-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Human Resource Management Research
p-ISSN: 2169-9607 e-ISSN: 2169-9666
2014; 4(2): 19-26
doi:10.5923/j.hrmr.20140402.02
Determining the Precedence Order of the Factors Influencing Doctors’ Choice of Specialty in Turkey
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLEmrah Önder1, Sündüs Dağ2, Güler Önder3
1School of Business, Department of Quantitative Methods, Istanbul University, Istanbul, 34322, Turkey
2School of Business, Department of Production, Istanbul University, Istanbul, 34322, Turkey
3Istanbul Medical Faculty, Neurosurgery Critical Care Unit, Istanbul University, Istanbul, 34104, Turkey
Correspondence to: Emrah Önder, School of Business, Department of Quantitative Methods, Istanbul University, Istanbul, 34322, Turkey.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Choosing a carrier is a kind of multi-criteria decision making problem and it is a crucial decision in people's life. The aim of this study was to determine the precedence order of the factors influencing choice of doctors as a carrier, to derive the relative weight of each factor and to identify differences and similarities in such factors between genders. In analyzing the data, three-tier Analytical Hierarchy Process (AHP) methodology was used. The questionnaires were answered by 57 doctors from 20 different specialties. In this study, subjective opinions of doctors turn into quantitative form with Analytic Hierarchy Process. This study found that “Compatibility with the individual knowledge, skills and the ability”, “Communication skills”, “Predisposition to team/ individual work / Being introverted-extroverted”, “Opportunity to apply surgery, treatment etc.” and “The specialist physician as a role model” were more important factors for doctors in choosing their specialty. Among the criteria, the criterion of “Less administrative tasks”, “Features in terms of academic career” and “Prestige of specialty” had the lowest weight for doctors. Main differences between male and female specialists’ preference occur in these factors: “Communication skills”, “Opportunity to apply surgery, treatment etc.”, “The specialist physician as a role model”, “The number of patients served”, “The necessity of coming face to face with patient” and “Duration to complete the training process”. Results of this study can be used by medical school management, medical leaders, Ministry Of Health, medical school academicians etc.
Keywords: Multi criteria decision making, Service sector, Specialty choice, Career of doctors, Career choice, Analytic hierarchy process
Cite this paper: Emrah Önder, Sündüs Dağ, Güler Önder, Determining the Precedence Order of the Factors Influencing Doctors’ Choice of Specialty in Turkey, Human Resource Management Research, Vol. 4 No. 2, 2014, pp. 19-26. doi: 10.5923/j.hrmr.20140402.02.
Article Outline
1. Introduction
- This paper is arranged into five sections. The first section provides an overview of existing studies about factors influencing choice of medical specialty. The second section gives information about medical education in Turkey. The next section describes the proposed methodologies. In section four the usage of AHP to analyze priorities is shown. Finally, results of the study are followed by concluding remarks and discussions.There are so many studies in the literature about factors influencing choice of medical specialty. We summarized some of the studies until today in order to reflect the factors influencing choice of medical specialty in different studies and countries.Culler and Bazzoil (1985) discovered in their study of the physician labor supply that an extremely significant positive correlation existed between physicians' working time and compensation rate [1]. Babbott et al. (1991) studied to determine the attitudes of medical students toward careers in internal medicine [2]. They discovered that the most important factor in their choice of specialty was intellectual content. Diagnostic challenge was next most frequently cited. Type of patient seen and role models were more frequently cited as the most important factors in specialty choice. DeWitt et al.(1998) identified the factors that motivate graduates of a large university-based, internal medicine training program in primary care to pursue generalist or subspecialty careers [3]. They offered that eight different factors: preferred location, salary, working hours, time for family, breadth of knowledge/skills required, breadth of clinical problem addressed in practice, mentors, an opportunity for continuity of care. Yang and Tsai (1999) investigated the factors effecting choice of specialty at a medical center in Taiwan [4]. This study detected that the major factors affecting the choice were economic factors, study experience, persons' expectations, and personal factors. Kao et al. (2000) discovered that the basic factors influencing specialty choice were personal interest, suitability with personality, workload and work pressure[5]. Azizzadeh et al. (2002) investigated factors influencing career choice among medical students interested in Surgery [6]. Their study indicated that prestige and career opportunities are more important factors for medical students interested in surgery. Concerns about lifestyle and work hours during residency and perceived quality of patient/physician relationships were deterrents to surgery as a career choice. Hung et al. (2005) identified the important factors that Taiwan’s medical students consider