-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Applied Psychology
p-ISSN: 2168-5010 e-ISSN: 2168-5029
2016; 6(1): 10-14
doi:10.5923/j.ijap.20160601.02

Translation, Adaptation and Beginnings of Validation of the Multidimensional Health Locus of Control Scale Form C in a Sample of Type 2 Diabetes Adult Patients in Puerto Rico
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMiglany E. Gomila Romero1, José R. Rodríguez Gómez1, Rosa J. Rodríguez Benítez2
1Clinical Psychology Program (PhD), Carlos Albizu University, San Juan, Puerto Rico
2College of Social Sciences, University of Puerto Rico-Río Piedras Campus, San Juan, Puerto Rico
Correspondence to: Miglany E. Gomila Romero, Clinical Psychology Program (PhD), Carlos Albizu University, San Juan, Puerto Rico.
| Email: |  |
Copyright © 2016 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Faced with the challenges of managing Type 2 Diabetes in Puerto Rico, a common pathology with serious health consequences, this research aimed to generated knowledge through the translation, adaptation and validation of the Multidimentional Health Locus of Control Scale Form-C (MHLCSF-C). Morowatisharifaba, Mazloomy Mahmoodabad, Baghianimoghadam, Rouhani Tonekaboni (2009) defined the Health Locus of Control concept as a widespread expectation about whether one's health is controlled by the behavior itself or by forces external to one. This concept applied to the diagnosis of Diabetes mellitus has an important role in the management skills of these patients. And, in part, may explain the type of behavior that the patient adheres to. Similarly, it can have an impact in the establishment of medical interventions. Beyond a causal perspective, the purpose of the association of Locus of Control with Diabetes fulfills a psychosocial function within the strictly biomedical science that usually circumscribes the treatment of this disease. A pilot study with 108 Puerto Rican adults with type 2 diabetes was performed in order to test psychometrics properties of the MHLCSF-C with this population. It is expected to obtain an Alpha cronbach of >.70 or higher, that according to Kline (2000) will be adequate. The data collection phase was conducted online using the platform PsychData, and through social networks (Facebook and Twitter) where a link was placed to gather participants. The psychometric properties revealed that based on the items that met biserial correlation index (RBIs) of .30 or more and after psychometric analyses (factor and biserial analysis) from 18 items a total of 7 items remained. We obtained adequacy of the sample provided by Kaiser-Meyer-Olkin (KMO = .791), which showed that the sample size (N = 108) was adequate. Principal Component Analysis with Varimax type rotation revealed that factor loading appeared in two components. Component 1 obtained a value corresponding to 3.31 Eigen explaining the variance in 40.19%. This component was named Responsibility and Behavior. Component 2 obtained a corresponding value Eigen to 1.55 explaining the variance in 22.26%. This component was called Self-monitoring. Reliability analysis for the 7 items with which concluded the scale showed that the instrument obtained an internal consistency of Cronbach's alpha .79. A direct and statistically significant moderate correlation (r = .436, p <.01) between the two factors was obtained. However, although there is a relationship, it appears to be not significant enough to eliminate one or the other. Similarly, the original authors of the English instrument indicate that the subscales are orthogonal to each other and therefore cannot nor should be gather in one (Wallston, 1993).
Keywords: Diabetes, Puerto Rico, Locus of control, Health, Scale
Cite this paper: Miglany E. Gomila Romero, José R. Rodríguez Gómez, Rosa J. Rodríguez Benítez, Translation, Adaptation and Beginnings of Validation of the Multidimensional Health Locus of Control Scale Form C in a Sample of Type 2 Diabetes Adult Patients in Puerto Rico, International Journal of Applied Psychology, Vol. 6 No. 1, 2016, pp. 10-14. doi: 10.5923/j.ijap.20160601.02.
