-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Applied Psychology
p-ISSN: 2168-5010 e-ISSN: 2168-5029
2018; 8(1): 1-5
doi:10.5923/j.ijap.20180801.01

Evaluation of Reproductive Health Training Programs of Physicians via Assessing Their Knowledge in Egypt: A Comparative Study
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML1Department of Psychology, School of Humanities and Social Sciences, The American University in Cairo, Cairo, Egypt
2Department of Statistics, Faculty of Economics and Political Science, Cairo University, Giza, Egypt
3Social Research Center of the American University in Cairo, Cairo, Egypt
Correspondence to: Hassan H. M. Zaky , Department of Psychology, School of Humanities and Social Sciences, The American University in Cairo, Cairo, Egypt.
| Email: |  |
Copyright © 2018 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

An essential component of quality of reproductive health (RH) care, which has often been overlooked in the Egyptian literature, is the physicians’ knowledge. This study attempts to assess the RH knowledge of physicians working under two different primary health care (PHC) settings and compare them with a control group of RH physicians working in the regular primary health care units. The first setting belonged to the health sector reform (HSR) program that Egypt attempts to scale-up while the second came from a special RH intervention initiative conducted by an NGO (ESPSRH) in Egypt. Two tools were developed to test physicians’ RH knowledge in the three groups of PHC clinics. A questionnaire was designed to test several aspects of RH knowledge and an in-depth interview schedule was used to collect detailed information from the physicians. Despite the fact that the three groups received training courses but with varying degrees of content and frequency, their learning level was low. None of the training settings had a significant influence on the physicians learning levels of RH knowledge unlike the situations in other countries. Findings clearly indicated that the training of the HSR group of physicians was lagging in various components of RH. However, since HSR program in Egypt is an irreversible route and to guarantee technical RH quality of care, all its theoretical training components of RH should be revised very carefully. It is expected that the amount of training time given to RH needs to be expanded. It is recommended that officials continuously conduct pre and post assessment of knowledge and analyze results to identify weak points in its training programs. Physicians need more frequent training as well as to attend weekly seminars to keep them up to date. HSR needs to be more aware of RH goals and becomes an effective advocate for these goals. It is recommended that HSR RH training programs be more area specific to emphasize local challenges in addition to general challenges facing Egypt. HSR needs to have a demographic eye and emphasizes family planning efforts within its other instruments.
Keywords: Reproductive health, Interventions, Physicians' knowledge, Training evaluation, Egypt
Cite this paper: Hassan H. M. Zaky , Evaluation of Reproductive Health Training Programs of Physicians via Assessing Their Knowledge in Egypt: A Comparative Study, International Journal of Applied Psychology, Vol. 8 No. 1, 2018, pp. 1-5. doi: 10.5923/j.ijap.20180801.01.
Article Outline
1. Introduction
- In the evaluation of reproductive health (RH) services in Egypt, researchers have mainly focused on the client’s views, organization characteristics, and characteristics of the physician-beneficiary satisfaction and responsiveness (Huntington et al. 2010; Papp et al. 2014; Zaky et al. 2007 and 2010). An essential component of quality of reproductive health care, which has often been overlooked in the literature, is the physicians’ knowledge (Becker et al. 2007; Valadez et al. 1997). Egypt has recently completed its RH strategy in 2015 with a main objective of providing quality services to beneficiaries. Since the late 1990s, there has been several attempts to provide good quality RH services at the primary health care level in Egypt. These earlier initiatives included, among other components, a training component to train physicians to raise their RH knowledge. One attempt was within the health sector reform program (HSR) implemented by the Ministry of Health and Population (MOHP) in several governorates in Egypt during the 2000s (Huntington et al. 2010). Another initiative was the RH intervention conducted by the Egyptian Society for Population Studies and Reproductive Health (ESPSRH) in some MOHP clinics in two governorates in mid 2000s (Zaky et al. 2007 and 2010). The focus of this study is to assess the RH knowledge of physicians working under these two settings and compare them with a control group of RH physicians working in the regular MOHP PHC clinics outside these two interventions. This assessment is carried out to ultimately assist MOHP to support the RH component in its current efforts to improve RH services especially the training component. Although the need for assessing the knowledge is important, little is known in this field in the Egyptian literature of assessment of RH knowledge among physicians. This study attempts to fill this literature gap. This study tests the learning process of the physicians’ theoretical training, which is the second of the four levels of evaluating training programs according to Kirkpatrick and Kirkpatrick (2006).RH theoretical training within the ESPSRH intervention was carried out in an intensive twelve-day course. The theoretical training covered the concept of reproductive health, skills of simple diagnosis and treatment/referral of common gynecological and obstetric conditions, socio-cultural aspects of medical care, and communication and the importance of listening. Family planning was emphasized as an integrated component of RH services (Farag et al., 2002). Neither the HSR group nor the control group of physicians had specific RH training. RH training at the HSR clinics was part of the training of the basic benefit package (BBP) provided. RH training did not exceed 3 days, some broad concepts and skills were introduced. The control group did not receive any specific RH training programs. As part of the population vertical programs at MOHP, all physicians in the study received programs focused on specific issues related to Egypt’s population problem such family planning and the use of contraceptives.
