-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
Journal of Health Science
p-ISSN: 2166-5966 e-ISSN: 2166-5990
2026; 14(1): 6-13
doi:10.5923/j.health.20261401.02
Received: May 6, 2026; Accepted: May 25, 2026; Published: Jun. 1, 2026

From Monitoring to Quality: How Surveillance Systems Shape Indigenous Medicine in Kajiado and Tharaka Nithi Counties
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLJulius Kaluai1, Wanja Tenambergen2, Carol Kawila Kyalo1
1Department of Health Systems Management, Kenya Methodist University, Kenya
2Riara University, Kenya
Correspondence to: Julius Kaluai, Department of Health Systems Management, Kenya Methodist University, Kenya.
| Email: |  |
Copyright © 2026 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Indigenous medicine remains widely utilized in Kenya despite persistent concerns regarding its safety, consistency, and quality. Pharmacovigilance surveillance systems are intended to facilitate adverse drug reaction reporting, safety monitoring, and regulatory responsiveness; however, their operational effectiveness within indigenous medicine systems remains inadequately understood. This study examined the influence of pharmacovigilance surveillance systems on the quality of indigenous medicine in Kajiado and Tharaka Nithi Counties, Kenya. Guided by Regulatory Compliance Theory, the Health Belief Model, and Diffusion of Innovations Theory, the study adopted a convergent mixed-methods research design. Quantitative data were collected from 334 respondents drawn from regulators, community health promoters, indigenous medicine practitioners, and manufacturers/suppliers, while qualitative data were obtained through key informant interviews and focused group discussions involving indigenous medicine users. Quantitative data were analysed using descriptive statistics and multiple logistic regression, while qualitative data were analysed thematically. The findings revealed that adequate pharmacovigilance surveillance systems significantly increased the likelihood of achieving good-quality indigenous medicine (OR = 2.37, 95% CI [1.37, 4.10], p = .002). However, descriptive and qualitative evidence demonstrated that surveillance systems remain weakly institutionalised, characterised by unclear reporting pathways, inconsistent adverse drug reaction reporting, weak feedback mechanisms, and limited stakeholder integration. Qualitative findings further showed that adverse reactions are frequently managed informally at practitioner or household level without systematic documentation or escalation to regulatory authorities. The study concludes that pharmacovigilance surveillance systems have substantial potential to improve the safety and quality of indigenous medicine, but their effectiveness is constrained by structural and behavioural limitations that weaken reporting and system responsiveness. The findings extend Regulatory Compliance Theory and the Health Belief Model by demonstrating that effective pharmacovigilance depends not only on institutional structures but also on stakeholder awareness, trust, and reporting behaviour. The study recommends strengthening reporting infrastructure, institutionalising feedback mechanisms, enhancing stakeholder coordination, and integrating indigenous medicine actors into formal pharmacovigilance systems to improve medicine safety and public health outcomes in Kenya.
Keywords: Pharmacovigilance, Surveillance Systems, Indigenous Medicine, Quality, Adverse Drug Reactions, Kenya, Health Systems Strengthening
Cite this paper: Julius Kaluai, Wanja Tenambergen, Carol Kawila Kyalo, From Monitoring to Quality: How Surveillance Systems Shape Indigenous Medicine in Kajiado and Tharaka Nithi Counties, Journal of Health Science, Vol. 14 No. 1, 2026, pp. 6-13. doi: 10.5923/j.health.20261401.02.
