-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
International Journal of Applied Psychology
p-ISSN: 2168-5010 e-ISSN: 2168-5029
2013; 3(5): 133-138
doi:10.5923/j.ijap.20130305.02
Correlation between Depression and Burnout in Nursing Professionals
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLCláudio Garcia Capitão, Ivani Genchini Nicoletti
São Francisco University, São Paulo, Rua Alexandre Rodrigues Barbosa, 45, Itatiba – SP, 13253-231, Brazil
Correspondence to: Cláudio Garcia Capitão, São Francisco University, São Paulo, Rua Alexandre Rodrigues Barbosa, 45, Itatiba – SP, 13253-231, Brazil.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
The present study aims to correlate the dimensions of Maslach Burnout Inventory (MBI) with Depression Scale (EDEP) in a sample of nursing professionals. The sample included 206 participants comprising 48 nurses, 32 technicians, and 126 nursing assistants who work in two different hospitals in São Paulo. Females (81.6%) constituted a majority of the sample. MBI and EDEP instruments were used along with a socio-demographic questionnaire (SDQ) for the sample characterization. The study results pointed out significant correlations between EDEP and the emotional exhaustion dimension of the MBI (r = 0.52, p < 0.01), as well as between EDEP and all the dimensions of MBI (r = 0.56, p < 0.01). Significant correlations between dimensions of the surveyed scales indicate measures of the same constructs. However, to estimate the prevalence over time, further studies are needed with other professional groups of larger sample size and in places with higher demand for healthcare professionals.
Keywords: Correlation, Burnout, Depression, Nurse
Cite this paper: Cláudio Garcia Capitão, Ivani Genchini Nicoletti, Correlation between Depression and Burnout in Nursing Professionals, International Journal of Applied Psychology, Vol. 3 No. 5, 2013, pp. 133-138. doi: 10.5923/j.ijap.20130305.02.
Article Outline
1. Introduction
- Although there is no unanimous definition for the burnout syndrome, there is a consensus that it appears in an individual as a response to labor stress. The first systematic description of the burnout syndrome was given by psychiatrist Freudenberger[1,2]. Since then, numerous studies have been conducted on its incidence.In the 1980s, it was observed that conceptual development is central in the empirical research and in the evolutionary phenomenon with a focus on occupational categories such as healthcare and education, which aim to take care of people. In recent years, there has been an increase in the number of such studies on other occupational categories. Burnout is an individual process and its evolution usually takes years or even decades. Its appearance is cumulatively slow, with progressive increase in severity that remains unnoticed by the suffering individual, who usually denies that anything is wrong with him/her[3-6]. A worker having burnout syndrome loses interest in his work. Things do not matter anymore and corrective measures do not have any effect. This leads to an internal experience, which results in negative attitudes, implying changes and dysfunctions of the mental state. Burnout appears to be one of the greatest psychosocial problems that affect the quality of life of workers, leading to harmful consequences for them and for their workorganization [3,7-9].This syndrome can occur as a result of prolonged work timings with very short recovery intervals. According to Maslach and Jackson[10], the burnout syndrome comprises three dimensions: (i) emotional exhaustion, characterized by lack of energy, enthusiasm, feelings, emotions, and depletion of personal resources; (ii) depersonalization, a process of hardening oneself and being insensitive, which is expressed in cold, distant, and even cynical attitudes towards those receiving care (customers or colleagues); and (iii) reduction of professional realization, i.e., a tendency to self-evaluate oneself negatively by reducing competitive feelings, thus leading to feelings of frustration, inadequacy, unhappiness, and discontentment.In general, the burnout syndrome is a characteristic of the labor environment. Its symptoms can be divided into four distinct categories: i. Physical symptoms, such as fatigue, constant and progressive dysfunctions, sleep disorders, muscle pain, headache, migraine, gastrointestinal disorders, immunodeficiency, cardiovascular disorders, disturbances in the respiratory system, sexual dysfunctions, irregular menstrual cycles, loss of attention, concentration, and memory, and increased emotions of fear, rage, shame, and contempt.ii. Psychic symptoms, such as inattentiveness and lack of concentration, memory loss, slow cognitive thinking, presence of an alienation feeling, loneliness, insufficiency, impatience, emotional instability, low self-esteem, difficulty in self-acceptance, asthenia, discouragement, dysphoria, depression, mistrust, and paranoiaiii. Behavioral symptoms, such as showing negligence or excess of consciousness in scruples, irritability, increase in aggressiveness, restlessness, difficulty in accepting changes, loss of initiative, increase in consumption of substances (especially alcohol, benzodiazepines), and abnormal behavioral changes, for e.g., high risk of committing suicideiv. Defensive symptoms, such as isolation, feeling of impotence, lack of interest in work or leisure, absenteeism, insomnia, and cynicism[3].Individuals, mostly affected by this