Article Outline
1. Introduction
- The Puerto Rican population has one of the highest rates of diabetes in the world (Rodriguez & Rodriguez, 2006). Different factors including cultural, nutritional and psychological have great impact in the way diabetes is perceived and treated in Puerto Rico. Statistics for 2007 indicated that approximately 12.50% of the total adult population in Puerto Rico had a diagnosis of Diabetes (Departamento de Salud, 2010). Recently, it has been identified that out of the Hispanic population in the United States, Puerto Ricans have the highest rate of diabetes diagnosis with 13.8% (CDC, 2011). Similarly, the third leading cause of death in Puerto Rico consistently from 1989 to 2014 is Diabetes. Treatments and/or medical interventions usually are aimed to target the root of the Diabetes using medications and nutritional interventions. However, the use of instruments and tools that aim towards the identification of the psycho-emotional aspect of the patient with diabetes is very limited. At the time of this research, psychological interventions in the field of medicine and physical health are gaining importance, and are headed to a bio-integrative approach. Generating an instrument that serves as a measure for estimating the control exercised by patients with diabetes to carry out his/her diabetes management, can be very useful when exploring treatments and their effectiveness/adherence. Knowing the extent to which people with diabetes take into account the external causes, such as chance, luck or fate, or internal causes, as her/his own decisions or efforts, as determinants of their illness, could lead to assess the adherence to selected treatments. With the translation and validation of this instrument it is expected to obtain an adequate tool to screen health locus of control in Type 2 diabetes patients. We expected to obtain an alpha Cronbach of >.70 or higher, which according to Kline (2000) would be an adequate index for a valid instrument.
2. Methodology
2.1. Translation of Instrument
- The first phase of this research consisted in translating the instrument (i.e., English to Spanish and viceversa) using the Brislin back-translating method (Brislin, 1970). The original scale is a "Likert" type scale with 18 items, with score ranging from 1 to 6 (1 = strongly disagree, 2 = moderately disagree, 3 = slightly disagree 4 = slightly agree, 5 = moderately agree, 6 = strongly agree). The scale originally established four dimensions of Health Locus of Control: internal, chance, doctors and others. Internal refers to the extent that the individual recognizes that their behavior affects the results or consequences of their health. Chance refers to the belief the individual has that factors such as luck or destiny have an influence on their health. And doctors/others is the belief the persons has that other people control the outcome of their health. Through the use of two (2) certified translators, there were no significant differences found, hence the first translation was used. After doing so, we proceeded with the second step which consisted in obtaining the content validity of the scale, through the assessment of experts, using the procedure of Lawshe (1975). Said method consisted in finding the proportion of content validity, through the evaluation of the item by a panel of experts on the subject, who indicated whether they are essential for evaluating the theoretical construct in question (Rungtusanatham, 1998). The questionnaire was submitted to be evaluated by a panel of ten (10) experts, whose inclusion criteria were: being doctors specializing in endocrinology, or psychologists who work or have experience in the field of Health Psychology or test construction. Their participation was voluntarily, and they were invited through a letter.
2.2. Gathering and Characteristics of the Sample
- The sample of participants consisted of 108 subjects both male and female, all 21 years of age and older with Type 2 Diabetes. In order to be part of the research, they had to currently live in Puerto Rico and be born on the island. Also, they had to have Type 2 Diabetes diagnosis for 6 months or more, be under medical treatment at the moment, and have access to a computer with internet connection because the sample was gathered through the use of PsychData. The participants were to read first the consent form in which they would acknowledge that they met the inclusion criteria and had fully read the information provided in the form. Later they would continue on to answer a socio-demographic questionnaire and then on to the Spanish instrument, titled, “Escala Multidimensional de Locus de Control en Salud-Forma C”.
