-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Applied Psychology
p-ISSN: 2168-5010 e-ISSN: 2168-5029
2013; 3(6): 169-173
doi:10.5923/j.ijap.20130306.04
Short Version of the Interaction Rating Scale Advanced (IRSA-Brief) as a Practical Index of Social Competence Development
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLTokie Anme1, Kentaro Tokutake1, Emiko Tanaka1, 2, Taeko Watanabe3, Etsuko Tomisaki1, Yukiko Mochizuki1, Bailiang Wu1, Ryoji Shinohara4, Yuka Sugisawa5, Shuntaro Okazaki6, Norihiro Sadato6
1Faculty of Medicine, University of Tsukuba, Tsukuba, 305-0006, Japan
2Research Fellow, Japan Society for the Promotion of Science, Tokyo, 102-0083, Japan
3Ashikaga University, Ashikaga, 326-0845, Japan
4University of Yamanashi, Chuo, 409-3898, Japan
5Ushiku Health Centre, Ushiku, 300-1292, Japan
6National Institute for Physiological Sciences, Okazaki, 444-8585, Japan
Correspondence to: Tokie Anme, Faculty of Medicine, University of Tsukuba, Tsukuba, 305-0006, Japan.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
This study evaluated the validity and reliability of the short form of the Interaction Rating Scale Advanced (IRSA-Brief) as a practical index of social competence development. Fifty adults completed a five-minute interaction session and were assessed with the IRSA-Brief and IRSA. Health social professionals evaluated their social competence based on regular practical assessments.The results indicated that the IRSA-Brief scores had a moderately high correlation with the IRSA scores (r= 0.41) and the professionals’ practical evaluations (r = 0.72). Cronbach’s alpha was 0.84. As the IRSA-Brief can measure social competence with high validity and reliability, providing evidence of social competence development, it would be useful in practical settings to further assist with social competence development, support, and treatment.
Keywords: Social Competence Development, Adult Interaction, Social Evaluation, Interaction Rating Scale Advanced
Cite this paper: Tokie Anme, Kentaro Tokutake, Emiko Tanaka, Taeko Watanabe, Etsuko Tomisaki, Yukiko Mochizuki, Bailiang Wu, Ryoji Shinohara, Yuka Sugisawa, Shuntaro Okazaki, Norihiro Sadato, Short Version of the Interaction Rating Scale Advanced (IRSA-Brief) as a Practical Index of Social Competence Development, International Journal of Applied Psychology, Vol. 3 No. 6, 2013, pp. 169-173. doi: 10.5923/j.ijap.20130306.04.
Article Outline
1. Introduction
- Researchers and practitioners have a long history of being interested in social competence because it strongly affects peoples’ lives and wellbeing. In the 1990s, emotional intelligence[1], which overlapped with social competence, gained much attention[2]. This revived interest in the study of individual differences in emotional abilities and the measurement of basic social competence. The model of emotional intelligence includes the ability to: identify/decode others’ emotions, accurately express/encode one’s own emotions, and monitor and regulate felt emotions [3]. This work suggests that most components of emotional intelligence involve nonverbal/emotional communication skills, which are the key components of the social competence model that underpins the Interaction Rating Scale Advanced (IRSA)[4].The IRSA is derived mostly from multidisciplinary research in the measurement and development of social, emotional, and interpersonal skills[5]. It represents an attempt to develop a general framework for the measurement of the basic social competence components that comprise global social skills or social/emotional competence. Thus, basic social competence is categorized into three skill classes via interpersonal interactions: coordination, regulation, and assertion. Furthermore, these three basic skills operate in two general domains: nonverbal communication and verbal communication. In addition to basic research, there are many domains of practice that are interested in measuring social competence. For example, high levels of social competence predict leadership ability and managerial success[6]. In the health arena, psychologists and counselors have developed methods for the behavioral assessment of social competence with social skills training, a frequently central component of many treatment and intervention programs[7,8]. However, most of these methods are time consuming.Our team has previously developed four social competence scales that can be applied alongside lifespan development. In our study, social competence was defined as the ability to understand others in the context of social interaction and to engage in smooth communication with them. Thus, social competence should be evaluated by the interaction between the person and social environment[9]. The four scales were 1) Interaction Rating Scale (IRS) — observation method for child-caregiver interaction available for children under eight years old[10-11]; 2) Interaction Rating Scale between Children (IRSC)—observation method for child-child interaction available from three to 18 years old[12]; 3) Interaction Rating Scale Advanced (IRSA) — observation method for adult-adult interaction available for adolescents over 15 years old[4]; and 4) Social Skill Scale (SSS)—filled by enumerator method and available for children under seven years old[13]. The scales that were based on accumulated knowledge from the developmental sciences focused on measuring the quality of an environment with the theory that optimistic interactions with the environment are significantly related to healthy development. The Interaction Rating Scale Advanced (IRSA) is a 92-item instrument, which was designed as a brief, yet comprehensive, observation measure to assess basic social competence over 15 years of age. The IRSA is used to measure social competence through five-minute observations of interactions. It forms a behavioral score and six subscales for an impression score, which are “self-control,” “expressivity,” “sensitivity,” “assertiveness,” “responsiveness,” and “regulation.” The 92 items were composed from several sources: original items by the study’s authors, several overlapping items from the Interaction Rating Scale (IRS)[10], the Social Skills Rating Systems (SSRS)[14], and the ENDCOREs[15]. As the IRSA was developed three years ago[4], many researchers and practitioners have asked whether a shorter version of the 92-item measure existed. Although the 92-item version of the IRSA is a reliable, valid, and relatively easy way of assessing basic social competence levels, researchers are increasingly in need of more practical measures to incorporate into their research.Therefore, the aim of this study was to evaluate the validity and reliability of the IRSA-Brief as a practical index of social competence.