syndrome are the most deceived and the most hopeful professionals[11]. Thus, professionals consequently end up in a dedicated, committed, and apathetic attitude, having belief only in oneself. Freudenberger[1] also confirms that professionals who are highly dedicated and committed to their work are most likely to develop the burnout syndrome.Burnout is essentially a social construct that appears as a consequence of interpersonal relationships within the organization. It is sometimes confused with depression[2,5]. Depression, however, is defined as a set of behavioral changes, such as increase in negative feelings, lack of concentration or abnormality in functioning, retirement from social life, loss of interest in professional, academic and playful activities, dissatisfaction in interpersonal relationships, feeling of guilt and self-depreciation, low self-esteem, loss of hope, abnormal changes in sleep and appetite, and lack of energy[12,13].Some authors consider burnout as a depressive condition usually derived from the work environment[14]. Others, however, affirm that depression and burnout syndromes have certain symptomatic similarities, such as tiredness, social isolation, and feeling of depreciation. But this explanation does not take into account significant differences in their clinical symptoms[5,15,16].Depression is one of the most prevalent disorders in any population and it has several etiologic factors.[17-19]. Some factors that cause depression are: (i) biological factors, such as endocrine disorders and genetic influences, evolution, and chemical structures of the brain; (ii) psychological factors, such as stress, trauma, abandonment, issues in perception and problem-solving, and his memories; and (iii) socio-cultural factors, which are usually represented by an individual’s social roles, his expectations, his definition of normality, social structure, and his family’s support[20]. The symptoms of depression include lack of energy, indecisiveness, feeling of insecurity and guilt, chronic disgust, despair, lack of hope, and high irritability[21]. These factors dissuade a person from seeking medical help. Depression is characterized as a pathological condition that greatly impacts the life of an individual, as well as his behavior towards his family and society, and causes frequent and irreparable losses[19,22-25].Several studies have been conducted to investigate the possibility of a correlation between depression and burnout. A study by Ahola et al.[42] used the population-based ‘Health 2000 Study’ in Finland to assess the relationship between job-related burnout and depressive disorders. This study showed that burnout and depressive disorders were clearly related. It concluded that the risk of depressive disorders was greater when burnout was severe. A similar study by Iacovides et al.[15] in Greece concluded that while burnout and depression are separate entities, they may share several ‘qualitative’ characteristics. A 2006 study by Bauer et al.[43] investigated the correlation between the burnout syndrome and psychological and psychosomatic symptoms among school teachers in Germany. The study concluded that for school teachers, burnout syndrome, a construct that derived from occupational psychology and occupational medicine, is significantly correlated with psychological andpsychosomatic symptoms.Murcho et al.[26] surveyed a sample of 499 nurses who worked for the Hospital Units of Algarve, Portugal. They used the depression sub-scale of EADS (Depression Anxiety Stress Scales-21) proposed by Lovibond and Lovibond[27] in its Portuguese adaptation of Ribeiro et al.[28], and the MBI in its Portuguese adaptation for nurses. Their results suggested that depressive situations can occur as a consequence of burnout in a work situation. However, the study does not indicate any clear evidence for the reverse relation, and it concludes that these two entities are different constructs, despite their common characteristics.Queiróz et al.[29] conducted a study on a sample of 48 nurses from three health centers of Bragança, Portugal, to explore the levels of anxiety, depression, and burnout in nurses who work with primary healthcare centers. The instruments used to evaluate depression and burnout were the hospital anxiety and depression scale (HADS), which is the Portuguese version adapted by Ribeiro et al.[30], and the MBI, which is a Portuguese version. For anxiety and depression, the average was 7 and 5 respectively from a maximum of 28 points. The study also revealed a greater tendency for anxiety and burnout among unmarried nurses, while depression seemed more frequent among married nurses with children. Queiróz et al.[29] also observed that nurses with more professional experience and permanent work agreement (therefore, with certain stability) showed more anxiety and depression, while nurses with less professional experience and fixed-time work agreements (therefore, with professional instability) showed a greater rate of burnout. The study did not present any MBI cutoff. In Germany, investigating 20 Intensive Care Units, Keijsers et al (31) obtained averages of 15.4 for emotional exhaustion (EE), 7.19 for depersonalization (DE) and 30.43 for professional accomplishment (PA) in 576 Nursing workers. In the USA, Schaufeli & Enzmann (32) found 11 studies in the nursing category, in a total of 1,542 participants. This sample showed an average of 23.80 for emotional exhaustion (EE), 7.13 for depersonalization, with 13.53 being the reduced average for professional accomplishment. The results pointed out that the American nurses presented one of the lowest averages for personal accomplishment at work, when compared with other professional categories.To test the association between alexithymia, burnout, depression, and family support, Brats et al.