2.3. Data Analysis
- After gathering the results, the data analysis consisted of a descriptive statistical analysis (i.e., frequency, percentages) for the sociodemographic variables. Discrimination index (rbis) was carried out for each item. The indexes that are greater than or equal to 0.30 were determined as acceptable according to Kline (2000). Also, the internal consistency of the instrument was assessed using Cronbach's alpha analysis. In order to consider that the instrument was reliable, it was expected that Cronbach's alpha coefficient was equal to or greater than .70 (DeVellis, 2003). Finally, an exploratory factor analysis of principal component with Varimax rotation was performed to understand how the items grouped together. It was expected that the loading factor was greater than or equal to .30 and they had an Eigen value greater or equal to 1 (Kline, 2000).
3. Results
3.1. Content Validity of the Instrument
- Our first goal after having the instrument translated and verified by the panel of ten (10) experts was to obtain the content validity of the instrument. According to Lawshe (1975) formula for content validity ratio (CVR), for 10 judges a CVR score of .62 or greater is desired in order for an item to be included in the instrument. Out of the 18 items originally translated, 12 passed with the required CVR. The CVR of the items included fluctuated between .80 and .99. The Content Validity Index (CVI) for the items retained was 0.94, suggesting that the instrument has adequate content validity.
3.2. Administration of the Instruments
- In order to carry out the recruitment and administration process of the investigation, the platform PsychData was used. This computer platform is commonly used in media data gathering. Through the online participation, subjects were administered a consent form for online participation, a socio-demographic data Sheet and the “Escala Multidimensional de Locus de Control de Salud Forma C”. The research was advertised through Facebook and Twitter, promoting the participation and the sharing of the web link. Those who did participate, once they pressed the link, they were taken to the consent form for online participation. Once there, if they met with the requirements for participation, they would press the “OK” button and continue on to the socio demographic data sheet. To ensure that the participants actually met the eligibility requirements, the question "Do you currently live in Puerto Rico?" was positioned so that if the participant answered "No", he/she would not be able to continue and complete the other instruments. Given the virtual nature of the collected sample, a larger number of participants were obtain in the socio-demographic (n = 140), unlike the participants who completed both instruments (n=108). Of those 140 participants, 12 did not complete the study because they did not meet the requirements, other 12 participants did not complete the socio-demographic and 8 only filled the socio-demographic. Since it we could not identify participants who only filled the socio demographic sheet from, we were unable to exclude them, leaving us with an n = 116 participants in the socio-demographics sheet.
3.3. Item Analysis
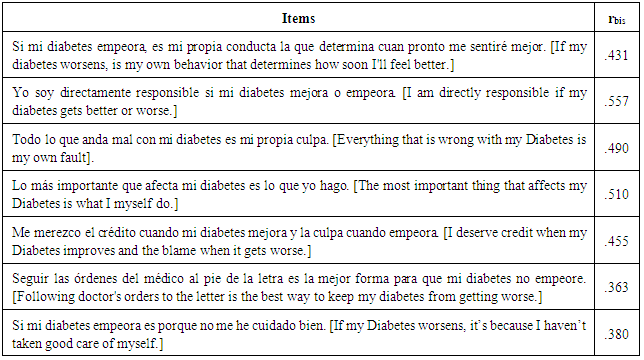
- To begin the statistical analysis of the items used, the of biserial correlation (rbis) index for each one was obtained, in order to know their level of discrimination between participants on the constructs of Health Locus of Control and the multidimensional factors that this entails: internal, chance, doctors and others. According to Kline (2000), the acceptance criteria for the items is obtaining an rbis score of .30 or greater. The results obtained during the analysis concluded that five items were removed, these being: “Si veo a mi médico regularmente, estoy menos propenso a tener problemas con mi diabetes” (If see my doctor, regularly I am less likely to have problems with my conditions); “la mayoría de las cosas que afectan mi diabetes me suceden por casualidad” (Most things that affect my condition, happen to me by chance); “Otras personas juegan un papel importante en si mi diabetes mejora o empeora” (Other people play a big role in whether my condition improve, stay the same or get worse) and “Para que mi diabetes mejore, otras personas tienen que velar que las cosas correctas sucedan” (In order for my condition to improve, it is up to other people to see that the right things happen). When removing the items that did not meet the requirements of a rbis greater than or equal to .30, we finished with seven (7) items ( Table 1).