2. Methods
- Two tools were developed to test physicians’ RH knowledge in the three groups of PHC clinics. First, a questionnaire was designed to test several aspects of RH knowledge. The questionnaire included twenty five multiple-choice questions and two problem solving questions. The questions were intended to test the following:a) Knowledge of definitions of RH and reproductive morbidity,b) Systematic approach to examination and diagnosis,c) Knowledge in diagnosis and treatment of common gynecological problems and referral criteria,d) Knowledge in management of normal pregnancy and criteria for high risk cases, ande) Knowledge in contraindications of contraceptive methods and management of associated problems.This questionnaire was self administered where physicians of each governorate were gathered in geographical groups and answered the questions under the supervision of several fieldworkers and a public health specialist. The form took on average 45 minutes to complete. Second, a specially designed in-depth interview schedule was used to collect detailed information from the physicians. The interview schedule included closed-ended questions about background, medical education and training, and work experience. Opened-ended questions aiming at understanding physicians’ perceptions regarding women’s RH problems, health seeking behavior, and the socio-economic context of RH were included. Furthermore, questions aimed at exploring physicians’ views regarding the rights entitled to clients, the quality and the completeness of RH services, and suggestions for improving unit performance and service utilization were incorporated in the in-depth interview.These two tools were developed using the knowledge, learning skills and core competencies adopted in both the integrated and the self-standing models of teaching sexual and reproductive health to physicians working at the primary health care. The literature about these models are available in Haslegrave and Olatunbosun (2003) and the World Health Organization (2011). All physicians trained through the RH intervention of ESPSRH in the governorates of Giza and Qalyoubia, and those trained in the context of HSR in Menoufia and Alexandria were included (29 and 31 physicians respectively). In the control group, 56 physicians, drawn from all health districts where the other two groups came from, were randomly selected.