Article Outline
1. Introduction
- Indigenous medicine continues to play a central role in healthcare delivery across many low- and middle-income countries, particularly in sub–Saharan Africa where it remains a primary source of treatment for a substantial proportion of the population. The World Health Organization estimates that a large percentage of people in developing countries rely on traditional and indigenous medicine for primary healthcare due to its accessibility, affordability, cultural acceptability, and perceived effectiveness [1]. In Kenya, the utilization of indigenous medicine remains widespread, especially in rural and underserved areas where access to formal healthcare services is often limited. Indigenous medicine therefore constitutes an important but largely informal component of the national healthcare system [2].Despite its widespread utilization, concerns regarding the safety, consistency, and quality of indigenous medicine continue to attract growing scholarly and policy attention. Unlike conventional pharmaceutical products, many indigenous medicines are prepared, dispensed, and consumed through informal processes that are rarely subjected to standardized manufacturing, quality assurance, or regulatory evaluation. This situation creates risks associated with contamination, dosage inconsistencies, poor storage conditions, uncertain efficacy, and adverse drug reactions. Existing studies have documented persistent challenges involving weak quality control systems, inadequate safety monitoring, and limited documentation of adverse effects associated with herbal and traditional medicine products [3,4]. These risks are further compounded by weak regulatory oversight and limited integration of indigenous medicine into formal healthcare and pharmacovigilance systems [5].Pharmacovigilance surveillance systems provide an important institutional mechanism for improving medicine safety and quality by facilitating the detection, reporting, assessment, and prevention of adverse drug reactions and medicine related risks. Effective surveillance systems support evidence based decision making, strengthen regulatory responsiveness, and enhance public confidence in healthcare systems. Their importance is particularly pronounced within indigenous medicine contexts where variability in preparation practices and informal distribution channels increase the likelihood of unreported adverse events and inconsistent product quality. Previous studies have shown that robust pharmacovigilance systems contribute significantly to medicine safety through early detection of safety signals, coordinated stakeholder engagement, and strengthened reporting structures [6–8].However, pharmacovigilance systems in many low resource settings remain fragmented and underdeveloped, particularly in relation to indigenous medicine. In Kenya, adverse drug reaction reporting within indigenous medicine systems remains limited due to unclear reporting pathways, inadequate stakeholder coordination, low reporting culture, and weak feedback mechanisms. Many practitioners and community level actors lack sufficient awareness, training, and incentives to participate in formal pharmacovigilance processes. Similar challenges have been reported across several African countries where underreporting, poor system integration, and weak institutional coordination continue to undermine pharmacovigilance effectiveness [9,7]. The absence of functional surveillance systems limits the generation of reliable safety data required for regulatory action and quality improvement [10].These challenges are particularly evident in Kajiado and Tharaka Nithi Counties where indigenous medicine remains deeply embedded within community healthcare practices. In these settings, adverse reactions associated with indigenous medicine are often managed informally at household or practitioner level without systematic documentation or escalation to regulatory authorities. The limited integration between indigenous medicine practitioners, community health actors, and formal regulatory institutions weakens information flow and constrains effective safety monitoring. Consequently, concerns regarding medicine quality, patient safety, and accountability continue to persist within the indigenous medicine sector.Although pharmacovigilance systems have been extensively studied within conventional pharmaceutical settings, limited empirical attention has been directed toward understanding how surveillance systems influence the quality of indigenous medicine in low resource African contexts. Existing studies have largely focused on regulatory challenges, utilization patterns, and adverse drug reaction reporting practices, with limited emphasis on how surveillance structures directly shape medicine quality outcomes. In Kenya, evidence linking pharmacovigilance surveillance systems to the quality and safety of indigenous medicine remains particularly limited despite the widespread reliance on traditional healthcare practices [2]. Furthermore, few studies have integrated quantitative and qualitative evidence to examine how reporting systems, stakeholder coordination, and feedback mechanisms influence surveillance effectiveness within indigenous medicine contexts. This knowledge gap limits the ability of policymakers and regulators to design context sensitive interventions for strengthening pharmacovigilance systems and improving indigenous medicine quality.This study therefore examined the influence of pharmacovigilance surveillance systems on the quality of indigenous medicine in Kajiado and Tharaka Nithi Counties, Kenya. The study sought to generate empirical evidence on how reporting mechanisms, stakeholder coordination, and surveillance practices shape medicine quality outcomes within indigenous medicine systems. By integrating quantitative and qualitative evidence, the study provides a comprehensive understanding of the operational effectiveness of pharmacovigilance surveillance systems and their implications for medicine safety, quality assurance, and health system strengthening.The study was informed by Regulatory Compliance Theory, the Health Belief Model, and Diffusion of Innovations Theory. Regulatory Compliance Theory explains how adherence to reporting procedures, regulatory standards, and surveillance guidelines influences the effectiveness of pharmacovigilance systems. The Health Belief Model provides insight into how perceptions of risk, perceived severity of adverse reactions, and perceived benefits of reporting influence reporting behaviour among practitioners, patients, and community health actors. Diffusion of Innovations Theory complements these perspectives by explaining how pharmacovigilance practices, reporting mechanisms, and surveillance innovations are adopted and integrated within indigenous medicine systems and community health networks [11]. Collectively, these theories provide a multidimensional framework for understanding the behavioural, institutional, and systemic factors that shape surveillance effectiveness and medicine quality outcomes.
