-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Applied Psychology
p-ISSN: 2168-5010 e-ISSN: 2168-5029
2015; 5(2): 45-53
doi:10.5923/j.ijap.20150502.04
Predictors of Change in Physical Activity and Fruit and Vegetable Intake in a Multiethnic Population in Hawaii at 6 and 12 Months Follow-up
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLJoy C. Galloway 1, Claudio R. Nigg 2, Min Liu 3, Jinan C. Banna 1
1Department of Human Nutrition, Food, and Animal Sciences, University of Hawaii at Manoa, Honolulu, USA
2Department of Public Health Studies, University of Hawaii at Manoa, Honolulu, USA
3Department of Educational Psychology, University of Hawaii at Manoa, Honolulu, USA
Correspondence to: Jinan C. Banna , Department of Human Nutrition, Food, and Animal Sciences, University of Hawaii at Manoa, Honolulu, USA.
| Email: |  |
Copyright © 2015 Scientific & Academic Publishing. All Rights Reserved.
Health-promoting behaviors have been shown to co-exist, but it is unknown if decisional balance with regards to one health behavior may predict change in another behavior. The objective of this study was to examine the relationship between benefits (pros) and costs (cons) of fruit and vegetable (FV) intake and physical activity (PA) and behavior over time, both within behaviors and transbehaviorally. This longitudinal study was conducted in multiethnic adults in Hawaii (n = 700; 63% female; mean age = 47 years; mean BMI = 25.9; mean education = 14.5 years, average household income = $45,000/year). Questionnaires assessed PA and FV pros/cons on a 5-point Likert Scale, PA (MET-min/wk), and FV intake (servings/day). Multiple regression was used to examine the relationship between pros/cons for PA and FV intake and behavior at 6- and 12-month follow-up. At baseline, average FV pros were 4.08 (.91), and average FV cons were 1.88 (.90). Average baseline PA pros were 4.07 (.89), and average PA cons were 1.71 (.77). Multiple regressions revealed that baseline FV pros and cons predicted FV intake, FV cons also predicted PA, and PA pros and cons were not predictive of PA or of FV intake. Study findings provide some support for decisional balance as a useful core construct used in leading theories of behavior change. Improving decisional balance for FV intake may have a beneficial effect on FV intake and potentially PA, indicating a potential gateway effect of decisional balance for FV intake on other behaviors.
Keywords: Decisional Balance, Behavior Change, Fruit and Vegetables, Physical Activity, Transtheoretical Model
Cite this paper: Joy C. Galloway , Claudio R. Nigg , Min Liu , Jinan C. Banna , Predictors of Change in Physical Activity and Fruit and Vegetable Intake in a Multiethnic Population in Hawaii at 6 and 12 Months Follow-up, International Journal of Applied Psychology, Vol. 5 No. 2, 2015, pp. 45-53. doi: 10.5923/j.ijap.20150502.04.
Article Outline
1. Introduction
- Currently, improvements are needed with regards to a number of behaviors impacting the health of the U.S. population [1]. The dietary intake of Americans is less than optimal, with fruit and vegetable (FV) consumption well below the current USDA recommendation of 2 cups of fruit and 2.5 cups of vegetables daily [2]. Similarly, a recent report indicates only one in five Americans meet the recommendations for weekly physical activity [3]. Poor dietary intake, lack of physical activity, and other problematic behaviors may contribute to the development of obesity and related chronic conditions [4-7], creating a burden on the health care system. Chronic health issues resulting from lifestyle choices affect the population across demographic groups [1]. To combat the current obesity epidemic and prevent the onset of disease, there is a need for interventions promoting sustainable change in Americans’ health-related practices [8].Behavior change theory identifies key determinants of behavior that may be manipulated to influence change, providing a framework for the development of evidence-based practices. Previous studies have demonstrated that theory-based interventions for change are more effective, as they provide an understanding of the causal mechanisms of change [9-10]. Theory-based interventions incorporate identifiable active components and provide evidence for the effectiveness of such components, improving both intervention and theory in the process [10]. The transtheoretical model (TTM) is an important behavior change theory which categorizes change into stages, indicating the individual’s intention and readiness to make the desired health behavior change [11]. In addition to characterizing the processes of how people change, the TTM identifies two different important psychological determinants of change-self-efficacy, and the perceived pros and cons of making change [12]. The anticipated benefits (pros) and costs (cons) of making