[33] conducted a study on a sample of nurse professionals of a Greek hospital. 95 nurses participated in the study that included 78 women and 17 men, with an average age of 36.7 years and with approximately 10 years of work experience. The instruments used were the Alexithymia Scale of Toronto, the MBI, Beck Depression Inventory (BDI), and Julkumen’s Family Support Scale. A moderate correlation of serious depressive symptoms was found in 16.8% of the participants. Alexithymic characteristics were observed in 14.7% participants, while low family support was observed in 15% participants. In the burnout evaluation in participants, emotional exhaustion was noticed in 38.9%, depersonalization in 46.3%, and lack of professional realization in 49.5%. 14.7% participants reported pathological scores for all sub-scales. Women presented higher levels of depression (evaluated by BDI) and alexithymia (evaluated by TAS-20), but lower levels of professional realization (evaluated by MBI) and family support perception as compared to men.The above studies suggest burnout and depression as separate entities, even though they share various qualitative characteristics in common, especially the gravest forms of burnout with low level of satisfaction in their daily work.However, in contrast, the present study aims to evaluate and correlate the consequences of burnout and depression in an individual’s work environment. It aims to correlate MBI and EDEP evaluations to detect work-related infirmities . This study is important as an attempt to establish a causality relationship between burnout and depression in the nursing profession in the specific context of Brazil, and thereby help policymakers improve the work environment for professionals.
2. Methods
- The study sample consisted of 206 nursing professionals including nurses, technicians, and assistants from two hospitals (one public and one non-profit), in two cities in São Paulo.The samples were chosen by considering the convenience of participants. This was essential because they were working in shifts during data collection. Only professionals with more than one-year work experience and aged above 18 years were included in the study.
2.1. Instruments Used
- A socio-demographic questionnaire (SDQ) was employed for sample characterization. The MBI-Human Services Survey (MBI-HSS) was used to evaluate the burnout syndrome, and EDEP to evaluate symptoms of depression. Maslach et al.[34] suggested two versions of the MBI that have been extensively used in empirical studies: the original HSS that is more suitable for service providers; and the most recent General Survey (GS), which can be applied to a broad range of professions. The first version of MBI evaluated the intensity and frequency of the answers with a scoring scale of Likert type, varying from 0 to 6. The second version of MBI, issued in 1986, evaluated only the frequency because of high association between both the scales. Other studies also point out a correlation greater than 0.80[10].Maslach et al.[35] exclusively employed the inventory for evaluating the burnout syndrome without taking into consideration the preceding elements or the consequences resulting from its process. It identifies burnout rates in accordance with the score in each dimension. High values of emotional exhaustion and depersonalization, and low values of professional realization, are significant indicators of burnout. Gil-Monte and Peiró[2] reinforced the importance of evaluating MBI as a tri-dimensional construct, i.e., all three dimensions must be evaluated and considered to maintain the perspective of the syndrome. The MBI-HSS prepared by Maslach and Jackson[10] was used in this study to evaluate burnout rates. The instrument is self-applied, totaling 22 items, and in its original American version, the frequency of the answers is evaluated by a scoring scale that varies from 0 to 6. Even in the Brazilian version the scale totals 22 items and its score varies from 0 to 5[36-38].The MBI evaluates an individual’s relation with his work in accordance with the three dimensions established by the Maslach Model: 9 items of emotional exhaustion (1, 2, 3, 6, 8, 13, 14, 16, and 20); 8 items of professional realization (4, 7, 9, 12, 17, 18, 19, and 21); and 5 items of depersonalization (5, 10, 11, 15, and 22). These 22 items indicate the frequency of the answers with a scale whose score varies from 1 to 7. A scoring system of 1 to 5 was chosen for this study. Each component of the MBI was analyzed separately as a continuous variable. In emotional exhaustion, 27 or more points indicate a high degree, 17-26 points indicate an average degree, and less than 17 points indicate a low degree. In depersonalization, 13 or more points indicate a high degree, 7-12 points indicate an average degree, and less than 7 points indicate a low degree. In professional realization, 39 or more points indicate a high degree, 30-38 points indicate an average degree, and less than 30 points indicate a low degree[39]. Presence of burnout syndrome is associated with high emotional exhaustion, high depersonalization, and low professional realization at