from non-essential travels. This finding can be drawn to demonstrate the relationship between risk perception of Coronavirus and higher likelihoods of self-restriction for non-essential travels. In which case, restrictive policy measures can be interpreted to have reduced the extent to which people engaged in non-essential travels, although this seemed to depend on the severity of the threats that came with Coronovirus and coping mechanisms.On the relevance of collective efficacy, it is established that here is also a strong significant statistical relationship between restrictive measures collective efficacy. This indicates that people who positively viewed restrictive measures and complied with the measures are likely to adopt collective efficacy behaviours. For instance, people who were mainly exposed to negative emotional warnings on going to crowded places tended to experience more negative emotions toward Covid-19 restrictions and crowded places. In effect, such people may have spent a great deal of their time internalizing the warnings and recalling risks of infections and death, with the consequent effects on risk perception and complying with the restrictions. In effect, increased negative emotions influenced more people to depend on negative information regarding the virulent disease in comparison to other information in making decisions. Therefore, restrictive measures put forth by the South Korean government seem to have aligned individual and collective interests. Measures of social restrictions encouraged people to adopt and internalize collective interests and guidelines. This influenced people to develop the drive to behave in ways that the society considered right in light of Covid-19 control protocols, and to avoid behaviours considered to be wrong. In which case, restrict measures that encouraged cooperation and morality encouraged the adoption of prosocial behaviours. This appeared to be the case as individuals’ behaviours in the society are often regulated by shared norms and moral values, so that those who do what is considered to be right earn positive recognition and veneration, while those who do not are condemned (Bavel et al., 2020). For instance, social distancing led to changes in behaviours as regard how the participants went out. They stopped going out in groups and started to go out individually.Therefore, it appears that measures of social restrictions also influenced people to pursue long-term collective interest in consideration of the greater good of the society, rather than short-term self-interest in consideration of individuals’ interests. In effect, the fight against the global epidemic called for extensive cooperation. Yet, a major challenge to cooperation included calling upon individuals to carry individual costs with focus on ensuring long-term benefit for each one. In reality, there was a clear divergence between individuals’ short-term self-interests and long-term collective interests of the larger society. Additionally, Covid-19 pandemic exposed a number of collective groups that had to act together to curtail the spread of the virus. These included families, communities, nations, and international community. For this reason, since the South Korean government expected people to place their priorities on individual and local interests, restrictive measures were necessary to encourage cooperation with the view of ensuring the attainment of long-term global interests. These indicate that restrictive measures increase cooperative behaviour among populations that are vulnerable to virulent infections during a pandemic. Additionally, such individuals are expected to cooperate when they believe that others are cooperating or adhering to restrictive measures. For that reason, interventions that are anchored in descriptive norms are likely to effectively increase cooperative behaviour among vulnerable populations.Regarding the effects of demographic factors like gender, age, educational level and health status, a number of findings are also made. When it comes to gender, female participants were more likely to develop appropriate positive coping behaviours compared to their male counterparts. Analysis of restrictive measures by health status show that people who considered themselves to be generally healthy failed were less likely to comply with restrictive measures compared to those who were less healthy and more vulnerable to infections. This indicates that healthier individuals are more likely to demonstrate optimism bias, which studies have showed can in turn expose them to more infections. Analysis of age by restrictive measures also indicates that elderly people who are more vulnerable to Covid-19 infections due to their reduced immunity are more likely to develop coping behaviours compared to their younger participants.Another compelling finding is that less restrictive measures are more likely to elicit cooperative behaviours. This implies that appropriate cooperative behaviours depend on the lower the degree of the strictness of restrictive measures. However, this may depend on the quality of communication from the government. Effective communication from the government was found to influence the adoption of cooperative behaviours. Covid-10 restrictive measures triggered cooperative behaviours, which assuaged panic. The measures stopped people from acting blindly and disproportionately out of the need to ensure self-preservation, which had a potential to endanger the survival of others. Rather than act selfishly with the view of ensuring self-preservation due to panic, the measures brought order, necessitated cooperation, and influenced general adoption of norm-governed behaviours. Indeed, studies have showed tendencies of people to exhibit altruistic behaviours during disasters or emergencies (Bavel et al., 2020). Such altruistic behaviours can be prevented using interventions that enabled mutual cooperation among vulnerable populations (Bavel et al., 2020).In reality, the quality of information remains a significant factor, particularly