Fatma Poni Mardiah , Mursyid Hasan Basri
School of Business and Management (SBM), Institute Technology Bandung (ITB), Bandung, 40132, Indonesia
Correspondence to: Fatma Poni Mardiah , School of Business and Management (SBM), Institute Technology Bandung (ITB), Bandung, 40132, Indonesia.
| Email: |  |
Copyright © 2012 Scientific & Academic Publishing. All Rights Reserved.
Abstract
Outpatient services have become an important component of health care. By hidebound thinking, the medical profession emphasized that a physician’s time is more valuable than a patient’s time. Consequently, the appointment system was designed to minimize physicians’ idle time overlooking patients’ waiting time. This is no longer valid in today’s consumer oriented society. Long waiting times for treatment in the outpatient department followed by short consultations has long been a complaint. Nowadays, customers use waiting time as a decisive factor in choosing a service provider. Therefore, idle time of both parties must be considered in designing an appointment system although these two objectives are contradicted to each other. This research aims to provide a study of the major causes of patients length of time for medical treatment in a outpatient clinic at one of Indonesian public hospital and also provide recommendation on the best strategy to improve the appointment system so that can maximize the effectiveness and efficiency of resource and capacity. The hospital queue model use single-channel multiphase systems. Queuing theory be the first tool to look at patient waiting times on each server independently. The results show that the hospital should change the appointment system for physicians. Applying ‘doctor on call’ system may appear to reduce doctor’s idle time but lead to high patients’ waiting times. In some cases, the appointment system make doctor to be back and forth to the hospital, so it was not directly affect the productivity of a doctor. Not only construct the appointment system, they should take attention of patient flow and set scheduling of the capacity to increase the effective and efficiency outpatient department performance.
Keywords:
Appointment System, Outpatient Waiting Time, Queue Theory
Cite this paper: Fatma Poni Mardiah , Mursyid Hasan Basri , The Analysis of Appointment System to Reduce Outpatient Waiting Time at Indonesia’s Public Hospital, Human Resource Management Research, Vol. 3 No. 1, 2013, pp. 27-33. doi: 10.5923/j.hrmr.20130301.06.
1. Introduction
Customer satisfaction has become a serious concern in service sector. On Healthcare industry, a number of initiatives have been introduced to enhance customer satisfaction. The healthcare industry providers globally are experiencing increasing pressure to concurrently reduce cost and improve the access and quality of care they deliver. Any healthcare institutions are confronted with long waiting times, delays, and queues of patients. Typical questions challenging hospital managers include: How should they optimally allocate their limited resources? How much exam rooms do they need? How much physicians and supporting staff do they need? If they increase or decrease the amount of exam rooms and/or staff, how would this effect patient waiting time, the length of a medical treatment and the total time spent in clinic by patient?To improve patient satisfaction, the performance of key processes has to be improved[1]. There is no doubt that healthcare institutions need to become high performers. If they increase or decrease the amount of exam rooms and/or staff, how would this effect patient waiting time, the length of a medical treatment and the total time spent in clinic by patient?. To improve patient satisfaction, the performance of key processes has to be improved[1]. There is no doubt that healthcare institutions need to become high performers.Practical issues such as the ease of use of the appointment system, or implications on modifying physicians’ behaviour need to be considered in order to achieve the ultimate goal of improving “real systems”. It may also be interesting to determine what are the most commonly used appointment system in practice. There is a lack of emphasis on the real-life performance of appointment system implemented as a result of studies. Discussions on implementation issues reveal how misleading it can be to view the problem as a “pure optimization” problem[2].Effectively managing patient flow in an outpatient unit is a key to achieving operational excellence as well as ensuring clinical quality. It is especially so for an outpatient department in a large hospital as it handles very large volume of patients with a diverse case mix.Based on data from the Ministry of Health, the number of hospitals in Indonesia has reached 1959 units in May 2012. That number could continue to grow in line with economic development. Public hospitals as many as 785 units and the others are private hospital. Although the number hospitals are large but there are still many people go for treatment to overseas, especially the upper classes. National hospital industry must consider what makes some people prefer to seek treatment to overseas.There is a need for more realistic representation of outpatient clinics. Effective appointment systems have the goal of matching demand with capacity so that resources are better utilized and patient waiting times are minimized. Patient waiting times and waiting-room congestion are two of the few tangible quality elements. Well-designed appointment systems have the potential to increase the utilization of expensive personnel and equipment-based medical resources as well as reducing waiting times for patients[2]. Hospital managers should therefore take steps to improve quality in these three aspects; appointment system, patient flow and capacity. The fact, many patients public hospital prefer to move to private hospital to do medical check up and treatment. Its means are the hospital management should be improved to increasing patient satisfaction.This study allows the hospital to notice what impact has the improvement do in the hospital performance. Moreover, this study will show what factors can be improved in the reducing patient waiting time. This research expected to bring new ideas and concept to be implemented in hospital in Indonesia, especially public hospital since the numbers of researches about this field are limited. Research question for this paper are:• How does the model of outpatient service and arrival pattern of patient in public hospital?• Is an existing outpatient service already fulfilling the minimum service standard of hospital?• What factors causing high outpatient waiting times?The objective of this paper is to investigate how does the model of outpatient waiting time and patient scheduling on Indonesia’s public hospital and find out the factors that causing the stack.
