-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Applied Psychology
p-ISSN: 2168-5010 e-ISSN: 2168-5029
2015; 5(6): 173-177
doi:10.5923/j.ijap.20150506.05

The Relationship between Mental Health and Life Quality among the Cardio-Vascular Patients
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLFariborz Jabbari Fard1, Mohamad Ghasemi Pir Baloti2, Ali Mohamad Rezaee3, Shahin Fathi Hafshejani2
1Department of Psychology, Shahrekord University of Medical Sciences, Shahrekord, Iran
2Department of Psychology, Islamic Azad University, Shahrekord Branch, Shahrekord, Iran
3Department of Psychology, Islamic Azad University, Arsanjan Branch, Arsanjan, Iran
Correspondence to: Fariborz Jabbari Fard, Department of Psychology, Shahrekord University of Medical Sciences, Shahrekord, Iran.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

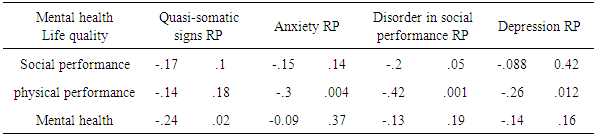
Cardio-vascular diseases are considered as the most important and prevalent threatening factors of human health. In spite of the reduction in the death range due to cardio-vascular diseases during the last decade, these disorders are the major cause of deaths or inability among the individuals. Cardio-vascular patients face many different physical, mental & social problems which may cause disorder in the procedure of their life quality. With regard to the life quality in chronic diseases and the function of training in improving it, the present research has been conducted with the aim of determining the relationship between the mental health condition and life quality among the cardio-vascular patients. Hence, the present study employed a correlation method. In this research, a number of 100 patients, referring to the health & treatment centers in the town of Lordegan, Iran were selected via convenience sampling. The data were collected using the questionnaire of general health & life quality, including a number of 36 questions (short form) and were analyzed using Spearman correlation coefficient, T-test & variance analysis. The findings showed that, many of the domains of the life quality were significantly correlated with mental health. Areas of physical function existed in life quality showed a significant correlation with the three domains of anxiety, disorder in social performance & depression. The mental health area of life quality only showed a significant correlation with quasi-somatic signs area of mental health (P<0.02). Finally, the social performance domain of life quality was significantly correlated with the domain of disorder in social performance in mental health (P<0.05). Moreover, mental health domains such as anxiety with p=.006 showed to have more significant correlation among women as compared to men, and quasi-somatic symptoms with P=0.025 showed to have more significant relationship among woman as compared to men. From among the domains of life quality, physical performance with p=0.03 was more significant among men than women and somatic pain with P=0.001 was more significant among women than men. Concerning the research findings, life quality domains were correlated with mental health areas among cardio-vascular patients, and heart problems have influenced the patients’ different life aspects.
Keywords: Mental health, Life quality, Cardio-vascular disease, Patients
Cite this paper: Fariborz Jabbari Fard, Mohamad Ghasemi Pir Baloti, Ali Mohamad Rezaee, Shahin Fathi Hafshejani, The Relationship between Mental Health and Life Quality among the Cardio-Vascular Patients, International Journal of Applied Psychology, Vol. 5 No. 6, 2015, pp. 173-177. doi: 10.5923/j.ijap.20150506.05.
