-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Applied Psychology
p-ISSN: 2168-5010 e-ISSN: 2168-5029
2015; 5(6): 178-182
doi:10.5923/j.ijap.20150506.06

Lifestyle and Coping Styles among Hypertension Patients and Normal Individuals
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLFariborz Jabbarifard1, Tayebeh Sharifi2, Ali Mohammad Rezaee3, Shahin Fathi Hafshejani2
1Department of Psychology, Shahrekord University of medical sciences, Shahrekord, Iran
2Department of Psychology, Islamic Azad University, Shahrekord Branch, Shahrekord, Iran
3Department of Psychology, Islamic Azad University, Arsanjan Branch, Arsanjan, Iran
Correspondence to: Fariborz Jabbarifard, Department of Psychology, Shahrekord University of medical sciences, Shahrekord, Iran.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Hypertension is a mental and physiological disorder which is developed and aggravated by psychological factors and the patient’s lifestyle not counting biological and physical risk factors. This study explored lifestyle and coping styles in hypertension patients and normal individuals in Lordegan using a causal-comparative analysis. To this end, 50 hypertension patients referring to healthcare centers in Lordegan in addition to 50 healthy people (companying the patients) referring to the same centers were selected through random cluster sampling based on inclusion and exclusion criteria as the respondents in this study and were compared in terms of lifestyle components and coping styles. The data were collected through Demographic Characteristics Questionnaire, Lifestyle Questionnaire, and Psychological Pressure Coping Scale. Then, the data were analyzed using One-Way analysis of variance (ANOVA) and multivariate ANOVA. The results of the study indicated that there is a significant difference between the two groups concerning the use of coping styles (P < 0.05). The results also showed that there is a significant difference (P < 0.05) between the two groups in terms of using lifestyle components. However, no significant difference was found between the two groups regarding physical health and drug abuse avoidance.
Keywords: Stress Coping Styles, Lifestyle, Lifestyle Components, Hypertension, Healthy people
Cite this paper: Fariborz Jabbarifard, Tayebeh Sharifi, Ali Mohammad Rezaee, Shahin Fathi Hafshejani, Lifestyle and Coping Styles among Hypertension Patients and Normal Individuals, International Journal of Applied Psychology, Vol. 5 No. 6, 2015, pp. 178-182. doi: 10.5923/j.ijap.20150506.06.
Article Outline
1. Introduction
- A healthy lifestyle is considered as a valuable resource for reducing the development of diseases and complexities arising from them. It is also used as a way to improve health, quality of life, and adjustment to stress. Lifestyle include behaviors such as eating habits, sleep and rest, exercises and physical activities, weigh control, smoking and drinking alcohol, immunization against diseases, adjustment to stress, and the ability of using family and community support (Lyons et al., 2000). As defined by World Health Organization (WHO), lifestyle refers to individuals’ way of life with a full refection of social values, behaviors, and activities. In addition, lifestyle covers a set of behavioral patterns and personal habits throughout the life (physical activities, nutrition, alcoholism, and smoking) developing as a consequence of socialization (Estagi et al., 2007). Statistics released about the main cases of death suggest that 53% of causes of death are related to lifestyle, 21% to environmental factors, 16% to genetic factors, and 10% to the healthcare system. Numerous studies have shown that 8% of hearth diseases and 90% of diabetes type II can be prevented by making a change in the above factors. In addition, one third of cancer cases can be prevented by improving nutrition, weight control, and performing physical activities and another one third can be prevented by avoiding smoking and changing one’s lifestyle (Park, 2001). Selecting appropriate coping styles against psychological pressures can reduce the impact of such pressure on the individual’s mental health. Problem-focused or rational coping style is used in situations where a person feels that he/she is able to have control the situation or change it. Some practical actions are the use of past experience, realism, collecting more information to solve the problem, seeking advice, and focusing on the positive aspects of the problem. Besides, emotion-focused coping style is used in cases when a person feels that the situation cannot be changed or controlled so he/she reacts emotionally to it or tries to tolerate it. Some practical examples of emotion-focused coping style are getting angry, crying, feeling alone, depression, thinking about past, and turning away from the situation (Hejazi et al., 2000). Problem-focused coping style is regarded as the most appropriate and adaptive way of controlling stress and its application is directly associated with a person’s mental health. In contrast, emotion-focused coping style may reduce one’s attempts to solve the problem so the problem is not solve and even in some cases it turns into a chronic and complicated problem. As a result, this coping style is not always practical and may be used only in uncontrollable situations (Farmanbar, 2000). Accordingly, Tavakoli and Dadsetan (1999) concluded that the use of emotional coping styles is positively correlated with pathological symptoms while the use of problem solving and cognitive approaches has a negative relationship with pathological symptoms. In fact, the adoption of a particular lifestyle can lead to the development of various diseases. Today, most of health related problems (obesity, cancer, hypertension, and other diseases) and death resulting from such problems are associated with lifestyle changes and the way one behaves and lives. Hypertension is a silent, symptomless, and non-communicable disease with an increasing rate in developing communities and is closely related to individuals’ lifestyle. Cancer is alone responsible for 7 million premature deaths worldwide (Ruiking, 2006). Given the increasing number of people affected by hypertension and high costs imposed on the healthcare system to treat such patients, the present study is going to provide a comparative analysis of lifestyle and coping styles among hypertension patients and normal individuals to determine potential affecting factors and control them with the aim of reducing the number of people suffering from hypertension.