2. Service Operation in Healthcare Industry
Healthcare service is a patient-oriented service that requires continuous interaction with customers. It utilizes facilities and equipment, and consumes a large volume of nursing care. Therefore, it becomes increasingly important to healthcare executives to understand what kind of facility, equipment, and workforce decisions are critical to achieve the commonly acknowledged goal of providing quality health service at a reasonable cost[3]Until now research on operations strategy in Indonesian public hospitals has not been well developed, especially when it relates operations strategy to the current health service condition. Most of the operations-oriented studies focus narrowly on issues of hospital cost containment, capacity planning, or personnel scheduling[3].Healthcare management has evolved into a dynamic and complex field. This diverse industry is always changing due to scientific discoveries that bring significant contributions to improve the health standards of our communities. The changes have moved on to determine new ways about how and where healthcare is provided.Li et al.[3] found that the obvious differences in previous hospital research and current hospital practice in managing demand is that previous research tends to focus on a reactive approach to manage demand through internal improvement of facility utilization and better scheduling policies.Integrated Healthcare Management is the systematic application of processes and shared information to optimize the coordination of benefits and care for the healthcare consumer. Integration of healthcare management not only observes the relationship between customer (patients) and hospitals but also the inter-relationship between departments in the healthcare systems. This integrated management will support the effectiveness and efficiency of hospital. Hospital strategic planning can be performed at the corporate level by examining the hospital "system" which would include hospitals, HMOs, walk-in clinics, and other health-oriented businesses[4].
3. Outpatient Management
Outpatient services are gradually becoming an essential component in healthcare. The development of the times, technology and the rapid increase in population make the theories need to be developed. The objective of outpatient scheduling is to and an appointment system for which a particular measure of performance is optimized in a clinical environment—an application of resource scheduling under uncertainty. As seen as Figure 1, Cayirli and Veral[2] discussion about modelling of clinic environment.The underlying problem applies to a wide variety of environments, such as general practice patient scheduling, scheduling patients for hemodialysis, radiology scheduling, surgical scheduling, etc.
4. Queuing Theory
Queuing is an event where people or goods will undergo a process from the arrival queue; enter the queue, waiting, until the last service. Limits the length of the queue can be limited (limited) can also (unlimited), depending on the number of existing units in the system. Waiting line or queuing system is an items or people in a line awaiting service. The parts of a waiting line are: (a) Arrivals or inputs to the system: these have characteristic such as population size, behaviour, and statistical distribution. (b) Queuing discipline or waiting line itself: Characteristic of the queue include whether it is limited or unlimited in length and the discipline of people or items in it, for example FIFO. (c) The service facility: its characteristic includes its design and the statistical distribution of service time. There are four type of queuing model, which are single channel single phase system, single channel multiphase system; multiple channel single phase system and multiple channel multiple phase systems[5].