when choosing a specialty using AHP [7]. They found that income is no longer an important factor affecting choice of specialty students still care about the relative fairness of compensation when choosing their specialty. Cochran et al. (2005) analyzed characteristics of general surgery residency and practice and their influence on student interest in surgical careers [8]. This study was performed with an internet-based survey. According to the result of study, students who choose surgical careers are not deterred by a negative perception of lifestyle and workload considerations. Mentoring and personality fit are central in medical student specialty selection. Avgerinos (2006) investigated the career choices, location preferences and criteria among medical students in Greece [9]. Chang et al. (2006) investigated the factors that Taiwan’s medical students consider when choosing their specialties using Saaty’s AHP [10]. Their study found that personal intelligence/ability preference and career opportunities were more important factors. Saigal et al. (2007) conducted qualitative interviews with 25 Japanese medical students regarding factors influencing specialty preference [11]. They stated that preclinical and clinical experiences as well as role models were reported by Japanese students as influential factors when formulating their specialty preferences. Fielding et al. (2007) determined identifiable factors that dissuade female medical students from entering the field of radiology [12]. The study showed that intellectual stimulation and use of emerging technology were significantly more important than other factors and the most dissuaded factor from a career in radiology was lack of direct patient contact. Soethout (2008) investigated students’ development of interest in a career in a public health in Netherlands [13]. This study pointed that Interest in a career in occupational health and social insurance health was low throughout medical school.Caner and Ökten (2010) examined the college major choice decision in a risk and return framework using university entrance exam data from Turkey [14]. According to the paper, family income, father’s self-employment and social security status are important determinants of choosing a major with a higher labor income risk such as business over a less risky one such as education or health. Glynn and Kerin (2010) identified important criteria influencing junior doctors in choosing a career in surgery [15]. Their results demonstrated that the three most important influences in career choice for medical students and junior doctors are employment, career opportunities and intellectual challenge. Riska (2011) made a review on female-male students and medical career choices [16]. Rehman et al. (2011) intended to elucidate the specialty preferences of Pakistani medical students and the factors which effect medical students to make the decision regarding which specialty to follow [17]. According to this study, More than 70% of the students were influenced by a specialty that was suited to their personality, time commitment, prestige labeled, and its scope internationally. Weissman et al. (2012) performed a study about specialty considerations by medical students early in their clinical experience at two Israeli medical schools [18]. The objective of this study was to serve as an impetus to medical educators and healthcare leaders to become interested in students’ career selection.
2. Medical Education in Turkey
- Medical education takes six years in Turkey, first three years being pre-clinical years and the latter three being Clinical years. Right after graduation, graduates can either work as Practitioner or take another exam called TUS (Medical Specialization Examination) to do residency in a particular department of a particular hospital. The physicians who do not pass the examination but want to specialize are granted a practitioner’s position in the National Primary Health Care System by the Ministry of Health. Candidates who pass the exam are placed in departments according to their score. There are two kinds of hospital for the medical specialty education in Turkey; education / research hospitals and the university hospitals. Physicians who want to have carrier in a specialty area prefer to work in University hospitals. University hospitals and educational and research hospitals are different from each other in some ways. Relationship between education / research hospitals specialists and assistants is formal in university hospitals, while friendlier in education / research hospitals. Education is more important than service in university hospitals. In university hospital, number of shifts is more than education/research hospitals because of the sub-departments. Also, additional payment is higher in educational and research hospitals because of the number of patient.
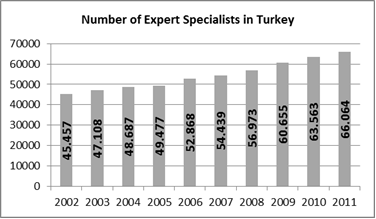 | Figure 1. Number of Specialists in Turkey [19] |
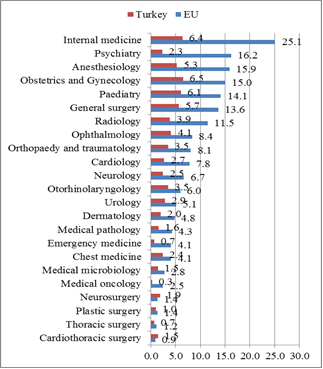 | Figure 2. Number of specialists per 1000 people in Turkey vs. EU [20] |
3. Methodology
- Multi-criteria decision making technique called Analytic Hierarchy Process (AHP) is applied to determine the relative weights of the evaluation criteria. AHP approach achieves pairwise comparisons among factors or criteria in order to prioritize them using the eigenvalue calculation [21], [22]. AHP model was represented in a questionnaire to survey doctors’ opinions. The relative weight of each factor in the model was calculated.