2. Methodology
- This study adopted a convergent mixed methods research design to facilitate the simultaneous collection and integration of quantitative and qualitative data in examining the influence of pharmacovigilance surveillance systems on the quality of indigenous medicine. The mixed methods approach was considered appropriate because it enabled triangulation of findings and provided both statistical and contextual understanding of surveillance system effectiveness within indigenous medicine settings [12,13].Study settingThe study was conducted in Kajiado and Tharaka Nithi Counties, Kenya, where indigenous medicine remains widely practiced alongside formal healthcare systems. The two counties were purposively selected because of the widespread utilization of indigenous medicine, the presence of diverse stakeholder groups involved in indigenous medicine practice, and the increasing policy interest in strengthening pharmacovigilance and medicine safety systems within community healthcare settings.Target Population and Sampling ProcedureThe study targeted key stakeholders involved in indigenous medicine systems, including regulators, community health promoters, indigenous medicine practitioners, manufacturers, suppliers, and indigenous medicine users. A stratified sampling approach was adopted to ensure representation across the various stakeholder categories. Within each stratum, respondents were selected using simple random sampling procedures based on available stakeholder lists obtained from county health departments and relevant associations.The quantitative component consisted of 334 respondents drawn from the identified stakeholder groups. The qualitative component involved indigenous medicine users selected purposively based on their experiences with indigenous medicine utilization and related medicine safety concerns.Data Collection Instruments and ProceduresQuantitative data were collected using a structured questionnaire administered by trained research assistants. The questionnaire captured information relating to pharmacovigilance surveillance systems, including adverse drug reaction reporting mechanisms, reporting channels, stakeholder coordination, feedback systems, and perceptions regarding the safety and quality of indigenous medicine.Qualitative data were collected through semi structured interview guides and focused group discussions designed to explore participants’ experiences, perceptions, and challenges associated with pharmacovigilance surveillance systems and indigenous medicine quality[14]. Two focused group discussions were conducted in each county, resulting in a total of four focused group discussions across the study sites. Each focused group discussion comprised 12 indigenous medicine users selected purposively based on their experience with indigenous medicine utilization and related safety concerns.The focused group discussions explored participants’ experiences with adverse drug reactions, reporting practices, follow up mechanisms, practitioner responses to medicine related complaints, and perceptions regarding the safety and quality of indigenous medicine. The discussions also examined participants’ awareness of pharmacovigilance processes and the extent to which adverse events are formally reported within community settings.All interviews and focused group discussions were conducted physically within the study locations by trained research personnel. Participants were informed about the purpose of the study prior to participation, and consent was obtained before data collection commenced. Responses were audio recorded with participants’ permission and supplemented with field notes to enhance completeness and contextual interpretation of the qualitative data.Measurement of variablesThe dependent variable, quality of indigenous medicine, was operationalized using seven five-point Likert scale items assessing safety, consistency, perceived effectiveness, handling practices, user satisfaction, reliability, and