|
3.4. Factor Analysis
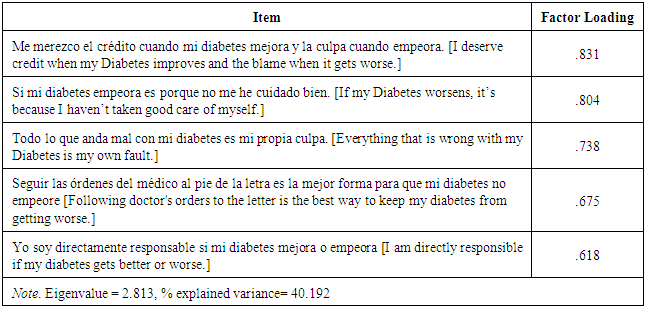
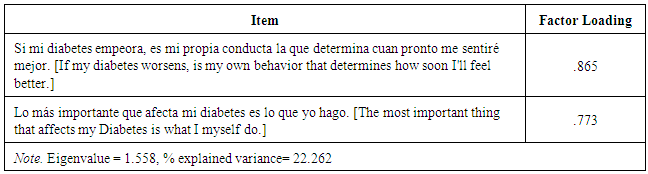
- Based on these seven (7) items, a factors exploratory analysis was performed. As part of this analysis, a Varimax (orthogonal type) rotation was carried out in order to give us a look at the factors underlying the instrument. The first thing we obtained was the measure of adequacy of the sample provided by Kaiser-Meyer-Olkin (KMO = .791), which revealed that the sample size (n = 108) was adequate. Field (2009) explains that a KMO of .70 or greater is used as a reference score to know whether to proceed with the factor analysis and to know whether the sample size is adequate. Also, according to calculations made based on a 70% statistical power, our sample size exceeded the required “n” of 92 subjects (Chow, Shao and Hang, 2008). After the KMO, the Barlett Sphericity test is performed in order to confirm that the correlation matrix is not an identity matrix. A significant Bartlett score was obtained (x2 = 235.79, p<.05). The Principal Component Analysis with Varimax rotation was carried out. This since it reduces the number of variables to a few linear combinations and a more interpretable data base. For the purpose of this analysis and following Kline’s (2000) guideline’s, a factor loading greater than or equal to .30 was used, as well as an "Eigen" value greater than or equal to 1. After these analyses were performed, we obtained that the items were grouped in two components. The first component obtained an Eigen value of 2.81 and it explained the variance in 40.19%. With five items, this component was named “Responsibility and Behavior” (Table 2).
|
|
3.5. Reliability Analysis
- After identifying the relationship between the items and the components identified, we proceeded with the reliability analysis for the seven items which made up the scale. Reliability analysis seeks to establish the extent to which the items meet the criteria measured by the instrument. In general, we obtained an internal consistency of Cronbach's alpha of .79 for the whole instrument. For the first component, which we called “Responsibility and Behavior” an internal consistency of Cronbach's alpha of 0.80 was obtained. For the second component, which we named Self-Monitoring, a Cronbach's alpha of 0.60 was obtained. The load obtained turns out to be lower than expected, but this can be due to small number of items that are observed in this component.
3.6. Correlation Analysis between the Factors
- A direct and statistically significant moderate correlation (r = .436, p <.01) between the two components was obtained. However, although there is a relationship, is not significant enough to eliminate one component or the other. Similarly, the authors of the instrument are very emphatic that the subscales are orthogonal to each other and therefore cannot nor should be gather into one (Wallston, 1993).