Article Outline
1. Introduction
- During recent years, we have observed some changes in the disease patterns in the form of decreasing contagious diseases and increasing non- contagious ones (Myres et al.1990). One of the latter is cardio-vascular diseases that are the main cause of deaths throughout the world in spite of the considerable advances in medical sciences and are the death reason for a number of 17 million people in the world annually. It is predicted that, this number will reach a number of 24.8 million people in the world if no preventive action is applied (Sharifirad et al, 2006).In the eastern Mediterranean countries such as Iran, cardio-vascular diseases are considered as an important social & health problem and their dimensions are rapidly increasing (Khoosfi, 2007). On the basis of the report published by the World Health Organization, an amount of 41.3% of deaths was due to cardio-vascular diseases in Iran in 2005, and it is predicted that it will reach 44.8% in 2020. Now, the cardio-vascular diseases are the first cause of deaths among the people, aging more than 35 in Iran (Hosseinifar, 2004). On the other hand, nowadays, the human beings are not only inclined to have increase of the quantity of life but also seek for the life quality improvement (Sayadi, 1999). No unanimous definition has been provided for the concept of the life quality due to its expansion. Life quality is determined on the basis of the individuals’ inference and understanding their own life conditions in relation to cultural as well as their goals, beliefs & attitudes. Life quality is influenced by the factors which give value to life and help create positive experiences and also has different meanings for different people. The individuals’ life quality is their personal opinion and is determined by the individuals themselves (World Health Organization, 1996). During recent years, some attempts have been made in order to focus on the health-related life quality. Expansion of technology in medicine has to some extent caused to forget full attention to the individuals’ needs (Katsching, 1997). Health-related life quality together with treatment interventions place special focus on the feelings of being good satisfied with life; thus, life quality is a meta-health concept, though dependent on it (Ferrans & Powers, 2007; Carr & Higginson, 2001). Health-related life quality is a reflection of the disease’s effects and its treatment with regard to the patients’ perspectives and experiences (Hofer et al., 2003). Unsuitable life quality co-occurs with severity of the disease, less stability, increase in the number of days of hospitalization and decrease in the cardio-vascular patients’ functional activities (Hofer et al, 2003; Havik et al, 2007). Maintaining and enhancing the life quality plays an important role in the patients’ recovery, their more rapid return to the usual life conditions, reducing the disease troubles and preventing the heart disease from its relapse. Hence, the health staff should provide the patients with such necessary training at the time of their hospitalization and release from hospital in this respect. Life quality has been recognized as a valuable criterion for measuring the health conditions in doing studies on medicine as well as public health. WHO (World Health Organization), has considered four dimensions for life quality; they are as follow: Physical health, including items such as a feeling of pain & sadness, sleep & rest and the ability to perform daily activities, 2- Psychological aspect including physical appearance, positive and negative feelings, memory, focus & self-confidence. 3- Social relationships, involving personal relationships, social support & sexual activities. 4- Social environment, containing financial support, home environment, access to information, cooperation in social activities & come-and-go facilities (No authors listed, 1995). Concerning the necessity of secondary prevention among cardio-vascular patients, the research & health care agency of U.S.A. stated that, a number of 2 million new-coming patients are annually in need of care-giving & rehabilitation programs in the U.S.A; since the analyses revealed that, care-giving follow-ups lead to an increase in the ability to perform the activities, a decrease in pain occurrence & anxiety, reduction in the extent of cardiac insufficiency, an increase in the social & familial interactions, and finally improvement of life quality among these patients (Gay, 1999). Assessing life quality, particularly chronic diseases, is of prime importance since, in such diseases, not only the patients’ physical health but also their mental & social health are seriously affected, and most of them continue their life, hopeless at their recovery (Addington & Kalra, 2001). Cardio-vascular diseases are generally categorized as chronic diseases, thus, assessing these patients’ life quality is of importance for treatment–related decision-making (Coelho et al., 2005). As a matter of fact, life quality has a complicated and multi-dimensional concept, involving subjective & objective elements and is often regarded as a definite understanding the satisfaction in life, physical health, social & familial health, hopefulness, rules of etiquette and the patients’ mental health. Just as other patients, affected by chronic diseases, maximizing life quality is the first goal of care-giving among the cardio-vascular patients. Hence, attempts are made to increase life quality, make treatment faster, reduce the hospitalization time and finally reduce hospital-related costs among these patients through necessary interventions. Otherwise, reduction in mental health among the cardio-vascular patients will influence their life quality and can result in losing jobs, familial disconnectedness, disorder in inter-personal relationships and inability in performing the personal, familial & social responsibilities. Thus, regarding the importance of life quality’s concept and the factors related to it among cardio-vascular patients, the present research attempted to analyze the relationship between life quality & mental health among these patients.