2. Methods
2.1. Participants
- Fifty adults (25 men and 25 women) with an age range of 18 to 48 years participated.In order to comply with ethical standards, and prior to conducting the research, all participants signed informed consent forms and were made aware that they had the right to withdraw from the experiment at any time. To maintain the confidentiality of the participants’ personal information, a personal ID system was used to protect their personal information. Furthermore, all video recording data were stored on a disk, which was password protected, and only the researchers who had permission were given access to the data.This study was approved by the ethics committee at the National Institute for Physiological Sciences.
2.2. Measures
- A shortened form of the IRSA was developed: the IRSA-Brief (Appendix 1). In this version, the six IRSA subscales are summarized by the three most common subscales of social competence: “coordination,” “self- regulation,” and “assertion.”The IRSA-Brief was developed by examining each of the original scale’s 92 items, and choosing the most feasible items to represent each IRSA-Brief subscale in terms of content validity and psychometric acceptability. This development was conducted using data that had been collected via the 92-item version of the IRSA. Two different sets of variables were scored for each subscale: behavior items and impression items. Each subscale assessed the presence of behavior (0 = no, 1 = yes) and the sum of all items in the subscale provided the overall behavior score. The total score range was from 0 to 39.Scores for the impression items and the overall impression item were on a five-point scale: 1 = not evident at all, 2 = not clearly evident, 3 = neutral, 4 = evident, 5 = evident at high level. The evaluator completed the 39-item checklist focusing on each behavior (e.g., expresses his/her own feeling to the partner). The health-social professionals provided an impression separately on a five-point scale of the level of interaction for each subscale. Inter-observer reliability was found to be 90%. The IRSA-Brief’s objective is to evaluate interactions in a short period of time in daily situations.
2.3. Procedure
- The participants’ dyads were escorted into a room furnished with a small table and two chairs. The instructor outlined the game to both participants.A five-minute video recording was conducted of the interaction setting in which the two participants played the game using “Keep it steady!” This consisted of a wooden ring and 27 six-inch long sticks of varying widths. Participants grasped all of the sticks together, slid the wooden ring around the center of the bundle, twisted it, and stood it up. The game began with a piece being pulled out and the participants took turns, back and forth, until the structure collapsed. The video recording was undertaken in a room with four video cameras at four different angles (Figure 1).To score the behavior, two evaluators coded all participants’ observed behaviors. The behavior during the interaction was coded as follows. If the participant displayed the behavior described in the item, a score of 1 was given; conversely, if the participant failed to display the behavior described in the item, a score of 0 was given. The total score was the sum of the score that the participant received on all the subscales. A higher score indicated a higher level of social competence. The overall IRSA-Brief score was the overall score of each subscale.Two health social professionals separately evaluated social competence based on regular observations in the practical assessment using the impression items from the IRSA-Brief.
 | Figure 1. Video recording from four angles |
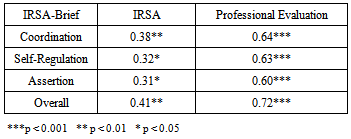
3. Results
- The IRSA-Brief’s validity was examined using the correlations with the original IRSA and professionals’ practical evaluations. These are shown in Table 1.