perceived quality outcomes associated with indigenous medicine. Responses were rated on a five-point Likert scale ranging from 1 = strongly disagree to 5 = strongly agree. Composite scores were generated by summing responses across the seven items, resulting in a minimum possible score of 7 and a maximum possible score of 35. Respondents with composite scores ranging from 7 to 21 were categorized as having poor quality indigenous medicine, while those with composite scores above 21 were categorized as having good quality indigenous medicine for purposes of binary logistic regression analysis.The independent variable, pharmacovigilance surveillance systems, was measured using seven five-point Likert scale items assessing adverse drug reaction reporting systems, consistency of reporting, availability of reporting channels, feedback mechanisms, stakeholder coordination, follow up procedures, and system responsiveness. Responses were rated on a five-point Likert scale ranging from 1 = strongly disagree to 5 = strongly agree. Composite scores were generated by summing responses across the seven items, resulting in a minimum possible score of 7 and a maximum possible score of 35. Respondents with composite scores ranging from 7 to 21 were categorized as having inadequate pharmacovigilance surveillance systems, while those with composite scores above 21 were categorized as having adequate pharmacovigilance surveillance systems for purposes of binary logistic regression analysis.Data Quality AssuranceTo ensure validity and reliability of the instruments, the questionnaire and interview guides were pre tested in a setting with characteristics similar to the study area. Feedback obtained during pre-testing informed refinement of the instruments. Content and face validity were assessed through expert review by specialists in public health, pharmacovigilance, and health systems research. Reliability of the quantitative instrument was assessed using Cronbach’s alpha coefficient. Research assistants were trained prior to data collection to ensure consistency in administration of the instruments and adherence to ethical procedures.Data analysisQuantitative data were analysed using Statistical Package for Social Sciences version 26. Descriptive statistics including frequencies, percentages, means, and standard deviations were used to summarize the study findings. Binary logistic regression analysis was used to determine the influence of pharmacovigilance surveillance systems on the quality of indigenous medicine. Odds ratios and corresponding p values were used to determine the statistical significance and direction of relationships between the study variables at 0.05 level of significance.Qualitative data were transcribed verbatim and analysed thematically. The analysis involved familiarization with the data, coding of responses, identification of categories, and development of emerging themes relevant to pharmacovigilance surveillance systems and indigenous medicine quality [14]. Qualitative findings were integrated with quantitative results during interpretation to provide contextual understanding and triangulation of findings.Ethical considerationsEthical approval for the study was obtained from the Kenya Methodist University Scientific Ethics and Research Committee. A research permit was also obtained from the National Commission for Science, Technology and Innovation, Kenya. Permission to conduct the study was sought from relevant county authorities. Participants were informed about the purpose of the study and written informed consent was obtained prior to participation. Confidentiality and anonymity of participants were maintained throughout the study and participation remained voluntary.
3. Results
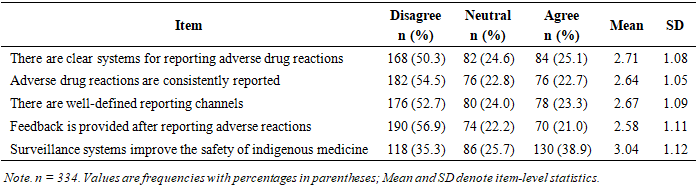
- The descriptive findings in Table 3.1 show a fairly weak and underperforming pharmacovigilance surveillance systems, particularly in relation to the reporting and follow-up of adverse drug reactions (ADRs).