2. Materials and Methods
- In this sectional – correlational research, the research population included all the patients, affected by different kinds of cardio-vascular diseases, referring to the treatment & health centers of the town of Lordeghan to receive treatment services in 2013. The number of the sample was 90 patients who were selected via convenience sampling. The inclusion criteria were as follows: aging more than 30 years, the diagnosis of cardio-vascular diseases and confirmed by a heart specialist, passing at least one year from the diagnosis, having no mental problems such as depression & not being treated with mind-altering drugs. The tools used in this study included questionnaire of personal information, questionnaire of public health (having 28 items) and questionnaire of life quality, which had 36 items (short form). The questionnaire of public health contained 28 items in the 4 domains of depression, anxiety, physical signs & social performance. Each of the domains included 7 items. Items 1-7 were related to the physical symptoms, items 8-14, were related to the anxiety, items 15-21 were related to the disorder in social performance and items 22-28 were related to depression, all of which being scored on Likert’s 4-point scale from 0 to 3. The reliability of this tool was obtained as .86 by Cronbach Alpha coefficient. The questionnaire of life quality with 36 items included 8 scales or concepts, involving physical performance, limitation in playing role due to emotional & excitement-related problems, somatic pain, social performance, mental health, being fresh & understanding public health. The reliability of this questionnaire was obtained to be .84, using test-retest method. The manner of answering the items in the questionnaire of life quality ranges from two-choice state (forced-choice) to Likert’s 6-point scale. Concerning the moral considerations & gaining the satisfaction from the patients, the researchers attempted to collect data through interview or completing the questionnaire by the patients themselves. For data analysis, the descriptive statistics as well as inferential statistics (Spearman correlation coefficient, variance analysis & T-test) were used.
3. Results
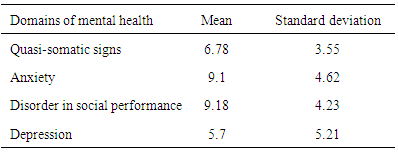
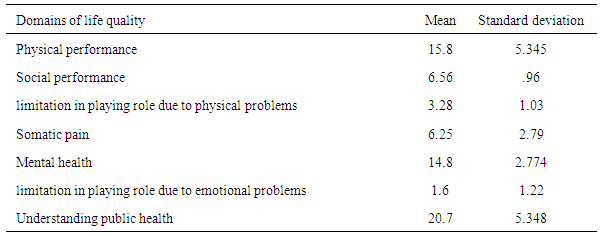
- In this study, 42.2% of the patients aged 40-50 years, 55% were male, 78.9% were married, 74.4% were supported by insurance services, 80% were literate, 43.3% were affected by cardio-vascular problems, 88.9% had hospitalization experiences & 32.2% had familial backgrounds in being affected with heart diseases. Regarding the cardio-vascular patients’ mental health conditions, the mean of disorder in social performance from mental health domain was 9.18, being higher than any other domains. Thus, heart diseases had its most powerful effect on the patients’ social performances (table 1). Concerning the determination of the cardio-vascular patients’ life quality conditions, the highest mean (20.78) belonged to the public health domain & the lowest mean (1.6) belonged to the domain of limitation in playing the role due to emotional & problems. A mean of 20.78 for public health represented its better condition in comparison with that of the other domains of life quality (table 2).
|
|
|
4. Discussion and Conclusions
- During last 20 years, interest in evaluation and improvement of life quality of the patients, affected with chronic diseases has considerably increased, in such a way that improving the daily performances and life quality among the patients with chronic diseases has turned into a goal (Czajkowski, 1998). The results of clinical experiments have shown that life quality can be a sign of quality in health cares and part of the disease treatment programs, and measuring it in chronic diseases provides us with more information on the patients’ health conditions; meanwhile, it can be a suitable guide for enhancing the quality of care-giving (Daugherty et al.,1998). Life quality in chronic diseases confronts with unsuitable changes, in such a way that most patients face dysfunction and deficiency in some dimensions of the life quality due to the particular characteristics of their diseases, and this issue was confirmed in this research. It is believed that, the life quality of those patients affected with serious diseases is correlated with the personal characteristics. It should be noted that there are differences between the patients with similar diseases regarding symptoms & severity of the disease. Such differences are evident even when the patients suffer from the same diseases. Thus, there are obvious differences between the disease effects and each of the patients’ functional abilities. Gaining access to the information about life quality not only helps in giving the patients an effective treatment but also plays a considerable part in enhancing supporting programs and rehabilitating actions. Nowadays, people are in need of improving life quality; thus, the governments all over the world pay more and more attention to the individuals’ life quality improvement and attempt to reduce being affected by the diseases and provide more health services, physical, mental & social welfare among the people of society (Park et al, 1995). In the present research, the results showed that, the cardio-vascular diseases generally had the most negative effect on the mental health conditions, particularly in social performance