the extent to which fear is communicated to the public. This study found that fear contributes to the efficiency of restrictive measures, as there is a significant relationship between the higher frequency of fear and restrictive measures. Findings in this research indicate that strong fear appeals lead to positive behaviour change whenever individuals perceive a sense of efficacy. Strong fear appeals with low-efficacy messages leads to greater levels of defensive reactions. Yet, a likely challenge is that individuals may tend to demonstrate optimism bias, which refers to a strong belief that harm may only befall others but not self. Although research has showed that optimism bias may contribute to avoidance of negative emotions, it can lead to scenarios whereby individuals misjudge their potential to contract an infection. The effects of risk perception on risk avoidance behaviours were also examined in this research. The particular risk avoidance behaviours that appealed to this research include self-efficacy, and collective efficacy. It is found that risk perception influenced the participants’ tendency to adopt risk avoidance behaviours. The perception of the level of self-restriction by other members of a population was found to be related to a reduction in the frequency of going out in groups. Risk avoidance behaviours are related to perceptions of the costs and benefits of particular safety choices for both an individual and the society. Restrictive measures drove emotions that triggered risk perceptions. In turn emotional responses to risky situations seemed to have influenced people’s thinking in two ways. The quality of the emotions seemed to have influenced the participants to internalize congruent information. The quality of emotions refers to whether an emotion is positive or negative. For instance, people may have tended to have a negative feeling about going to public placed depending on the negative information that accompanied restrictive measures associated with social distancing. Yet, such information guided people’s judgment of the costs and benefits of restrictive measures.
7. Conclusions
- Restrictive measures encouraged the adoption of coping behaviours that positively contributed to extensive health benefits with respect to curtailing the spread of the virus. As established, restrictive measures have a positive relationship with self-care self-efficacy. Findings also suggest that restrictive measures have a positive relationship with collective efficacy behaviours. Therefore, measures of social restrictions also influenced people to pursue long-term collective interest in consideration of the greater good of the society, rather than short-term self-interest in consideration of individuals’ interests. Restrictive measures are also found as tending to be more effective in vulnerable social groups like the elderly, women, and individuals with underlying health conditions because of their higher risk perception. However, restrictive measures are found to lead to cooperative behaviours only in circumstances when there is effective communication of fear and higher risk perception. Therefore, restrictive measures put forth by the South Korean government seem to have coincided with individual and collective interests by causing fear and triggering higher risk perception. The more vulnerable groups in the society, such as the elderly, women, or the sickly people are also found to be more willing to develop appropriate positive coping behaviours than their corresponding counterparts. This is linked to their higher frequencies of fear and higher risk perception.Restrictive measures should be less restrictive to provide people with more freedoms to perceive the costs and benefits of restrictive measures. Indeed, less restrictive measures are more likely to elicit cooperative behaviours. This implies that appropriate cooperative behaviours depend on the lower the degree of the strictness of restrictive measures. However, this depends on the quality of communication from the government. Communicating fear leads to positive behaviour change whenever individuals perceive a sense of efficacy. In addition, non-pharmacological interventions that are restrictive in nature should be able to bring about a balance between preventing optimism bias without bringing about disproportionate fear and anxiety.
8. Research Implications
- The findings in this research have varied practical implications on the implementation of restrictive measures that can enable the public to assume constraining behaviours that can curb the spread of a virus during an outbreak. Of particular relevance is the importance of targeting fears with restrictive measures to influence members of the public to change their behaviours and to trigger defensive reactions. Focus should be placed on implementing restrictive measures that can increase cooperative behaviour, risk avoidance behaviours, and coping strategies among populations that are vulnerable to virulent infections during a pandemic. These could curtail the spread of Covid-19 pandemic when pharmaceutical interventions are not available.Findings in this research can further be drawn to demonstrate the relationship between risk perception of Coronavirus and higher likelihoods of self-restriction for non-essential travels. Under such circumstances, policymakers could interprete restrictive policy measures as having reduced the extent to which people engaged in non-essential travels. However, this should be understood as dependent on the severity of the threats that came with a virulent disease and associated coping mechanisms.Restrictive measures are found to have far-reaching effects in terms of contributing to social behaviour change. Therefore, to curtail local transmissions, policymakers should set up less restrictive non-pharmaceutical measures like restricted movements, closure of schools and public campaigns to institute social distancing and behaviour change to reduce the number of new confirmed cases and to delay the peaking of the virulent disease.