5. Factor That Influenced Outpatient Management
Appointment SystemThe term of “appointment” refer to the period of time allocated in the schedule to a particular patient’s visit and “service time” refer to the amount of time the physician actually spends with the patient (which may be shorter or longer than the appointment duration).[6]Based on Cayirli and Veral[2], Appointment scheduling can be classified into two broad categories:Static. All decisions must be made prior to the beginning of a clinic session, which is the most common appointment system in healthcareDynamic. The schedule of future arrivals are revised continuously over the course of the day based on the current state of the system. This is applicable when patient arrivals to the service area can be regulated dynamically, which generally involves patients already admitted to a hospital or clinic.The most primitive form of outpatient management is single block scheduling. The single block rule assigns all patients to arrive at the same time. The patients are served on a first come first serve basis. Another, nowadays more common, form of appointment scheduling is the individual block rule. Patients are assigned unique appointment times that are spaced throughout the clinical session.Manager should consider the factor that influenced on design appointment system. Figure 2 describe factors that influenced on design appointment system.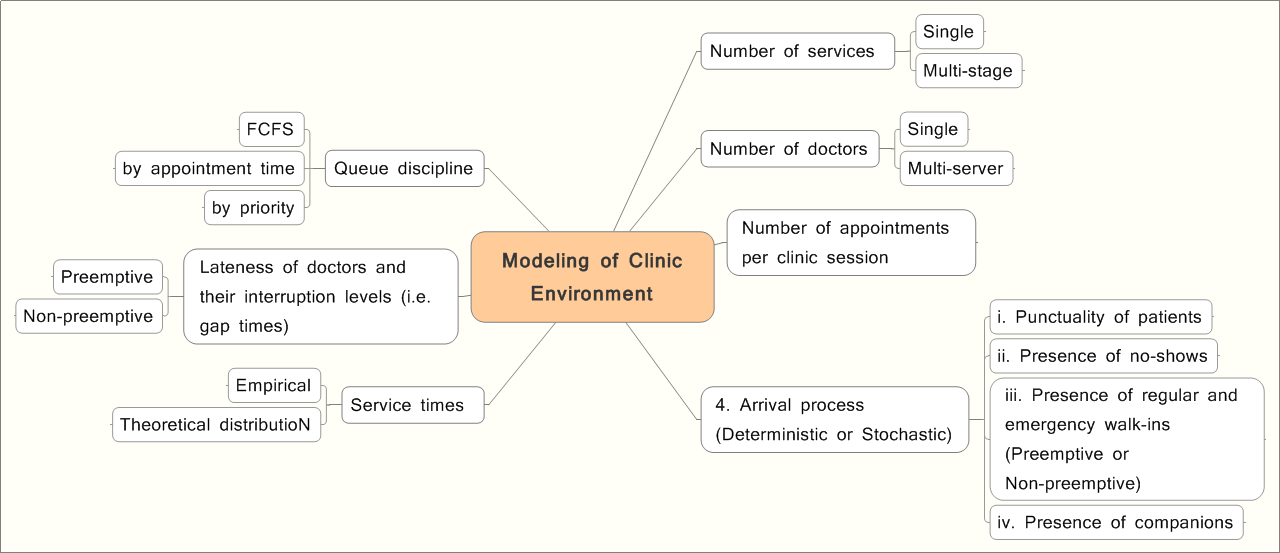 | Figure 1. Modelling of Clinic Environment[2] |
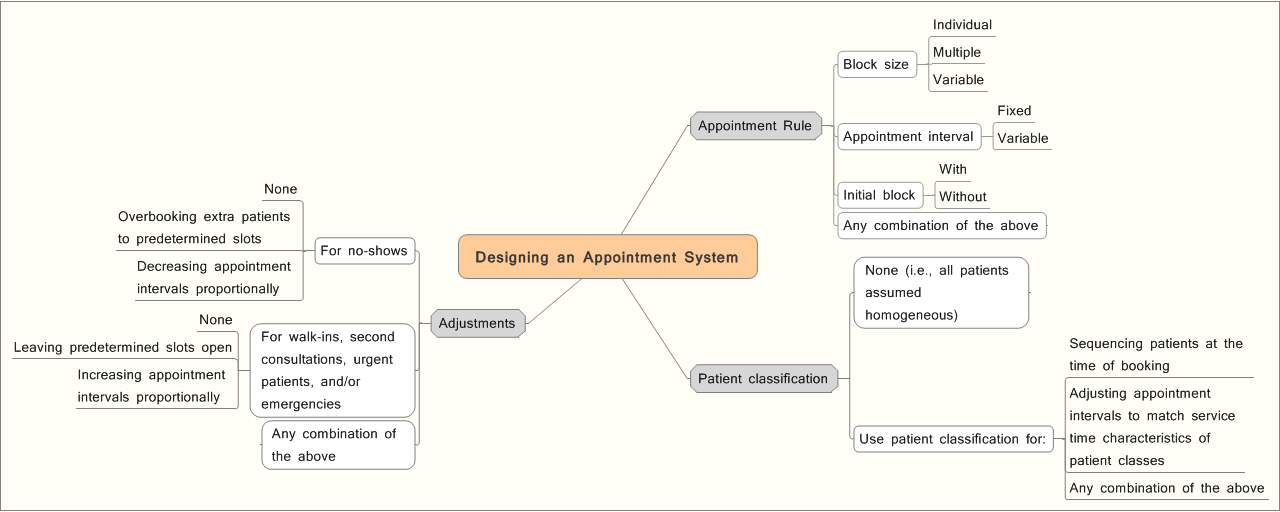 | Figure 2. Design of Appointment Systems[2] |
 | Figure 3. Patient Flows for Discharged Alive Coronary Patients (clinical) |
 | Figure 4. Patient Flows for Patients at a Family Practice Clinic (operational) |
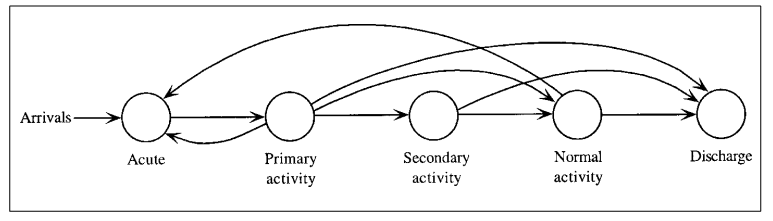
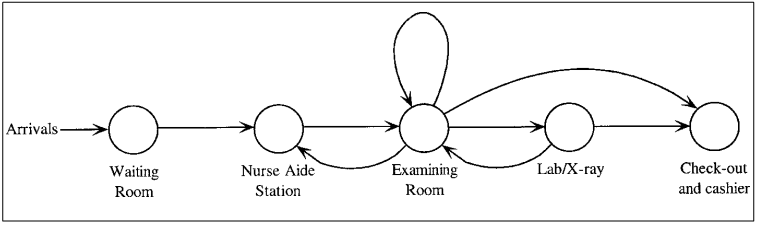
Patient FlowOne of the major elements in improving efficiency in the delivery of healthcare services is patient flow. From a clinical perspective, patient flow represents the progression of a patient’s health status. Patient flow management requires addressing three aspects of an outpatient unit: arrival of patients, service process, and queuing process. Working on the patient’s arrival includes controlling its patient panel size, balancing patient volumes across available sessions, and achieving desirable patient arrival pattern