3.1. Demographic Characteristics of Respondents
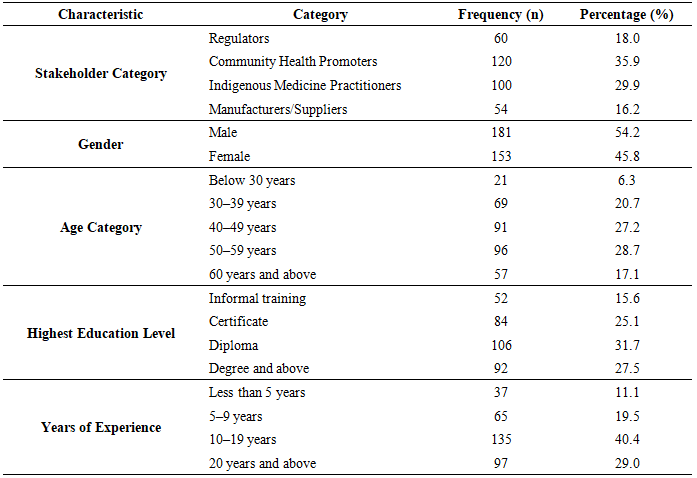
- Table 3.1 presents a summary of the demographic characteristics of quantitative respondents included in the study, excluding patients who participated only as qualitative key informants. The table summarizes the respondent distribution by stakeholder category, gender composition, age profile, educational attainment, and years of professional experience. These characteristics are important in contextualizing respondents’ experiential knowledge, institutional exposure, and capacity to engage in pharmacovigilance practices and quality control processes within indigenous medicine systems.
|
|
|
4. Discussion
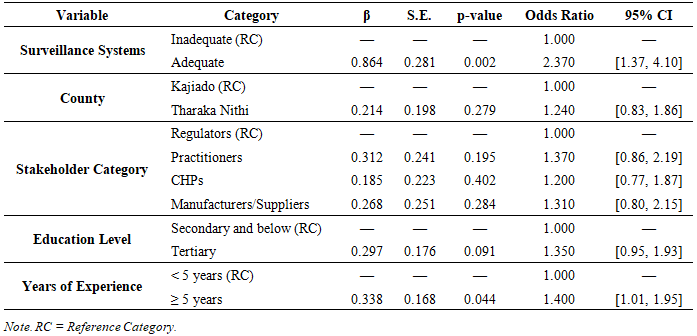
- The findings of this study provide robust empirical evidence that pharmacovigilance surveillance systems play a critical role in shaping the quality of indigenous medicine. The results demonstrate that adequate surveillance systems significantly increase the likelihood of achieving good-quality indigenous medicine, even after controlling for socio-demographic and professional characteristics. This indicates that surveillance system functionality is an independent and reliable determinant of quality outcomes within indigenous medicine contexts.These findings are consistent with existing literature, which identifies pharmacovigilance systems as essential mechanisms for enhancing medicine safety and quality. The World Health Organization emphasises that effective surveillance systems facilitate the detection, reporting, and prevention of adverse drug reactions, thereby enabling timely regulatory action [14]. Similarly, pharmacovigilance systems strengthen safety signal detection and support evidence-based regulatory decisions [8], while surveillance systems contribute directly to quality assurance by identifying contamination, dosage inconsistencies, and unsafe preparation practices [13].The present study extends these insights by providing empirical evidence that such mechanisms are equally critical within indigenous medicine systems, where variability in preparation and use amplifies safety risks.However, the descriptive and qualitative findings reveal a critical gap between system potential and operational reality. While the regression results indicate a strong positive effect of surveillance systems on quality, the descriptive evidence shows that these systems remain weakly institutionalised and inconsistently implemented in practice. Low reporting rates, unclear reporting pathways, absence of feedback mechanisms, and limited stakeholder integration indicate that the pharmacovigilance cycle is incomplete. This disconnect suggests that the observed statistical relationship reflects the inherent effectiveness of surveillance systems rather than their current operational performance.Qualitative evidence provides further insight into the mechanisms underlying these findings. Participants consistently reported that adverse drug reactions are managed informally at the practitioner or household level without formal reporting or escalation. As one participant explained, “when a medicine causes problems, the healer just changes it or tells you to stop, but there is no reporting to anyone else” (Patient 11). Similarly, another respondent observed that “the practitioner listens but there is no place they report these problems to” (Patient 14). These accounts demonstrate a fundamental breakdown in the transition from experiential recognition of harm to formal pharmacovigilance action. In addition, the absence of feedback mechanisms further undermines system effectiveness, as reflected in the observation that “once the medicine is sold, nobody follows up even if people complain” (Patient 22). Such patterns indicate that surveillance systems are not functioning as integrated, learning-oriented systems capable of generating, transmitting, and utilising safety information.The significance of years of experience as a predictor of quality outcomes further underscores the importance of knowledge and practice-based competence in pharmacovigilance processes. More experienced stakeholders are more likely to possess a deeper understanding of preparation practices, safety risks, and informal monitoring mechanisms, which may contribute to improved quality outcomes. This finding aligns with existing research indicating that awareness, training, and experiential knowledge significantly influence pharmacovigilance reporting behaviour and system effectiveness [10,6].From a theoretical perspective, the findings provide empirical