work[10]. The EDEP is a Brazilian instrument used to measure the symptoms of depression[40]. It indicates 26 symptoms of depression: depressed humor, lack of interest in pleasurable activities, crying, despair, abandonment, indecisiveness, feeling of incapacity, feelings of inadequacy, dependency, negativism, avoidance of social situations, reduction in productivity, unusefulness, severe self-criticismincorporated with negativism, guilt, decrease in concentration, suicidal tendency, lowered self-esteem and self-confidence, lack of perspective about the present situation, hypochondria, changes in appetite, changes in weight, insomnia or hypersomnia, psychomotor slowness or agitation, loss of libido, fatigue, energy loss, and irritability. Some of these indicators refer to opposite situations, such as changes in appetite where the change might be positive or negative and in such case both the changes must be captured by the instrument. From the above indicators, 150 phrases were created that approached each symptom negatively and positively, such as “I do things that I like” and “I don’t want to do the things anymore that I liked earlier” (which are related to the symptom of “a lack of interest in pleasurable activities”) and “I have been crying much” and “I haven’t been crying” (which are related to the symptom “crying”). Thus, after eliminating repeated and dubious phrases, 75 non-redundant items were generated, each composed by a pair of phrases. Psychometric studies further reduced the scale to 32 items, each composed by a ruler containing three circles where the participants had to indicate a single circle that better expresses how they feel in relation to the statements. The participant must then choose the circle immediately closer to the phrase either to the left or to the right, in case he or she agrees with the statements. The circle at the center should be marked if the feeling could be classified as “more” or “less”. Several studies were conducted to seek evidences for validity and other psychometric qualities for the 75 descriptors composed initially in the EDEP[40].
2.2. Procedure
- The project was first approved by the Ethics and Research Committee of the University of São Francisco and then the Informed Consent Form was read and signed by all participants. The study was initiated by samplecharacterization with the SDQ, followed by the EDEP and MBI evaluations. The total evaluation time was approximately 40 minutes.
3. Results and Discussion
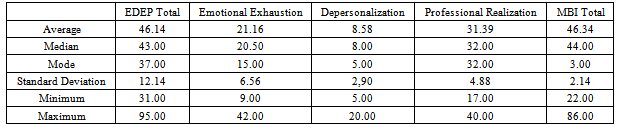
- Two hundred six nursing professionals participated in the study. They included 126 (61.2%) nursing assistants, 32 (15.5%) nursing technicians, and 48 (23.3%) nurses. Majority of the participants were women because the nursing profession in Brazil is mostly composed of females.Table 1 presents the results obtained after the application of EDEP and MBI. Participants reported an average score of 46.14 (SD = 12.14), with a minimum score of 31.0 and maximum score of 95.0.For MBI, the emotional exhaustion dimension presented an average value of 21.16 (SD = 6.56), considering 17-26 points as average for exhaustion evaluation. The depersonalization results (M = 8.58; SD = 2.90), agree with the average standard stipulated by the instrument (7-12 points). For professional realization dimension, the average value obtained was 31.39 (SD = 4.88), which was in accordance with the average level (more than 30 points). The data obtained is in accordance with the criteria of burnout syndrome that is characterized by high levels of emotional exhaustion and depersonalization, and low levels of professional realization [7,8,16,10,36,39,41].The scores of both the applied instruments were correlated to fulfill the aim of the study. The scores of EDEP evaluated the symptoms of depression, while the MBI dimensions evaluated the burnout rates. As shown in Table 2, highly significant correlations were observed between the scores of EDEP and MBI in all dimensions (r = 0.56, p < 0.01).
|
|

|

4. Conclusions
- The present work aimed to correlate the MBI and EDEP instruments in a sample of nursing professionals. Highly significant correlations were found between EDEP and all the dimensions of MBI (r = 0.56, p < 0.01), demonstrating a correlation between the pertinent constructs of both instruments. The vacation time variable was studied to check if it influenced the obtained scores. The correlations for emotional exhaustion and MBI were significant with all its three dimensions. The results revealed that the burnout symptoms could be chronic and could be replaced with other segments of the person’s life, even when the person is not involved in any work activity.The present study did not survey the frequency of leaves taken, recurrent absenteeism, or other reasons that might be directly related with chronic work stress and/or depression. Therefore, further studies are required with other groups of professionals, with bigger sample size and in places having intense demand for healthcare professionals to explore the correlation between burnout and depression better. The burnout syndrome as well as depression is responsible for irreparable suffering among workers. People with such symptoms need support and help, especially in the hospital, shelter, and nursery environments. The unkind, cold, distant, and at times negligent service could be related to such a condition.
ACKNOWLEDGEMENTS
- We thank the nursing professionals who participated in this study.