change together are referred to as decisional balance, and are an important predictor of change. Change becomes more likely with the increasing sum of pros minus cons; before change is initiated, the pros must necessarily outweigh the cons [13]. Researchers have shown that changes in decisional balance are especially useful in predicting early stage progression and the initiation of change [13, 14]. This construct in the TTM has been shown to have an important influence across a wide variety of health behaviors [15]. Both increasing pros and decreasing cons have shown to contribute to positive health change for behaviors often targeted in interventions, such as fruit and vegetable intake and physical activity [16-18]. While a number of research studies have examined pros/cons for specific health-promoting behaviors such as FV intake and the relationship with the behavior itself [19-21], there is a lack of research on transbehavioral effects of changes in decisional balance. Previous research has pointed to the need to examine such transbehavioral effects to inform the design of health behavior change interventions, as well as the need for longitudinal change analyses [22]. Through examination of transbehavioral effects, it may be possible to identify mechanisms of ‘transfer’ or ‘gateway behaviors,’ those behaviors that may have positive effects on other behavior changes when modified via intervention. If such behaviors do exist and impact the general health of a population, it may be possible to target the mechanisms of a small number of behaviors in interventions focused on more general health promotion. The ability to focus only on certain behaviors is of significance for researchers designing such interventions, as the difficulty of changing more than one risk factor is well recognized [23].In examining the relationship between various health behaviors, previous studies have identified several behaviors that may have potential gateway effects. Physical activity is one such behavior, which, if adopted, may motivate individuals to engage in other health-promoting activities such as consumption of a healthier diet [23-26]. Several cross-sectional studies have revealed a positive association with physical activity level and participation in other behaviors favorably impacting health [24, 27], and healthy nutrition habits are among the behaviors that have been cited as being tied together with physical activity [23]. Based on these cross-sectional relationships, a recent study further examined the association between physical activity and FV intake in a longitudinal fashion in a multiethnic cohort of adults, with findings indicating that individuals who did more physical activity also tended to eat more FV [28]. However, while this study in a multiethnic cohort provided insight into how behaviors change relative to others, decisional balance was not examined to allow for investigation of how decisional balance with regards to one behavior may impact performance of the second behavior at several time points longitudinally.Given previous results suggesting that gateway effects may exist for specific health behaviors, further exploration of the impact of changes in pros/cons for one behavior on other health behaviors of interest over time is warranted. As self-efficacy, one of the two components of the TTM, has long been shown to be a transbehavioral component of change [29], a similar transbehavioral effect may be expected regarding decisional balance. The purpose of the current study is to investigate the relationship between pros/cons and FV intake and PA over time in a large multiethnic sample in Hawaii, both within behaviors and transbehaviorally. It was hypothesized that: 1) pro/con beliefs for FV would predict FV intake over time; and 2) pro/con beliefs for PA would predict PA over time. In addition, given the association between fruit and vegetable intake and physical activity observed in previous studies and the potential gateway effects of these behaviors, it was also hypothesized that cross-behavioral effects of decisional balance for FV and PA would exist.
2. Methods
- This study is a secondary analysis of data collected from a longitudinal cohort of 700 randomly sampled adults in Hawaii, and was approved by the [blinded] Institutional Review Board. The study procedures are described in detail elsewhere [30]. Briefly, random-digit dialing was used to select 700 English-speaking adults residing in Hawaii to complete a 30-minute survey via telephone. Participants completed the same pre-programmed telephone survey again at 6- and 12-month follow up. The survey assessed decisional balance with regards to changing FV intake and PA, amount of weekly PA in which participants engaged, and amount of FV consumed. All participants gave their informed consent prior to taking part in the study.