support for both Regulatory Compliance Theory and the Health Belief Model. Regulatory Compliance Theory suggests that adherence to safety and quality standards is shaped by the presence of effective monitoring and enforcement mechanisms. The observed influence of surveillance systems on quality outcomes confirms that institutional structures play a decisive role in shaping compliance behaviour. At the same time, the Health Belief Model highlights the importance of behavioural factors, including awareness, perceived benefits of reporting, and trust in the system. The weak reporting culture observed in this study indicates that these behavioural determinants remain insufficiently addressed, thereby limiting the effectiveness of pharmacovigilance systems.The findings also carry important implications for health systems strengthening. In contexts where indigenous medicine remains a primary source of healthcare, pharmacovigilance systems must be adapted to reflect the realities of informal and culturally embedded practices. This requires the development of inclusive and context-sensitive approaches that integrate traditional practitioners, community health actors, and patients into formal safety monitoring processes. Strengthening reporting systems, institutionalising feedback mechanisms, and improving stakeholder coordination are therefore essential for enhancing system functionality.The findings indicate that improving the quality of indigenous medicine is not solely a function of establishing surveillance systems, but of ensuring their functional integration and active utilisation. This underscores the need for interventions that simultaneously strengthen institutional structures, enhance stakeholder coordination, and promote community-level engagement.
5. Conclusions and Implications
- Pharmacovigilance surveillance systems play a statistically significant and substantively important role in shaping the quality of indigenous medicine. The findings demonstrate that functional surveillance systems significantly increase the likelihood of achieving good-quality indigenous medicine, thereby confirming their central role as quality assurance mechanisms. This effect remains robust even after controlling for socio-demographic and professional characteristics, indicating that surveillance system adequacy is an independent determinant of quality outcomes.However, the descriptive and qualitative findings reveal that the current operational performance of these systems remains limited. Weak reporting structures, absence of clearly defined reporting pathways, ineffective feedback mechanisms, and poor stakeholder integration constrain the ability of pharmacovigilance systems to function as intended. These limitations are not merely procedural gaps but reflect deeper structural weaknesses that prevent the generation, transmission, and utilisation of safety information.From a theoretical perspective, the findings extend the application of Regulatory Compliance Theory and the Health Belief Model by demonstrating that the effectiveness of pharmacovigilance systems depends not only on institutional structures but also on behavioural and perceptual factors. In particular, awareness, perceived benefits of reporting, and trust in the system emerge as critical conditions for effective pharmacovigilance practice.From a policy perspective, the results underscore the need to shift focus from the mere existence of surveillance systems to their functional integration and operational effectiveness. Strengthening pharmacovigilance systems in indigenous medicine contexts requires the development of clear and accessible reporting mechanisms, institutionalisation of feedback loops, and enhanced coordination among stakeholders. In addition, targeted capacity building and community engagement are necessary to improve reporting behaviour and system responsiveness.Practically, these findings suggest that improving surveillance system functionality has the potential to significantly enhance the safety and quality of indigenous medicine. Given the widespread reliance on indigenous medicine in Kenya, strengthening pharmacovigilance systems is not only a regulatory priority but also a critical public health intervention.Finally, the study acknowledges that the findings are based on evidence from Kajiado and Tharaka Nithi Counties, which represent specific socio-cultural contexts. As such, caution should be exercised in generalising the results to other settings without considering contextual differences in indigenous medicine practices and health system structures.