2. Materials and Methods
- The present study uses a causal-comparative research method to explore lifestyle and coping styles in hypertension patients and normal individuals in Lordegan. To this end, 50 hypertension patients referring to healthcare centers in Lordegan in addition to 50 healthy people (companying the patients) referring to the same centers were selected through random cluster sampling and they were matched in terms of demographic characteristics.
2.1. Instruments
- Demographic Characteristics Questionnaire: It is a short questionnaire attached to the main questionnaire (Lifestyle Questionnaire) to collect the respondents’ demographic data. Lifestyle Questionnaire (LSQ): The questionnaire was used in this study to measure the respondents’ lifestyles. The final version of LSQ contains 70 items based on a likert scale (Always = 3; Usually = 2; Sometimes = 1; and Never = 0). The questionnaire measure 10 factors/components including 1) Physical health, 2) Sports and health, 3) Weight control and nutrition, 4) Disease prevention, 5) Psychological health, 6) Spiritual health, 7) Social health, 8) Drug and alcohol avoidance, 9) Accident prevention, and 10) Environmental health. Higher scores for each component or for the whole questionnaire show a good lifestyle. La’ali, Abedi, and Kajbaf (2012) examined the reliability and validity of the questionnaire using Cronbach alpha and factor analysis and reported the related values of 0.76 and 0.89, respectively. The reliability of the questionnaire in the present study was equal to 0.83. Psychological Pressure Coping Scale: A short form of Psychological Pressure Coping Scale (Andler & Parker, 1990) was employed in this study to determine coping styles used by the respondents to cope with psychological pressures. The scale was translated and normalized for the first time in Iran by Akbarzadeh and was used in 1984 to 1992 in Tehran to investigate coping styles used against psychological pressures. The scale contains 21 statements that must be responded by a six-point likert scale (None = 0 to Very much = 5). Boyson (2012) reported the alpha coefficients for its subscales as follows: Problem-focused subscale (0.72), Emotion-focused subscale (0.77), and Avoidance subscale (0.74). In addition, the results of a factorial analysis by Callsbik et al., (2002) confirmed the three-factor structure of the sale which shows the scale has an acceptable level of construct validity. The data in the two questionnaires were scored and analyzed using multivariate analysis of variance (MANOVA).
3. Results
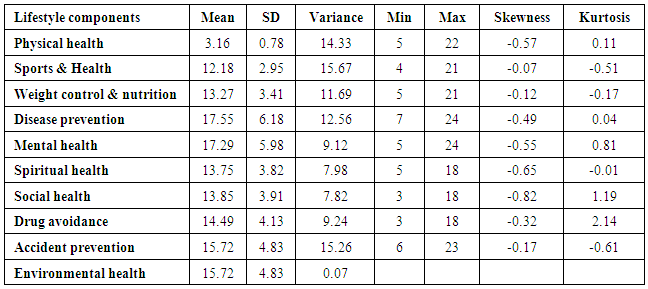
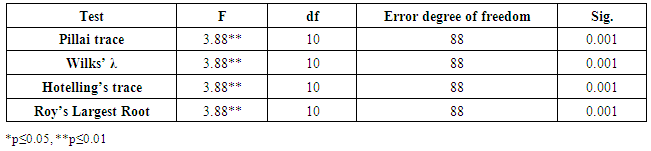
- SPSS software was used in this study to analyze the data and test research hypothesis. The results of descriptive and inferential statistics are presented in tables 1 through 6. Descriptive statistics included mean, standard deviation, variance, minimum, maximum, skewness, and kurtosis. Inferential statistics used in this study included multivariate analysis of variance (MANOVA). The sample under study included 50 hypertension patients and 50 health persons with an average age of 55.7 (with a range of 29-87 years). Table 1 presents the results of descriptive statistics for lifestyle components.