2.1. PA Decisional Balance
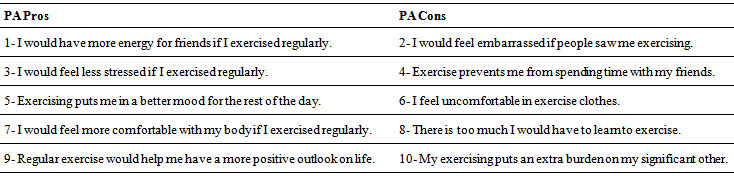
- Decisional balance with regards to engaging in PA was measured by a shorter version (10-item) of a validated 16-item statement set focused on pro and con beliefs [31]. The abbreviated version was tested with principal axis factoring. With direct oblimin rotation, two factors were extracted with simple structure, with each variable loading highly onto one factor only. These two factors had high internal consistency (Cronbach’s alpha = .92 pros; .75 cons). These questionnaires used a 5-point Likert scale, ranging from “not at all important” to “extremely important” to assess participants’ beliefs on the importance of each statement in deciding whether or not to engage in PA [Appendix A].
2.2. Physical Activity
- The International Physical Activity Questionnaire (IPAQ), a validated and reliable tool commonly used to measure PA, was used to assess PA [32, 33], with total MET-min/week used as the PA outcome.
2.3. FV Decisional Balance
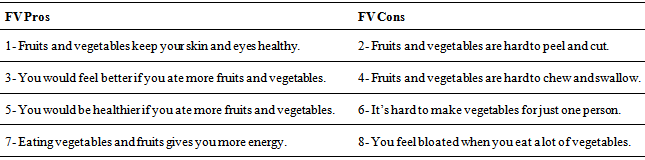
- FV decisional balance was measured by a validated eight-item statement set focused on pro and con beliefs, which has high internal consistency (alpha = .79 pros; .75 cons) and uses the same Likert scale as in PA decisional balance questions [Appendix A].
2.4. FV Intake
- FV intake was assessed using a nine-item food frequency questionnaire developed by the National Cancer Institute (NCI FFQ) [34]. The NCI FFQ has been found to closely correlate with FV obtained from 24-hour recalls (rp = 0.59 men; 0.56 women) [34]. Total intake of FV was calculated to provide a mean number of daily servings.
2.5. Statistical Analyses
- Analyses were performed using IBM SPSS for Mac statistical software package release 22.0.0.0 (IBM Corp., Armonk, NY, USA).i. Descriptive analysis The means and standard deviations of FV, PA, FV pros and FV cons, and PA pros and PA cons at baseline and 6- and 12-month follow-up were calculated, as were statistical descriptions of the baseline demographic variables sex, age, ethnicity, BMI, years of education, and household income, as shown in the first three columns in Table 1. As shown in the same table, bivariate relationships were examined to determine if any of these demographic factors were related to FV and PA or decisional balance at baseline using a correlation matrix.