within a session[7].Based on Cote[8], Patient flow can be described by one of two complementary approaches: clinical or operational. Regardless of approach, all patient flows share four common characteristics: an entrance, an exit and the random nature of the healthcare elements.It will describe by the following figure:Figure 3 is an example of an inpatient medical condition and illustrates the possible recovery paths associated with a group of discharged alive coronary patients. In contrast, Figure 4 is an outpatient application of a family practice clinic’s patient-care episodes.In particular, resource planning, scheduling, and utilization are all affected by patient flows. Quantitative tools, like forecasting and queuing models, can help decision makers assess healthcare services in light of the patient flows. Queuing performance measures such as time in the system and traffic intensity have direct correspondence to the patient flow characteristics.
6. Methodology Research
6.1. Research Paradigm
This research is a positivist social science, because this study is research that emphasizes the legal phenomenon of cause and effect of a condition. The research is done by using the empirical observation made cautiously[9]. Research methodology used in this research is case study. Case study is research that is an in-depth examination of an extensive amount of information about very few units or cases for one period or across multiple periods of time[9].
6.2. Data Collection
This research is using interview to see the appointment system and the factor that effect patient waiting time. Initial interview was conducted with key informant in outpatient department to get information about general overview of outpatient system. After that, interview will be conduct to collect more data and information related to this study. The information will be used to how the model of outpatient service and arrival pattern of patient in public hospital.The field work pertaining to business process will be conduct. The observations include field visit to public hospital and to see directly outpatient service and arrival pattern of patient in public hospital.Secondary data will be collected from previous research that conducted by hospital, national and international journal to complete the information regarding outpatient waiting time and patient scheduling.