3.1. Content and Participants
- The study group of the research is 57 specialists with an age range of 27-63. 24 of the specialists (42%) are female and 33 of them (58%) are male. The questionnaire conducted between the dates 1 March 2013 – 30 June 2013. Specialists were informed that participation in the study was voluntary and that their responses would remain anonymous. Data were collected from the specialists in their offices. Specialists are asked to compare the criteria at a given level on a pair-wise basis to identify their relative precedence.
3.2. Data Gathering Instruments
- AHP is an effective decision making method especially when subjectivity exists and it is very suitable to solve problems where the decision criteria can be organized in a hierarchical way into sub-criteria. The findings of previous studies about factors influencing specialists’ choice of branch were first identified by literature review. Specialists expressed or defined a ranking for the attributes in terms of importance/weights. Each specialists is asked to fill ‘‘checked mark’’ in the 9-point scale evaluation table. The AHP allows group decision making. One of the main advantages of the AHP method is the simple structure.
3.3. Analytic Hierarchy Process
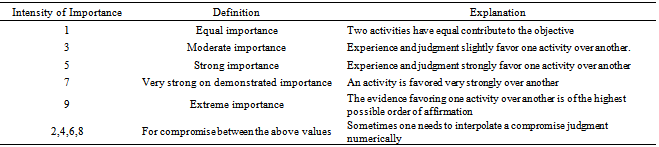
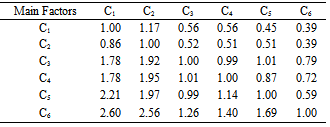
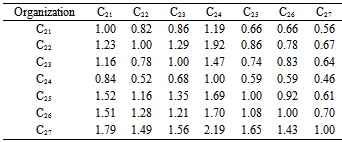
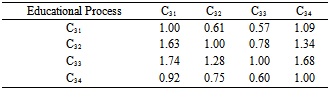
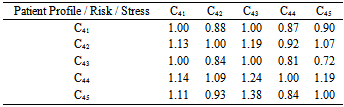
- AHP was developed in the 1970s by Thomas Saaty is a multi-criteria decision making (MCDM) methodology. It has been used extensively for analyzing complex decisions. The approach can be used to help decision-makers for prioritizing alternatives and determining the optimal alternative using pair-wise comparison judgments [21], [22].The AHP is a selection process that consists of following steps [23], [24], [25].1. Define the problem and determine the criteria. Factors and related sub factors must be correlated [26].2. Structure the decision hierarchy taking into account the goal of the decision.3. Construct a set of all judgments in a square comparison matrix in which the set of elements is compared with itself (size nxn) by using the fundamental scale of pair-wise comparison shown in Table 1. Assign the reciprocal value in the corresponding position in the matrix. For a set of n elements in a matrix one needs n(n-1)/2 judgments [26].
|
|

 | (1) |
 | (2) |
 | (3) |
 | (4) |
 | (5) |
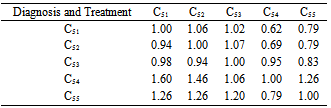
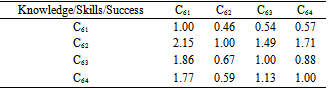
4. Using AHP to Analyze Priorities
|
|

|
|
|
|
|
5. Results
- 6 first level criteria and 31 sub criteria are given in Figure 3. The study found that “Compatibility with the individual knowledge, skills and the ability” (10.9%), “Opportunity to apply surgery, treatment etc.” (6.5%) and “Predisposition to team/ individual work / Being introverted-extroverted” (6.1%) were important for male specialists, whereas “Compatibility with the individual knowledge, skills and the ability” (7.2%), “Communication skills” (6.7%) and “Predisposition to team/ individual work / Being introverted-extroverted” (6.1%)were important for female specialists.