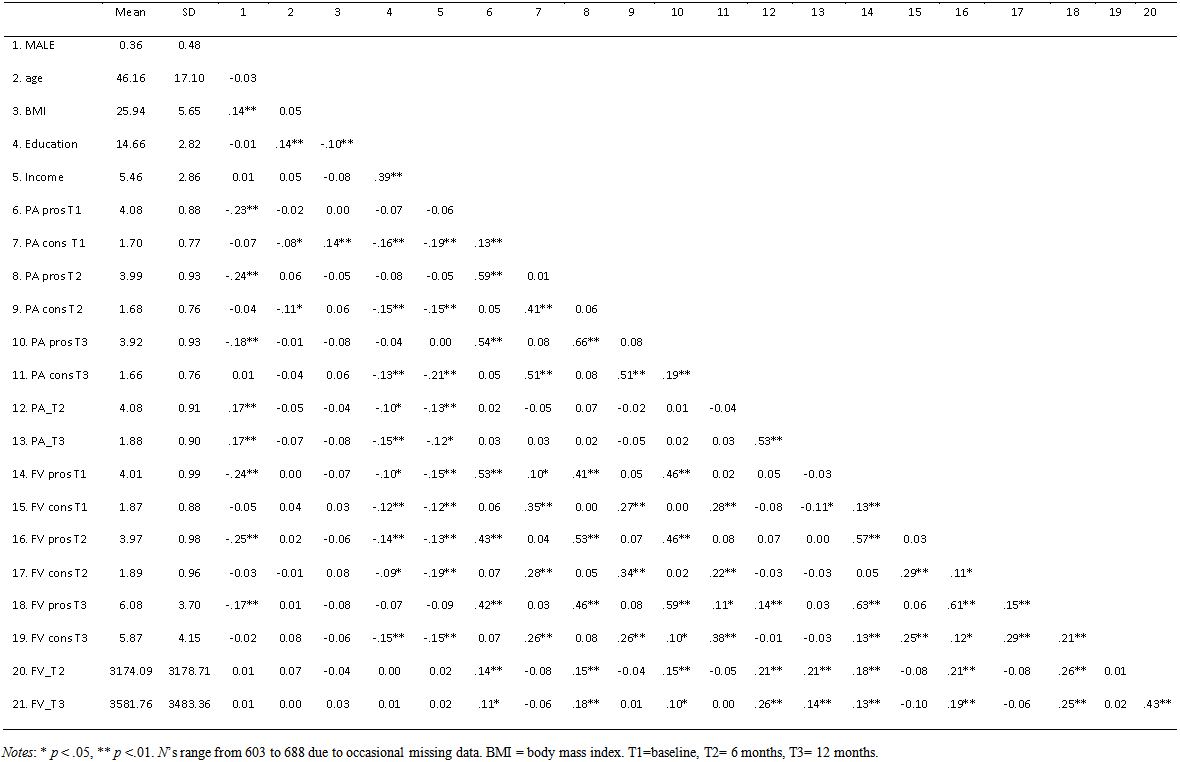 | Table 1. Means, standard deviations, and correlations of model variables |
3. Results
3.1. Descriptive Analysis
- Detailed demographic characteristics and participation and retention rates of the sample have been published elsewhere [19]. In brief, the sample was 36% male and 46 years old on average, multi-ethnic, had a mean BMI of 25.9, 14.6 years education, and an average household income of $55,000/year. The characteristics of the sample were similar to the state of Hawaii’s demographics in most respects, with an overrepresentation of females and Caucasians and an underrepresentation of high income earners and multi-racial residents.From baseline to 6 months, average PA decreased by approximately 1424 Met-min/wk (Figure 1), and by approximately 3 Met-min/wk from 6 months to 12 months. Average FV intake decreased by approximately 0.74 servings/day from baseline to 6 months, and by 0.26 servings/day from 6 months to 12 months (Figure 2).
 | Figure 1. Mean PA at baseline and 6 and 12 month follow-up in a multiethnic adult sample in Hawaii (n=700) |
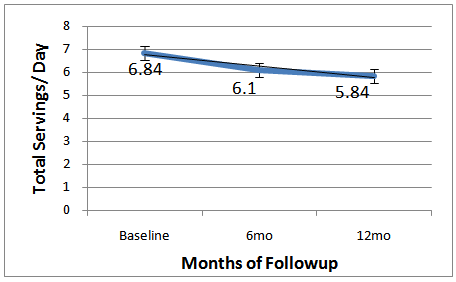 | Figure 2. Mean FV intake at baseline and 6 and 12 month follow-up in a multiethnic adult sample in Hawaii (n=700) |
3.2. Examination of Relationships within Behaviors-baseline Pros/cons with Behavior at 6 and 12 Months
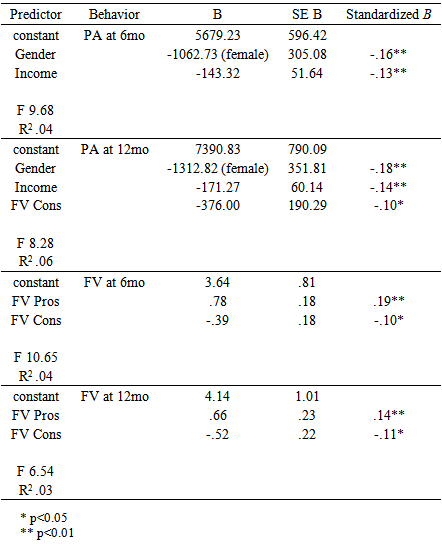
- As shown in Table 2, regression analysis revealed that baseline FV pros were predictive of FV intake at 6- and 12-month follow-up. FV cons were also predictive of FV intake at 6 and 12 months, though more weakly so. Baseline PA pros and cons were not predictive of PA behavior.
|
3.3. Examination of Relationships across Behaviors-baseline Pros/cons with Behavior at 6 and 12 Months
- Cross behavior predictions revealed a significant relationship between FV cons and PA at 12 months [Table 2]; however, not for FV cons and PA at 6 months; nor for FV pros for PA at 6 or 12 months. There were no cross behavior predictions for baseline PA pros or cons with FV for 6 or 12 months.