7. Data Calculation and Analysis
7.1. Descriptive Analysis
The hospital has two kinds ambulatory service. One service is general outpatient clinic that was treated by residency. The others is Specialist Outpatient Clinic that was treated by specialist (e.g internist, ophthalmologist, obstetrician). The study was conducted in Speciality Outpatient Clinic. This clinic has eleven specialists. They are: internal medicine, obstetrics and gynaecology, general surgery, orthopaedic, neurosurgery, dermatology and venereology, neurology, medical rehabilitation, pediatric, psychiatry and ophthalmology.Observations made during a month. After the observation, it was decided for data retrieval done on Monday and Tuesday, which is on the busy days of the week. The data used are the number of patient arrivals per specialist per day, arrival time of doctor and patient, length of registration service and the duration of examination.From one month of the observation, it was found the average number of patient per hour. From the Table 1, it shows the high arrival rate on Monday and Tuesday. Internal medicine always takes a large number of patients.| Table 1. The average number of patients per day |
| | Specialist | Mo | Tu | Wed | Thr | Fr | | Internal Medicine | 49 | 51 | 35 | 35 | 29 | | Obstetrics and gynecology | 19 | 17 | 20 | 17 | 15 | | General Surgery | 46 | 30 | 30 | 31 | 20 | | Orthopedic | 11 | 9 | 7 | 8 | 4 | | Neurosurgery | 7 | 4 | 1 | 3 | 2 | | Neurology | 15 | 8 | 13 | 10 | 5 | | Dermatology and Venereology | 12 | 7 | 11 | 9 | 7 | | Medical Rehabilitation | 1 | 0 | 2 | 1 | 0 | | Pediatric | 0 | 0 | 0 | 0 | 0 | | Psychiatry | 2 | 3 | 1 | 2 | 2 | | Ophthalmology | 1 | 0 | 1 | 0 | 0 |
|
|
Table 2 shows the time of patient arrivals. A large number of patients come between 08.00 am to 11.am. This condition thought to lead to a long patient waiting times. So, this research will focus on the busy hours. The patient arrival rate on busy hours is 30 people per hour. | Table 2. The average number of patients’ arrival per hours |
| | Time | num of patient/ day | | 1 (Mo) | 2 (Tu) | 3 (Mo) | 4 (Tu) | | < 07:59 | 3 | 0 | 5 | 5 | | 8:00 | : | 8:59 | 34 | 26 | 30 | 28 | | 9:00 | : | 9:59 | 38 | 25 | 47 | 27 | | 10:00 | : | 10:59 | 34 | 28 | 23 | 22 | | 11:00 | : | 11:59 | 14 | 16 | 19 | 17 | | 12:00 | : | 12:59 | 11 | 11 | 7 | 6 | | 13:00 | : | 13:59 | 5 | 5 | 3 | 4 | | > 14: 00 | 2 | 3 | 1 | 2 |
|
|
This Clinic has over 30 sub-specialists. The number of existing space is 10 rooms and 174 doctors. The highest level of patient arrival is at the beginning of each week. The clinic implements the single block system. The patient was not scheduled to come before. The physician appointment system is on call. The doctor comes when patients arrive. The problem of this system is the first patient will have a longer waiting time. Moreover utility of the room and the equipment is also a critical issue. The condition is compounded because the hospital has not yet allocate doctor schedule by room and type of disease. When the condition is all the doctor came at the same time, there is no empty room or all of the tools being used, so that both physician and patients have to wait even longer. At other times, the room become idle. The waiting time becomes higher because hospital did not allocate and well-scheduled their resources. The clinic has an effective operating time for six hours, but many patients accumulated at one time.Therefore this study would like to implement individual block schedule. By implementing an appointment system, the clinic is able to optimize the resources and capacity. Patients were also more likely to be served and patient satisfaction will increase. It does not mean to expect more people to be sick. The existing conditions, the number of patient are large compare to the hospital capacity. Consequently many patients run to private hospitals and even abroad for better treatment.