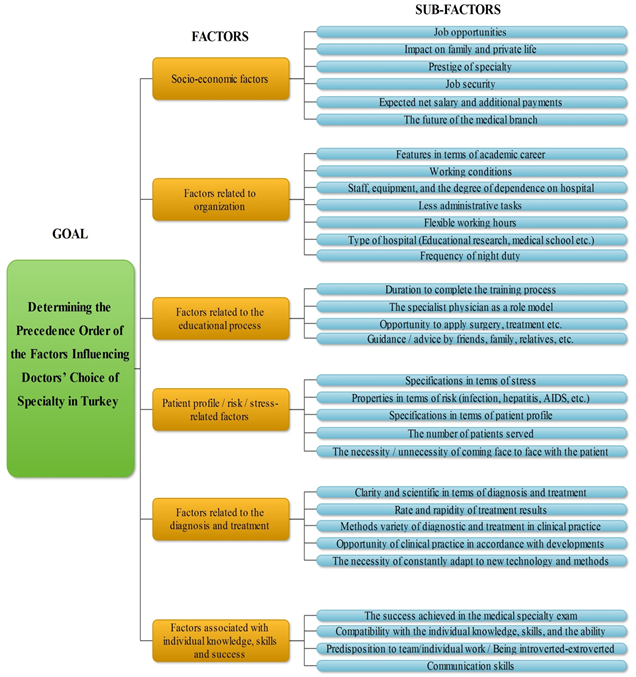 | Figure 3. Hierarchy of the model |
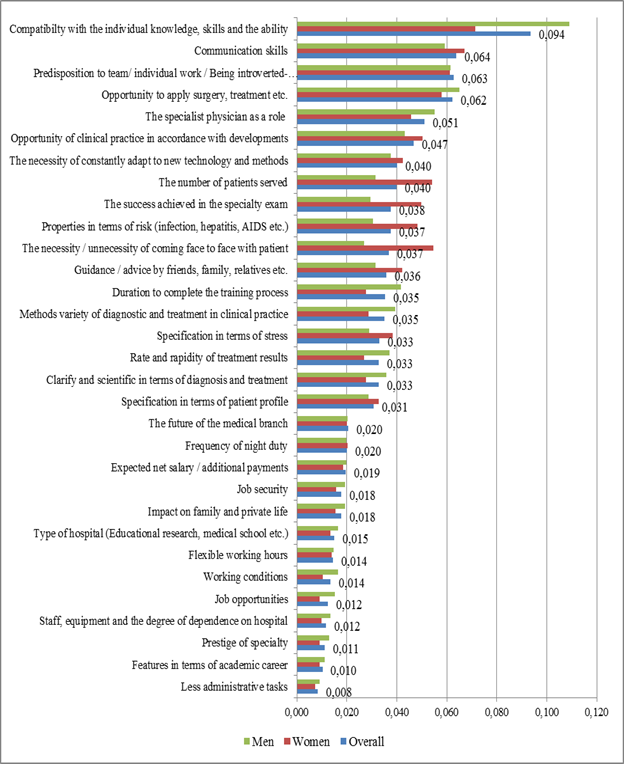 | Figure 4. Precedence order and the weights of the factors for all female specialists (Total: 57, Men: 33, Women: 24) |
|
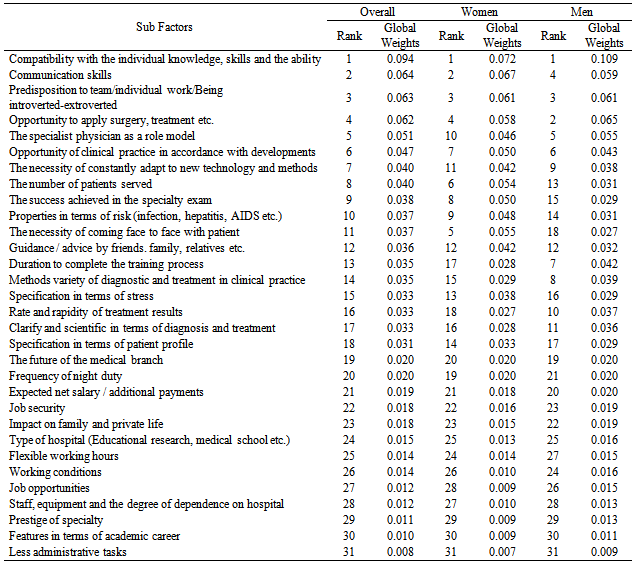
6. Conclusions and Suggestions
- Our findings indicate that, although “Compatibility with the individual knowledge, skills and the ability” factor is the most important influence in specialty choice for male doctors, “Factors related to the educational process” such as “Opportunity to apply surgery, treatment etc.” is also very important one. The overall priorities are shown at Table 10. There is a significant difference between male and female doctors for some criteria. ‘The number of patients served is more important factor for female doctors. Because of the fact that more patients means more stress and tiredness for female doctors. This factor can be ignored by male doctors due to their physical endurance. Besides this women are more influenced by domestic circumstances and hours of work and working conditions than male doctors. The findings of this study could provide a foundation for policy makers, university and hospital administrators in planning and developing strategies. Due to the use of a sample from several hospitals in Turkey, sampling bias exists in this study. Findings from this study cannot be generalized, suggesting that a further study is needed to confirm the preliminary findings using random sampling among all hospitals in Turkey. Also this study’s results can be used for recruitments efforts and development strategies of doctors facing the problem of a shortage.