|
|
4. Discussion
- The IRSA-Brief is an easy-to-administer observation measure that assesses each of the basic social communication skill dimensions that, when combined, comprise global social competence[16]. The general concept of social competence has broad implications for the understanding of many areas of human social behavior[17]. The simple administration of the IRSA-Brief makes it a desirable method for assessing basic social competence.The IRSA-Brief overall score should be comparable to the longer overall IRSA result, so that users interested in a global social competence measure should feel comfortable using either the full IRSA overall score or the IRSA-Brief overall score. It is recommended that the IRSA-Brief be administered with the same instructions, under the same conditions, and using the same Yes-No response format as the original IRSA. Although the IRSA-Brief may be the best instrument to use when one is pressed for time, the use of the full IRSA is recommended, particularly when feedback concerning individual scores is required. The social competence scale for child-caregiver interaction (IRS)[10,11], and child-child interaction (IRSC)[12], were already found to be a reliable, valid, feasible, and practical tool for the studies of social interaction over time. It is meaningful that the IRSA-Brief can be used to assess social competence continually alongside lifespan development.There are a number of advantages to the IRSA-Brief. The IRSA-Brief will be particularly useful in practical settings where professionals do not have the appropriate time required to administer the full IRSA. As it takes only approximately five minutes to complete, with observations, evaluators could score the IRSA-Brief by hand and configure it into a profile. Additionally, evaluators could use the profile to assess the degree of balance contained in the IRSA-Brief score. Furthermore, the IRSA’s framework is based on the most common frameworks used all over the world, making it easy to use in international comparative studies, and the subscales are based on various categories that are widely used in the research of social competence indicators. Although the IRSA-Brief provides valuable strength, it is also important to acknowledge its limitations. First, with only 50 participants in our study, we should be cautious about using the results to generalize. Second, the IRSA subscales might not cover all of the dimensions of social competence, even though we used the most common frameworks of social competence[18]. Despite these limitations, the IRSA-Brief offers a reasonably good, albeit shorter, alternative to the full IRSA. This is particularly true when using the total score as a measure of global social competence. However, as is the case with many abbreviated scales, the accuracy in measuring the construct is diminished.
5. Conclusions
- It is clear that the IRSA-Brief, as with the full IRSA, has the strong potential for use in applied settings. Similar to the full IRSA, the IRSA-Brief has a number of possible applications, specifically in the health-social sciences, education, counseling, and therapy. Further research should expand on the possibilities of practical outcomes for social interaction development by both practitioners and researchers.
ACKNOWLEDGEMENTS
- This research was supported by a Grant-in-Aid for Scientific Research to N.S. (S21220005) from the Japan Society for the Promotion of Science. Part of this study was the result of a project entitled, “Development of biomarker candidates for social behavior,” which was undertaken by the Strategic Research Program for Brain Sciences by the Ministry of Education, Culture, Sports, Science, and Technology (MEXT), and a Grant-in-Aid for Scientific Research (23330174, 24653134).
Appendix 1: Short Form of Interaction Rating Scale Advanced (IRSA-Brief)
- 1. Cooperation1) Looks at partner's face or eyes when the partner attempts eye contact.2) Shares intentions and attitudes with partner via eye contact.3) Smiles or laughs in response to partner's smile or laughing.4) Nods or smiles in response to partner's verbalizations and/or actions.5) Moves in the same manner as the partner.6) Shares emotions with partner.7) Emits a soothing non-verbal response at partner's successes or failures.8) Praises partner's efforts, success, and behavior.9) Does not vocalize or interrupt the partner while he/she is speaking.10) Pauses when the partner starts to verbalize.11) Greets partner.12) Says a word of apology such as, “I am sorry,” to the partner.13) Avoids vocalization, makes a facial expression, or moves inconsistently with the partner's verbalization.14) Avoids vocalization, makes a facial expression, or moves inconsistently with the partner's behavior or nonverbal cues.15) Vocalizes or moves (such as a joke) so as to brighten the atmosphere.16) Shows empathy by verbal or non-verbal responses.17) Behaves to manage a smooth relationship with the partner.2. Self-control18) Makes appropriate eye movements. 19) Makes appropriate physical movements. 20) Makes appropriate utterances. 21) Not tense (hypertonic or hypotonic).22) Tries to respond calmly to partner.23) Is not rude to the partner or materials.24) Avoids displeasing the partner.25) Does not display distress cues even when something does not go well.26) Does not depart from accepted standards.27) Does not demonstrate hypersensitive reactions.28) Is not paranoid or obsessive.3. Assertion29) Casts the partner a glance to seek sympathy.30) Smiles or laughs during the task.31) Attempts to elicit a response from the partner.32) Shows his/her feelings through facial expressions or gestures.33) Expresses his/her thoughts and feelings through facial expressions or gestures that are appropriate for the situation.34) Exhibits a differing opinion.35) Exhibits a differing opinion that is appropriate for the situation.36) Expresses his/her own thoughts to the partner.37) Expresses his/her thoughts to the partner through verbal communications that are appropriate for the situation.38) The words and actions indicate his/her decision. 39) Explains his/her opinion logically.