domain. After disorder in social performance domain with a mean of 9.18, there were anxiety domain with a mean of 9.1, quasi-somatic symptoms domain with a mean of 6.78 and depression domain with a mean of 5.7. Moreover, the results of this study showed that, cardio-vascular diseases had a negative effect on physical as well as social performances. Regarding the relationship between the domains of life quality and mental health, the research results showed that, there was a reversed correlation between social performance domain of the life quality and social performance of mental health, and between psychological health of life quality and quasi-somatic symptoms of mental health. In fact, since the cardio-vascular patients have physical performance disorders, this has influenced their physical health & life quality and has caused a bi-lateral effect on the mental health of these patients. In general, the results of the present study showed that, the majority of the patients with cardiac-vascular insufficiency have a lower life quality than healthy people. Also, based on the studies done by Juenger et al (2002) the majority of cardio-vascular patients suffer from low life quality (Juenger et al, 2002; Jaarsma, 1999; Wielenga, 1998).In their research, Stewart &Blue (2001) concluded that, cardiac insufficiency causes disorder in life quality of the patients more than the other chronic diseases. In a study done by Juenger et al. (2002), a significant relationship was observed between disease severity & life quality. Stewart & Blue stated that, with an increase in disease severity, the patients’ life quality becomes worse and it seems that the disease severity results in more disorder, reducing life quality and increasing the number of referring to doctors and hospitalizations (2001).In the studies done by Non & Michelle (2004), a significant relationship was observed between age and life quality, in such a way that, with an increase in age, the life quality decreased and younger people had a better life quality and women had a lower life quality in some domains, especially in psychological domains as compared to the men. These results were congruent with those of the study done by Parajon et al. (2004).Moreover, Carson et al. (2009), in their research, reported that the patients, aging below 65 years had relatively a better life quality than older individuals. Since the severity of cardiac-vascular diseases increases with a rise in age, life quality is expected to decrease. On the other hand, the younger people are, the more able they are to take care of themselves and also gain a better mental condition with their returning to work, while the older individuals are mostly retired and stay at home.Conam & Acoron (1999), considered economic factors as effective in life quality and stated that, income is an important environmental factor that is in correlation with the individuals’ health conditions and performances and a lower income is accompanied by a weaker evaluation of health level and more performance limitations. Juenger et al. (2002), regarded disease severity as the most important determining factor of life quality among the other variables under study, affecting all the dimensions of life quality. With a rise in disease severity, the life quality lowers, i.e., those patients, being in the fourth rate of the rating by U.S.A. Heart Committee have lower life quality in comparison with those, being in the first rate. A wide research in the U.S.A. revealed that, cardiac insufficiency has caused disorder in life quality of the patients more than the other prevalent chronic diseases and the patients’ life quality became worse with a rise in the disease severity (Stewart & Blue, 2001).Regarding the results of the present research, it is essential to provide necessary and appropriate training for older patients and those who are illiterate or have little education, as well as the unemployed individuals, married patients, those patients being hospitalized more times due to heart diseases and those who have a longer experience of being affected with heart diseases; and some emphasis should be placed on doing such training so that the relapse of such diseases can be prevented among them and it can be effective in enhancing their level of health & life quality. Based on the obtained results, recognizing the severity of mental problems among the patients with cardio-vascular diseases and paying attention to the enhancement of their life quality needs more focus and full attention by the Ministry of Health, Treatment & Medical training more seriously widely regarding treatment projects of psychological teams. On the other hand, establishing and enhancing the supporting institutions and providing the patients with the culture of consistency with types of mental problems among them seem fundamental. Finally, it is necessary to focus on the stance of spirituality in increasing the life quality among these patients. In fact, treatment teams and the staff can provide them with appropriate situations for their spiritual recovery, with happiness and hope as the most important aspects, through recognizing their spiritual needs, since happiness and hope of life are of most essential needs of the patients with chronic diseases in order to enhance their level of mental health and improve their life quality.
ACKNOWLEDGEMENTS
- The researchers express their gratitude for all the patients, participating in the present research.