|
|

|
|
|
|
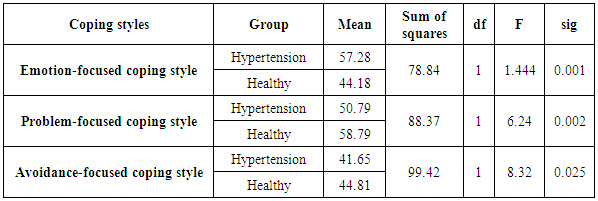
4. Discussion and Conclusions
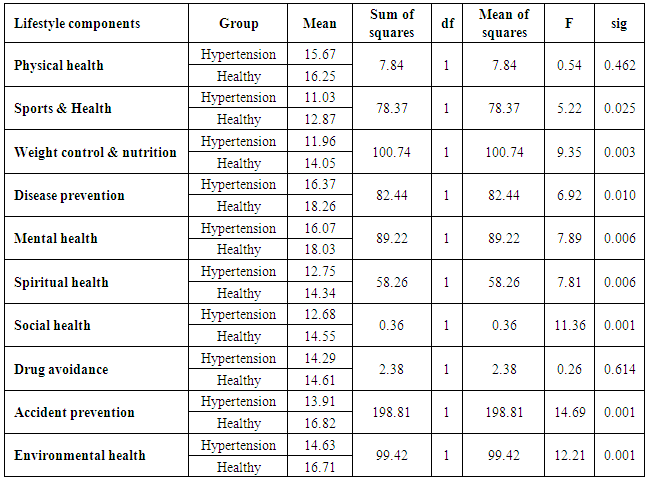
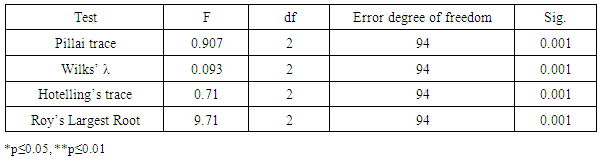
- The results of the study indicated that the differences between hypertension patients and healthy people in terms of lifestyle are significant. This is in line with the results of other studies which showed significant differences between hypertension patients and healthy people in terms of lifestyle. In other words, the two groups are significantly different in terms of all lifestyle components except for Physical Health and Drug Avoidance. In addition, the mean scores of all components for healthy group are higher than those of hypertension group suggesting that healthy people have a healthier lifestyle than hypertension patients as supported by previous studies (Hamidizadeh et al., 2006; Metelska et al., 2010).It was also shown that hypertension patients and healthy people are significantly different in terms of stress coping styles they so that hypertension patients use inefficient stress coping styles such as emotion-focused coping style more frequently than other coping styles, which shows the significance role of stress coping styles in individuals’ physical and mental health. This finding is supported by other researchers such as Miller et al., (2002), Clark (2003), and Davies (1971). As such, when people suffering from hypertension are faced with a stressful situation, they are likely to use emotion-focused coping styles such as turning away from the source of the problem or avoiding the problem to reduce its significance. They may also do things such as playing sports or watching TV to be distracted from the problem. Both hypertension patients and healthy people experience important events in their lives. However, hypertension patients show more emotional responses when coping with stress and problems than healthy people. Hypertension patients usually face their problems using an emotional approach. They show more emotional reactions than healthy people and this aggravates their cardiovascular reactions as shown by Chiou et al., (1997) and Damsa et al., (1988). In summary, what is important more than stress and its intensity is lifestyle and the way one reacts to stressful factors. The actual causes of hypertension are not known in most cases but it can be said that life style and ways used to cope with stress play a significant role in prevalence of this disease. Therefore, it seems that beside medications, healthcare measures should be accompanied by reforming lifestyle and stress coping stress to have more efficient effects.