3. Results
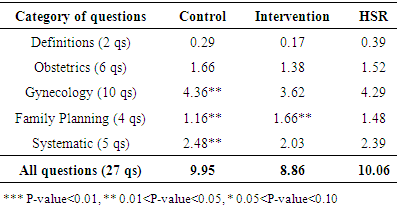
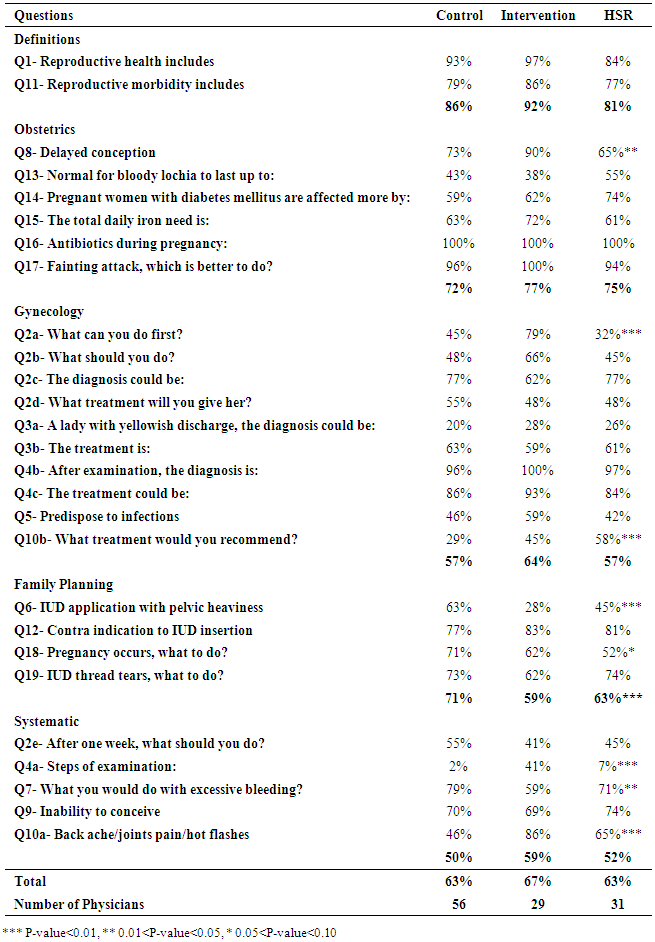
- The demographic characteristics of the three groups of physicians were very similar. The median age of physicians ranged between 40-45 years. The majority in all groups were married and had between 1 to 3 children with median 2 children. The proportions of physicians in the three study groups who had graduate studies after medical school were 59 percent, 33 percent, and 55 percent for the HSR, the intervention, and the control groups respectively. Out of those who have acquired graduate degrees, 86 percent of the intervention group studied gynecology, 43 percent of the control group studied maternal and child healthcare (MCH), while in the HSR group physicians received their graduate degrees in different medical fields, e.g. public health, gynecology, pediatrics, tropical and internal medicine. The results of the in-depth interviews showed that a larger percentage of physicians -one-third- in the ESPSRH intervention group mentioned health conditions specific to women in answer to a general question about health problems in the served communities, compared to one fifth in the other groups. These conditions included reproductive tract infections (RTIs), post-partum problems, lack of knowledge of contraceptive methods, and repeated pregnancies. When asked about women’s health problems encountered in practice, RTIs were reported by a large proportion of each of the three groups, with an even larger proportion of the ESPSRH intervention group of physicians (81 percent). Prolapse of genital organs was also mentioned by the three groups with a slightly higher percentage for the intervention group. A greater proportion of the HSR group (31 percent) mentioned anemia as a health condition frequently affecting women, and more of the HSR group also mentioned infertility. As for the control group, they had the largest proportions of those mentioning bleeding and frequent pregnancies (31 percent). Small proportions of all groups mentioned problems with contraceptive methods. Problems with sexual relationships were mentioned by few of the ESPSRH intervention and HSR groups of physicians, while only some of the physicians in the ESPSRH intervention group related urinary tract infections to women’s health problems. Few of both the HSR and control groups mentioned tumors of the genital tract, and some of the control group mentioned delayed pregnancy and abortion.Three-quarters of the intervention physicians thought that women in rural areas lacked health awareness compared to one-half of the HSR and control groups. Almost 60 percent of the ESPSRH intervention physicians reached this conclusion after talking with women. When asked about other factors that may affect the health status of women and their health-seeking behavior, physicians in all study groups pointed out different socio-economic factors. The first factor mentioned by a great majority of physicians was poor economic status, followed by traditions and customs such as influence of mothers-in-law on younger women, early marriage, and having many children. In addition, physicians mentioned illiteracy and ignorance regarding sound nutritional and sanitary habits among important factors affecting women’s health. All these factors were mentioned by larger proportions of physicians in the intervention group 74 percent) than those in the other two groups. Physicians also emphasized the impact of environmental problems such as garbage and sewage disposal on health. Physicians responded unanimously positively regarding entitlement of clients to certain rights. The control physicians clearly stressed on the importance of provision of good medical service, i.e. good medical examination and sound treatment. ESPSRH Intervention and HSR groups reported the right of clients to courteous treatment and securing privacy and confidentiality as important as good medical services if not more important. At least 50 percent of both groups confirmed the rights of respect and privacy. Giving the client sufficient time for the encounter with the physician came third for both the HSR and intervention groups (more than 15 percent). The right to have the diagnosis and treatment explained was also mentioned by some physicians in all groups, especially the HSR (14 percent) and intervention (10 percent) groups of physicians. The right to file a complaint was mentioned by some of the physicians in the control and ESPSRH intervention groups (8 and 5 percent respectively). Surprisingly, HSR physicians failed to mention this right.Table 1 shows the mean of incorrect answers for the five categories in the questionnaire. The lower the mean the higher is the percentage of correct answers. The means of incorrect answers were around 9 out of 27 questions. The likelihood of getting the answer wrong was almost one-third regardless of the group. No significant differences were observed among the three groups, with the exception of the FP group of questions. When comparing each two groups together, we found no significant differences between the control and HSR groups of physicians and between the ESPSRH intervention and HSR groups of physicians. Some significance was only detected between the control and intervention groups. The FP knowledge was slightly better among the control group but the Intervention physicians were more able to answer gynecology and systematic questions better, as shown in Table 1.