4. Discussion
- The findings of the current study provide some support for decisional balance as a useful core construct used in leading theories of behavior change, given its ability to predict health behavior. The study also suggests that decisional balance may have some transbehavioral effects, and is the first study to reveal these effects with regards to decisional balance (specifically cons) for FV intake. Results indicate that pro/con beliefs for FV are important predictors of FV behavior and that there is also a cross-behavioral effect of FV cons on PA. These psychosocial factors, therefore, warrant particular attention in behavior change interventions, as promoting attitudinal change can be an effective strategy for influencing positive behavior change. Results may inform clinicians and public health practitioners regarding behaviors on which to focus to better general health; targeting FV cons may lead to changes in other health-promoting behaviors, allowing for tailoring of interventions to most effectively improve health outcomes.Both FV pros and cons predicted FV behavior, though FV pros had a stronger relationship with behavior than cons. These results are in line with phenomena explained by the TTM. Predictable patterns in decisional balance are observed according to the TTM stages of change-precontemplation, contemplation, preparation, action, and maintenance. Of note, cons tend to decrease much more slowly than pros increase across the stages, and may peak even after the precontemplation stage [13, 15, 17]. Difficulties and obstacles that the individual may not have anticipated or may not have considered significant in the precontemplation stage are faced in the contemplation and later stages. Building self-efficacy and mastery over barriers in these stages cause cons to decrease in the action and maintenance stage. Indeed, the results reflect the tendency of cons to have a weaker relationship with behavior than pros, as has also been demonstrated in previous studies [15].Unexpectedly, PA pros and cons did not predict PA. These results do not reflect those of previous studies demonstrating an association between improvements in decisional balance for PA and amount of PA performed [35, 36]. However, in an examination of the stages of readiness to exercise, and their relationship to self-efficacy, decisional balance, and self report of activity in Rhode Island worksites, Marcus et al. [21] found that high pros and low cons were related to physical activity only indirectly, through the mediation of the stage of change variable. Given that the current sample’s behaviors generally exceeded the respective national health goals, it may be that the majority of the individuals in this study were not in the earlier stages of change, in which decisional balance has a stronger effect [15]. In addition, barriers to PA change (e.g. time, energy) may be more difficult to overcome than for FV intake. In terms of transbehavioral effects, having low FV cons was predictive of PA. This may be because the expected costs of FV actually also relate to increasing PA, indicating that FV decisional balance may have a potential gateway effect on other health behaviors. To further examine these gateway effects, future studies may examine whether influencing decisional balance for FV intake also impacts other health-related behaviors such as smoking or alcohol use, as those with a healthy diet may be less likely to engage in these behaviors [23]. A greater understanding of the relationships between various behaviors targeted in health promotion interventions will allow for the design of programs focused on behaviors with broad effects on wellbeing. In addition to elucidating the relationships between decisional balance for FV intake and physical activity and behavior, the current study also allowed for evaluation of differences in behavioral outcomes according to demographic characteristics, as the large sample size and the diversity of the participants supplied a heterogeneous sample. That males tended to engage in more PA corresponds with national statistics [37, 38]. That PA and FV intake were unrelated to BMI, on the other hand, were divergent trends compared to the nation [39]. These findings provide demographic correlates that may be useful in future research and interventions specific to Hawaii.