4. Conclusions
- Among the various challenges that the people of Puerto Rico face, health problems and their prevention and management remains a highly relevant area. Specifically Diabetes, since it is a widespread disease. For over two decades (1989-2012) this illness remains the third leading cause of death. The most recent statistics published in 2014 (based on data collected through 2012) reported that the prevalence of diabetes increased from 12.8% in 2010 to 16.4% in 2012 (Departamento de Salud, 2014). The rate of diabetes mortality is at 13.8% and ranks in second place of death worldwide, surpassed only by Mexico. Many factors have been described as precipitants of the extremely high levels of Diabetes on the island, from biological and genetic aspects to psychosocial and cultural factors (Rodriguez and Rodriguez, 2006). However, with full knowledge of the scope the condition has in the Puerto Rican population, a lack of innovation in the management of the disease it’s observed. Hence, this research takes the field of health psychology as an essential part of managing chronic conditions, in our case Type 2 diabetes. In the absence of real time statistics and the need to manage more effectively the epidemic that exists on the island, this research provided insight of people with Type 2 Diabetes in Puerto Rico and their Locus of Control within the condition. At the same time it searched for innovative alternatives into managing Diabetes. Thus, the idea of exploring the Health Locus of Control factor and its ability to serve as a tool for health professionals; in the hopes to measure and assess the behavioral aspect of the patient in the management of Type 2 Diabetes. This is fundamental to prevent the morbidity and mortality of the condition. A first step to this goal was through the translation, adaptation and validation of the “Escala Multidimensional de Locus de Control de Salud Forma C”. The “Escala Multidimensional de Locus de Control de Salud Forma C” ended with 7 items, divided into two factors: "Responsibility and Behavior" and "Self-Monitoring. Based on the scores obtained by participants and turned into T scores, the following scoring system was identified to categorize the total levels of Health Locus of Control for patients with Type 2 Diabetes: “Very Low” (scores 30-39), “Low” (scores of 40-49) and “Average” (scores of 50-59). The same system can be applied to evaluate the levels of Health Locus of Control for each component identified. This differs from the original scale. In the original version the score was measured by each factor and not as a whole. Because we have fewer items and most measure just one dimension, we can obtain a total score and in turn evaluate the underlying factors. Both the original instrument and the translated version obtained an internal consistency index greater than .70. Within the course of this investigation some limitations were that given the large population with type 2 diabetes in Puerto Rico, the sample size was not as large enough to be fully representative. Also, using a sample obtained online may limit the access of partakers, and therefore decreases the possibility of adequate participation. And last, the access to clinics or specialized centers where the sample with diabetes could be obtained face to face is extremely challenging, time consuming and highly bureaucratic processes. This makes it detrimental for the development of innovative ways in the treatment of Diabetes in Puerto Rico. We conclude that through this research it was possible to validate and adapt an instrument in the Spanish language, culturally sensitive and valid (Cronbach's alpha of 0.79), to assist in the identification of Health Locus of Control for patients diagnosed with Type 2 Diabetes. It is intended for health professionals, where both patient and provider will benefit, since the measure Health Locus of Control for Type 2 Diabetes patients will help identify the behaviors and beliefs, making it easier for the patient and the provider to adjust treatment and the adherence of patients. Although it does not measure the four dimensions of Health Locus of Control originally established (internal, chance, doctors and others), it can distinguish the dimensions of internal and external identified through the components "Self-Monitoring" and "Responsibility and Behavior". Similarly, we understand that with the use of a socio-demographic sheet relevant to diabetes management elements and beliefs or perceptions that patients have about their condition, the health provider may get valuable information to establish a treatment plan that is more tailored and to which the patient has better adherence. Also, the use of both instruments will shed some light into the Type 2 Diabetes patient to learn about his own patterns of behavior, and in turn, make their own lifestyle changes in order to develop better skills to manage the disease.
5. Recommendations
- It is recommended to conduct the study with a representative sample, preferably at diabetes treatment centers where people come from different regions of the island. This way people will be able to participate in the study without the need for computer access.