7.2. Appointment System
Existing appointment system which applied in this clinic is the single block rule. It assigns all patients to arrive at the same time. The patients are served on a first come first serve basis. The queue system is single channel multiple phase with two single server. The current queue model is M/M/1/I, which means the pattern is random arrival. The service pattern is also random that follows Poisson distribution. The number of facilities is only one with infinite population. It has waiting line in each server. The queue model will be shows as the figure below. | Figure 5. Queuing Model for Specialist Outpatient Clinic |
The detail of queue model can be seen from the following patient flow diagram.From the Figure 6, there are two type of patient on specialist outpatient clinic, one type is patient that already a member, and the other is patients that come for the first time. The new member need to pre-register on information desk by filled the registration form. There is no queue on information desk, so this server was not considered on this research. After registration, the patient is waiting for the treatment (next server). On the other hand, medical record staff will look for the patient record file. Time taken to search medical records is relatively shorter than patients waiting for the doctor. The patients will not go home. They still have another choice. It can be one, two or all three alternative; supporting treatment, cashier, or pharmacy.
7.3. Outpatient Waiting Time
The ambulatory facilities are designed to make more effective use of patients' and doctors' time. The queuing formula for model single channel system that used was: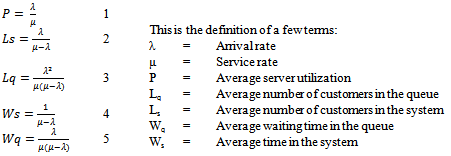 Based on calculation for first server using one month daily data, the table below was the result. The average time need on waiting for the patient is 0.3hours, or 18minutes. Table 4 show the condition on three specialists; internal medicine general surgery and obstetrics & gynecology. This calculation didn’t consider the capacity of the room. Internal medicine has a higher waiting time. It is about 0.54hours or 33minutes. General Surgery has 14 minutes and obstetrics & gynecology has 9minutes.From two tables above, it can be predict the patient waiting time ranged between 27-51minutes. Based on the minimum standards of hospital care, outpatient waiting times should be less than 30 minutes. This time is calculated from the first patient enrolled until physician served. Since the calculation of the patient's waiting time separately (not considering doctor arrival time), the waiting time of patients still within reasonable limits. In fact, there are even patients who have to wait more than three hours. The main causes of long waiting times patients are physicians who are not available any time.
Based on calculation for first server using one month daily data, the table below was the result. The average time need on waiting for the patient is 0.3hours, or 18minutes. Table 4 show the condition on three specialists; internal medicine general surgery and obstetrics & gynecology. This calculation didn’t consider the capacity of the room. Internal medicine has a higher waiting time. It is about 0.54hours or 33minutes. General Surgery has 14 minutes and obstetrics & gynecology has 9minutes.From two tables above, it can be predict the patient waiting time ranged between 27-51minutes. Based on the minimum standards of hospital care, outpatient waiting times should be less than 30 minutes. This time is calculated from the first patient enrolled until physician served. Since the calculation of the patient's waiting time separately (not considering doctor arrival time), the waiting time of patients still within reasonable limits. In fact, there are even patients who have to wait more than three hours. The main causes of long waiting times patients are physicians who are not available any time.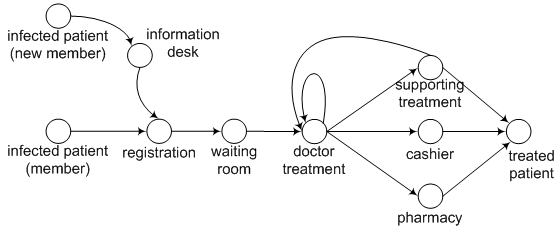 | Figure 6. Patient Flows for Specialist outpatient Clinic |
| Table 3. Calculation Result for First Server |
| | | Registration | | Arrival rate (λ) | 27 | | Service rate (μ) | 30 | | Average server utilization(P) | 0.90 | % | | Average number of customers in the queue(Lq) | 8.10 | people | | Average number of customers in the system(Ls) | 9 | peoples | | Average waiting time in the queue(Wq) | 0.30 | hours | | Average time in the system(Ws) | 0.33 | hours | | Probability (% of time) system is empty (P0) | 0.10 | % |
|
|
| Table 4. Calculation Result for Second Server (medical treatment) |
| | | Internal Medicine | General Surgery | Obstetrics & gynecology | | Arrival rate (λ) | 6.5 | 5.2 | 2.8 | | Service rate (μ) | 8 | 8 | 6 | | (P) | 0.81 | 0.65 | 0.47 | % | | (Lq) | 3.52 | 1.18 | 0.42 | people | | (Ls) | 4.33 | 1.82 | 0.89 | peoples | | (Wq) | 0.54 | 0.23 | 0.15 | hours | | (Ws) | 0.67 | 0.35 | 0.32 | hours | | (P0) | 0.19 | 0.35 | 0.53 | % |
|
|
8. Conclusions and Future Research
Based on the problem of specialist outpatient clinic which is about the length of patient waiting time and it impacts to the performance of the hospital that become the reason of this study. This research provides suggestion to the hospital to construct the appointment system, take attention of patient flow and set scheduling of the capacity to increase the effective and efficiency outpatient department performance. The most suitable appointment system for outpatient is using no-show. The condition that affect patient waiting times are the physician come on call, go show patient, no proper calculation of the room capacity, the number of physicians and the number of sub-specialists. This research is a preliminary study that analyzed each variable separately. Analysis was performed to confirm that the waiting time targets not met the minimum service standard of hospital.Research continues as intended by examining all variables simultaneously. These variables are appointment system (patient scheduling), patient flow, capacity and behaviour of the physician. For the future, further analysis is still required to design this system such as make a simulation of all variable that affects bottleneck and it supposed to make the clinic performance more effective and efficient.