|
|
4. Discussion and Concluding Remarks
- Despite the fact that the three groups received training courses but with varying degrees of content and frequency, their learning level was low. None of the training settings had a significant influence on the physicians learning levels of RH knowledge unlike the situations in other countries such as Turkey (Ozek et al., 2003) and Lithuania (Jaruseviciene, 2003; Jaruseviciene et al. 2013).Findings clearly indicated that the training of the HSR group of physicians was lagging in various components of RH. However, since HSR program in Egypt is an irreversible route and to guarantee technical RH quality of care, all theoretical training components of RH should be revised very carefully, especially those of the HSR program. It is expected that the amount of training time given to RH needs to be expanded. It is recommended that MOHP continuously conduct pre and post assessment of knowledge and analyze results to identify weak points in its training programs. Physicians need more frequent training as well as to attend weekly seminars to keep them up to date. HSR needs to be more aware of RH goals and becomes an effective advocate for these goals. RH training within HSR should reflect this approach. There were some indications that ESPSRH physicians were slightly more aware of the RH problems in their served areas, probably because of its context focus. It is recommended that HSR RH training programs be more area specific to emphasize local challenges in addition to general challenges facing Egypt. Findings indicated that the training of ESPSRH emphasized the systematic approach of treating beneficiaries which is a strong point needed to support the HSR program. Findings also showed that the control group of physicians showed higher percent of correct answers within the family planning section. This is probably due to the stress of MOHP through its vertical programs on family planning as a key factor when dealing with the country's population challenges (Berman and Bossert, 2000). This is another area HSR needs to support as a horizontal program when it tackles all health challenges facing Egypt to have a demographic eye rather than diluting family planning efforts within its other instruments. Another aspect that is usually missed in the literature of reproductive health in Egypt is that the lack of RH knowledge among physicians may have negative psychological effects on beneficiaries as shown in various studies such as British Medical Association (BMA) Science and Education (2011). Empirical evidence is emerging on the psychosocial, and physical costs of not meeting the needs of beneficiaries in general and RH beneficiaries in particular, and on the positive psychological effects of changing the way and the environment in which the care is provided. Positive results will be gained if the service is offered in a positive environment and vice versa. Providing the right service will definitely add to the well-being of the woman seeking RH services. At the same time, missing the need of this woman via lack of knowledge among physicians will certainly have adverse psychological effects as well as demographic implications.
ACKNOWLEDGMENTS
- This research article is a product of the Project titled “Reproductive Health Interventions in Egypt: An Assessment Study, Phase 1” funded by the FORD foundation and is part of the activities of the Reproductive Health Working Group. The study was implemented by the Egyptian Society for Population Studies and Reproductive Health (ESPSRH) chaired by Hind A.S. Khattab, Ph.D. Hassan H.M. Zaky, Ph.D. was the P.I. of the Project. The author wishes to express his special thanks to the Ministry of Health and Population for their full cooperation, to FORD foundation for their generous support, and to Drs. Hind Khattab and Dina Galal for their valuable assistance to produce this article.