4.1. Limitations
- This study has several limitations. First, self-report measures of PA and FV intake were used, as data were collected as part of a telephone survey that did not involve objective assessment of behavior. Given this, there was the potential for inaccurate self-reporting of PA and FV intake. Inaccurate reporting of FV intake may potentially have occurred due to error in estimation of serving size, a commonly documented issue with self-reported dietary intake [40-42]. However, this potential error was likely attenuated in the current study by the inclusion of serving size examples to accompany FV serving questions, which has been shown to significantly improve accuracy [34]. A previous study found that, when compared to results from four 24-hour diet recalls in 466 adults, the NCI FFQ closely estimated total FV [34]; others have found that the NCI FFQ significantly overestimated FV [43].In addition to the limitations inherent in a self-report measure of intake, the high reported levels of FV intake and PA may constitute another potential limitation in examining the relationship between decisional balance and behavior. Because the current sample’s behaviors generally exceeded the respective national health goals, it may be that the majority of individuals in this study were not in the earlier stages of change. Previous studies have indicated that decisional balance has a stronger effect in the earlier stages, exerting most influence from movement across precontemplation to contemplation, and contemplation to preparation [15]. Thus, if a larger number of individuals in the preliminary stages had been included in the sample, the effect of decisional balance on behavior may have been even greater.A final limitation relates to the representativeness of the study sample. The aim of random digit dialing was to provide a large sample representative of Hawaii’s population, and it indeed provided a close match in demographic characteristics. However, it is not known to what extent the decisional balance responses are representative of the state. Owning a landline telephone with the state’s local area code and being able and willing to spend approximately 30 minutes per survey may have contributed to differences in personal characteristics the surveys did not capture. The current study adds to a growing field of multiple health behavior change research. An emerging body of evidence shows that changes in one health behavior have a gateway effect of promoting change in another behavior [44]. The underlying mechanisms behind change in multiple behaviors require elucidation through transbehavioral research. That FV cons potentially affect PA change indicates there may be a common mechanism whereby addressing cons for health outcomes caused by one behavior also impacts attitudes for other health outcomes resulting from different behaviors. Thus, while the current study adds to the body of multiple behavior change research, there is great opportunity for future studies to further investigate and discover mechanisms of behavior change.
5. Conclusions
- This study revealed that decisional balance scores for FV were able to predict FV behavior in a large multi-ethnic population, and that cons for FV also predicted PA. Study findings suggest that decisional balance in one health domain may affect behaviors in other domains, indicating that these motivations and barriers may have a gateway effect on other behavior. Given this, inciting change in decisional balance regarding a particular behavior may lead to parallel changes across different health behaviors. More research is needed with regards to transbehavioral decisional balance and effective intervention strategies to promote change across behaviors.
ACKNOWLEDGEMENTS
- Supported by a grant (R01CA109941) from the National Cancer Institute.
Appendix A
- Decisional Balance QuestionnairePhysical ActivityThis section looks at positive and negative aspects of exercise. As I read the following items,please consider how important each statement is with respect to your decision to exercise or not toexercise in your leisure time.Please answer using a 5-point scale where 1 is "not important", 2 is "slightly important", 3 is"moderately important", 4 is "very important" and 5 is "extremely important".So, how important are the following opinions in your decision to exercise or not to exercise?
 Fruit & Vegetable IntakeEveryone has different reasons for eating the way they do. Whether or not you decide to eat 5fruits and vegetables each day depends upon how important the pros--or benefits, and cons--or problems of eating more fruits and vegetables are to you. I'm going to ask to rate each of thefollowing statements based on how important it is to you in your decision to eat, or not to eat,fruits and vegetables.Please answer using a 5-point scale where 1 is "not important", 2 is "slightly important", 3 is "moderately important", 4 is "very important" and 5 is "extremely important".So, in making the decision to eat fruits and vegetables, how important is it to you that_______________?
Fruit & Vegetable IntakeEveryone has different reasons for eating the way they do. Whether or not you decide to eat 5fruits and vegetables each day depends upon how important the pros--or benefits, and cons--or problems of eating more fruits and vegetables are to you. I'm going to ask to rate each of thefollowing statements based on how important it is to you in your decision to eat, or not to eat,fruits and vegetables.Please answer using a 5-point scale where 1 is "not important", 2 is "slightly important", 3 is "moderately important", 4 is "very important" and 5 is "extremely important".So, in making the decision to eat fruits and vegetables, how important is it to you that_______________?