ACKNOWLEDGEMENTS
We would like to express our sincere gratitude to the hospital’s staff who provides assistance and information during field visits and interviews. We would like to express our thanks to the anonymous reviewers who provided valuable comments to improve this paper.
References
| [1] | Torres, J.E. and Guo, K.L. (2004) : Quality improvement techniques to improve patient satisfaction. International Journal of Health Care Quality Assurance, 17 (6), 334-338. |
| [2] | Cayirli, Tugba & Emre Veral (2003) : Outpatient Scheduling in Healthcare, Production and Operation Management, vol 12(4) |
| [3] | Li, Ling X., W.C. Benton, and G. Keong Long (2002) : The Impact of Strategic Operations Management Decisions on Community Hospital Performance. Journal of Operations Management 20: 389-408 |
| [4] | Butler, Timothy W., G. Keong Leong & Linda N. Everett (1996) : The Operations Management Role in Hospital Strategic Planning , Journal of Operations Management 14 (137-156) |
| [5] | Heizer, Jay and Barry Render (2008) : Operationts Management, Ninth Edition, Prentice Hall |
| [6] | White, Denis L., Craig M.Froehle, Kenneth J. Klassen (2011) : The Effect of Integrated Schedulling and Capacity Policies on Clinical Efficiency. Production and Operation Management, vol 20(3), pp442-455 |
| [7] | Yeon, N., Taesik Lee & Hoon Jang (2010) : Outpatient Appointment Scheduling with Multi-Doctor sharing Resources. Proceedings of the 2010 Winter Simulation Conference |
| [8] | Cote, Murray J. (2000) : Understanding Patient Flow, Decision Line, March |
| [9] | Neuman, W. L. (2006). Social Research Methods: Qualitative and Quantitative Approaches. Sixth Edition Boston: Allyn and Bacon |
| [10] | Cayirli, Tugba, Emre Veral & Harry Rosen (2008) : Assessment of Patient Classification in Appointment System Design, Production and Operation Management, vol 17(3), pp338-353 |
| [11] | Chand, S., Herbert Moskowitz, John B. Norris, Steve Shade & Deanna R. Willis (2009) : Improving Patient Flow at an Outpatient Clinic, Healthcare Management Science 12, pp325-340 |
| [12] | Fomundam, Samuel F. & Jeffrey W.Herrmann (2007) : A survey of Queuing Theory Applications in Healthcare, ISR Technical Report |
| [13] | Goldstein, S.M., et al. (2002) : The Effect of Location, Strategy, and Operations Technology on Hospital Performance. Journal of Operations Management 20, 63-75. |
| [14] | Santibanez, P., Vicent Chow, John French, Martin Puterman & Scott Tyldesley (20xx) : Reducing Patient Wait Times and Improving Resources Utilization at BCCA's Ambulatory Care Unit through Simulation, CIHR Team in Operations Research for Improved Cancer Care |
| [15] | Singh, Vikas (2006) : Use of Queuing Models in Healthcare, Departement of Health Policy and Management, University of Arkansas for Medical Sciences |
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML